




Published in:
01-06-2019 | Central Nervous System Trauma | Neuro-Images
Paroxysmal Sympathetic Hyperactivity with Dystonia Following Non-traumatic Bilateral Thalamic and Cerebellar Hemorrhage
Published in: Neurocritical Care | Issue 3/2019
Login to get accessExcerpt
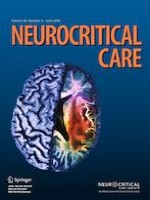
A 53-year-old male with diabetes, hypertension, and prior left putaminal and right gangliocapsular hemorrhages was admitted due to left facial droop. Initial examination revealed left hemiparesis/facial droop and stable vital signs (systolic blood pressure [SBP] 115 mmhg and heart rate 70 bpm). Computed tomography of the brain showed a new intraparenchymal hemorrhage in the right cerebellum and a left gangliocapsular area of encephalomalacia associated with a right thalamic hemorrhage (Fig. 1). On third day of admission, the patient was found to have episodes of intermittent hyperthermia (37.3–38.9 Celsius), tachycardia (59–127), diaphoresis, mydriasis, and hypertension (SBP 120–189) associated with dystonia of the neck, and bilateral upper and lower extremities (Video 1). Initial concern was for seizures; however, electroencephalography only revealed diffuse slowing consistent with encephalopathy. Potential mimicking conditions, such as infectious, inflammatory, and toxic-metabolic conditions were ruled out, and paroxysmal sympathetic hyperactivity (PSH) was diagnosed. Patient was treated with bromocriptine and propranolol with marked improvement. Although the role of dopamine in PSH remains unclear, dopamine agonists like bromocriptine may be helpful [1].
Fig. 1
CT brain demonstrating thalamic and cerebellar hemorrhages
× ![]()
…