




Published in:
01-12-2015 | Images in CV Applications
Exercise echocardiography in asymptomatic severe aortic stenosis
Published in: The International Journal of Cardiovascular Imaging | Issue 8/2015
Login to get accessExcerpt
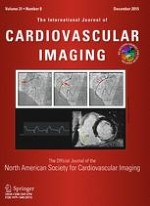
A 77 year old female with asymptomatic severe aortic stenosis (AS) and normal LV systolic function was referred for exercise stress echocardiography (ESE) in order to assess whether she is truly asymptomatic and to risk-stratify her aortic valve disease. While she only developed minimal breathlessness after 4.2 min of Bruce protocol and no other high risk features (arrhythmias, SBP drop, mean Aortic gradient rise >20 mmHg) [1], it was noted that her stroke volume (SV/indexed SVi) and flow rate (FR) at peak stress had dropped compared to the ones at rest (SVi rest = 45.7 ml/m2, SVi stress = 27 ml/m2, FR rest = 234 ml/s, FR stress = 203 ml/s). SV can drop physiologically during exercise due to reduction in ejection time [2]. However the drop in FR remained unexplained. This could be due to stress-induced myocardial dysfunction originating from global ischaemia due to AS or from myocardial ischaemia due to associated significant coronary artery disease (CAD). The patient had contrast ESE in order to assess for exercise induced LV dysfunction. This showed significant Regional Wall Thickening Abnormality in the left anterior descending (LAD) territory involving 9 out of 17 segments. She therefore underwent a coronary angiogram which confirmed features of tight proximal LAD disease (Fig. 1). Patient was referred for aortic valve replacement (AVR) and coronary artery bypass grafting.
Fig. 1
A Exercise stress echocardiography: LVOT PW Dopplers demonstrate drop in stroke volume (SV) at peak stress. B Exercise stress echocardiography (contrast): Apical 4- and 2-chamber at peak stress demonstrate inducible ischaemia in the LAD territory. C Coronary angiography: features of tight proximal LAD disease
× ![]()
…