Introduction
After three successful annual meetings in Taormina (Italy), Thessaloniki (Greece) and Wiesbaden (Germany), the Euro CTO Club moved to England for its fourth meeting. Attendance included key speakers from Japan and the USA, 180 interventional cardiologists active in CTO recanalisation (including 35 Euro CTO Club members), and a large representation from industry. The format remained the same as the previous three meetings, focusing on 16 recorded CTO cases to offer examples of easy and difficult anterograde and retrograde approaches with various techniques. The recordings were edited to extract key learning points, condensed to 20-30 minutes from much longer procedures. All cases, discussion included, and all presentations were recorded and are already available online on the website of the Euro CTO Club: www.eurocto.eu (click on Events and WEB TV or via www.livemedia.gr/webtv/eurocto). The aim of this short editorial is not to summarise 15 hours of discussion or offer an alternative to the recently published Euro CTO consensus document1 but to identify a few leitmotifs of the course, with special attention to the many elements of innovation.
CTO SLANG AND MATERIAL
The main criticism at the previous course in Wiesbaden came from less experienced operators totally lost in following complex cases where mysterious expressions such as trapping, reverse controlled antegrade and retrograde subintimal tracking (CART) and subintimal transcatheter withdrawal (STRAW) alternated with the equally unfamiliar names of dedicated wires and microcatheters. We took advantage of this feedback and started the congress with Anthony Gershlick trying to convince the audience that CTO slang is no worse than cockney, the type of slang spoken in the part of London where the congress was held. Gerald Werner, Antonio Serra and Craig Thompson systematically reviewed primary and adjunctive material used, comparing properties and potential advantages of wires and microcatheters, highlighting the need for unusual bailout material, from the Venture microcatheter (St. Jude Medical, St. Paul, MN, USA) to coils and snares. Throughout the course and in parallel with the presentation of cases, on a secondary screen Matteo Ghione, Pilar Agudo and Albert Alahmar presented factoids focused on devices, schematic drawings of the techniques, and results of CTO studies.
ANTEROGRADE OR RETROGRADE?
At each course for the past three years the first question to the panel after the presentation of the case concerned the route to follow: which is better –anterograde or retrograde? If the presenter or the panellist chose retrograde immediately, this required explanation, almost an apology. The impression is that this year everything has changed. More sophisticated materials, e.g., Corsair catheter, Sion wire (both ASAHI Intecc., Aichi, Japan), together with increasing operator experience, have allowed a growth in retrograde operators and procedures. The usual update of the Euro CTO registry2, presented by Alfredo Galassi, showed a growth utilisation of the retrograde approach from the 59 members, from a stable 10% in 2008-2010 to 18% in 2011 and 25% in 2012. There was clear consensus that truly ostial occlusions, occlusions which are ambiguous or have no stump, lesions failed during well conducted anterograde attempts, lesions with a distal cap at a large bifurcation or vessels poorly visualised from collateral flow are indications for the retrograde approach in the presence of suitable interventional collaterals. The cases presented by Nick Palmer, Javier Escaned, Gerald Werner, Nicolaus Reifart, Roberto Garbo, Aigar Lismanis, Elliot Smith, Giorgios Sianos, Andrea Gagnor, James Spratt and Alfredo Galassi showed obvious individual differences in the threshold to move to a retrograde approach, fairly low in operators with good experience in tackling difficult collaterals, but higher in operators who routinely try to identify stumps with IVUS and accept the possibility of a distal re-entry using IVUS or Stingray (BridgePoint/Boston Scientific, Natick, MA, USA). A point fully clarified by the Euro CTO Club registry (Figure 1A and Figure 1B) and consistent with previous US data3 is the higher success rate of retrograde operators (90% vs. 80% obtained by operators not accustomed to this approach).
