




Published in:
01-06-2016 | Images
“Red Hand Syndrome” Due to Cytarabine in a Case of Mantle Cell Lymphoma
Published in: Indian Journal of Hematology and Blood Transfusion | Special Issue 1/2016
Login to get accessExcerpt
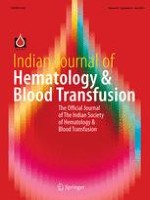
We report a 45-years-old gentleman, diagnosed with mantle cell lymphoma (MCL) Stage-IIIB at our hematology clinic and started on an alternating regimen of CHOP [Cyclophosphamide (750 mg/m2), doxorubicin (50 mg/m2), vincristine(1.4 mg/m2), prednisone(60 mg/m2 for 5 days)] and DHAP [Dexamethasone (40 mg oral D1-4), Cisplatin (100 mg/m2 intravenously on D1), cytarabine (2000 mg/m2 intravenous 12 hourly on D2)] every 21 days. Rituximab could not be administered due to non affordability. Patient tolerated the CHOP well and presented to us 24 h after the administration of cytarabine (Ara-C) in DHAP cycle with complaints of erythematous lesions on bilateral hands associated with intense itching and mild pain. Examination revealed well demarcated areas of erythema on bilateral palms and fingers (Fig. 1) with sparing of other body parts. Patient was diagnosed as Ara-C induced ‘limited’ acral erythema and was treated with oral pyridoxine (100 mg per day), hydroxyzine (25 mg thrice daily) and cold compression of palms. Rash gradually subsided with desquamation over 7 days. Interestingly, the rash reappeared 24 h after the next DHAP and not after the CHOP cycle. Patient was reassured of its benign nature and was advised prophylactic treatment with pyridoxine and cold application to palms during subsequent Ara-c infusions. Patient completed the remaining cycles of CHOP–DHAP without the need for treatment interruption and achieved complete remission of his disease. MCL accounts for 6 % of all non-Hodgkin’s lymphomas (NHL). Incorporating high dose Ara-C (HIDAC) and Rituximab in frontline settings, an overall response rate and complete remission of 95 and 36 % respectively has been achieved with RCHOP/RDHAP regimen (v/s 90 and 25 % respectively with RCHOP alone) [1]. Our patient was administered upfront CHOP/DHAP, based on our institutional protocol for newly diagnosed fit cases of MCL. The concept of cutaneous toxicity of anticancer drugs including Ara-C was first reported in 1982 by Burgdorf et al. [2]. Skin toxicity manifests as maculopapular rash, morbilliform rash or a unique eruption known as acral erythema, ‘hand-foot syndrome’ or ‘palmar-plantar erythrodysesthesia (PPE)’. PPE manifests as erythema of palms and soles, associated with pain, tingling, paresthesia and edema progressing to ulceration and desquamation in severe cases. Lesion is usually self-limited and is rarely life threatening. Accumulation of the drug and its metabolites in sweat glands has been proposed as a possible underlying mechanism [3]. Cytarabine induced skin toxicity is usually seen with HIDAC when given as infusion in the treatment of acute myelogenous leukemia (AML). Cetkovska et al. [4] in their study of 172 patients treated with HIDAC, found an overall incidence of cutaneous toxicity to be 53 % which was dose dependent. Incidence of Ara-C induced PPE has been reported between 14 and 33 % at doses >1000 mg/m2 [5]. Recently, Morio et al. [5] described risk factors for Ara-C related skin reactions (AML, no steroid use and age <50 years) and found that concomitant use of steroids with Ara-C reduced the incidence of PPE, thereby explaining a significantly lower incidence of skin reactions in patients with NHL. Our patient developed localized red palms without the full blown PPE while receiving Ara-C and concurrent steroids for NHL. Isolated “Red hand syndrome” is extremely rare in the treatment of NHL. Current case emphasizes the fact that treatment interruptions due to red palms while on Ara-C are unnecessary and requires re-assurance and conservative management.
Fig. 1
Bilaterally symmetrical areas of palmar erythema following cytarabine therapy
× ![]()
…