




Published in:
01-11-2016 | Urology – Letter to the Editor
Retroperitoneal metastatic germ cell tumor presenting as a psoas abscess: a rare clinical occurrence and review of the literature
Published in: International Urology and Nephrology | Issue 11/2016
Login to get accessExcerpt
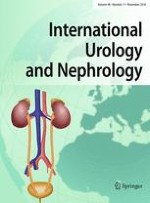
A 25-year-old man with a history of IV drug abuse presented to our emergency department complaining of fluctuating back and right flank pain. The pain did not improve and he stated the only thing that helped the pain was lying on his side or flexing his knees. He also showed symptoms of shortness of breath, bloated abdomen as well as onset of shaking and chills. On physical examination, he demonstrated a diffusely enlarged right testicle with vital signs significant for fever (38.9 °C, 102.0 °F). His laboratory workup showed the following results: White blood cell count was 19.76 × 103 cells per microliter, serum alkaline phosphatase level of 407 international units per liter, beta-HCG level of 4 milli-international units per milliliter, lactate dehydrogenase level of 700 units per liter and negative alpha-fetoprotein level at 0.5 micrograms per liter. Blood cultures were obtained at the time of presentation. A computed tomography (CT) scan showed a 6.4-cm × 7.5-cm × 9.1-cm peripherally enhancing mass with central hypodensity in the right retroperitoneal region. The differential diagnosis of the CT scan findings was retroperitoneal tumor/metastatic adenopathy with central necrosis, retroperitoneal abscess or a combination of both (Fig. 1). A chest CT showed a right hilar mass measuring 1.9 cm in diameter and prominent lymph nodes in the superior mediastinum with the largest measuring 1.3 cm in diameter. His bone scan was negative.
Fig. 1
Abdominal computerized tomography shows mass in right retroperitoneal region with central necrosis
× ![]()
…