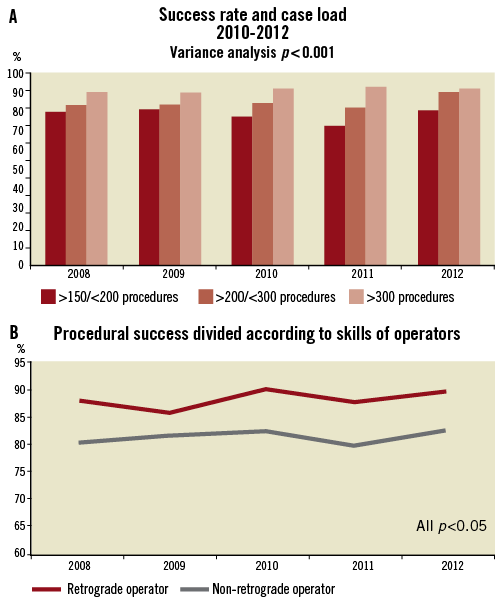
Figure 1. 2008-12 European Club database. The graphics show the procedural success over time according to the operator’s overall experience (A) and ability to apply a retrograde approach (B).
COLLATERAL SURFING OR SELECTIVE INJECTION?
There are differences in the way septal collaterals are approached, and this was clearly explained in one of the two “Controversies”. Surfing, i.e., probing collaterals with a rapid to and fro movement to identify the path of least resistance, was defended by Sudhir Rathore. He explained that this random selection often leads to engaging and crossing smaller, sometimes partially invisible but straighter collaterals. Masahisa Yamane preferred the routine preliminary creation of a road map, selectively injecting the most promising collateral. The consensus was an approach respectful of the anatomies of collaterals, with a trial and error strategy well suited to multiple small septal collaterals, and a preliminary injection from the Corsair at the ostium of the septal or of the epicardial collateral preferred for single larger and tortuous collaterals. The importance of a careful review of the diagnostic angiogram (acquired without panning and in the best views to define the course of the collateral and its connections with donor and recipient arteries) was stressed by Masahiko Ochiai. A practical tip to ensure the acquisition of readable angiograms is the utilisation of a high-pressure syringe. Gerald Werner warned against the potential risk of collateral damage and contrast extravasation during forceful selective injections when no blood can be aspirated from a fully wedged microcatheter.
6 Fr OR LARGER LUMEN GUIDING CATHETERS?
CTO operators are often perceived as old school femoralists unable to switch to the modern radial approach, shown to reduce bleeding and possibly mortality, especially in STEMI patients4. Masahisa Asakura et al defended the freedom allowed by large guiding catheters, indispensable when the Corsair is the preferred microcatheter and is used in combination with balloon trapping or anchoring or concomitant IVUS. Conversely, Georgios Sianos reported good compatibility of small microcatheters such as the FineCross (Terumo Corp., Tokyo, Japan) with a monorail balloon but also a second FineCross. Keen radialists such as Aigars Lismanis assured the audience that 7 Fr and 8 Fr catheters are compatible with the radial arteries of most male patients. Others praised sheathless catheters5 or the use of the radial for contralateral injection of the donor artery or for anterograde use, gaining with deep intubation the back-up lost with the inability to anchor the guiding catheter.
STINGRAY: LIMITED BAIL-OUT USE OR THE STANDARD TOOL OF CHOICE FOR PREDICTABLE RE-ENTRY?
Craig Thompson and James Spratt clearly explained the reasons for their preference for this device as a routine strategy for lesions longer than 20 mm with well-defined stumps6. They also supported its use in synergy with the CrossBoss (BridgePoint/Boston Scientific, Natick, MA, USA), able to create a small lumen sufficient for the advancement of the Stingray, avoiding large dissections which may obliterate the distal lumen7. Many European and Japanese operators, however, possibly prompted in part by cost and lack of availability, expressed scepticism about the ability of the Stingray to gain large acceptance outside niche indications when “conventional” techniques already obtain >80% success. Osamu Katoh reviewed the use of IVUS to obtain distal re-entry or guide reverse CART. However, while praising the extraordinary skills of the presenter, many questioned the applicability of this technique as a potential alternative to the Stingray because of the long and steep learning curve needed to obtain enough experience with image interpretation to apply this method successfully.
PREVENTION OF COMPLICATIONS
Alexander Bufe, Elliot Smith, Joachim Buettner, Leszek Bryniarski, Carlo Di Mario were some of the operators brave enough to share their difficulties and mistakes and explain the way they managed to rescue the situation most of the time. The compulsive use of ACT measurements to prevent catheter thrombosis, especially in the retrograde approach, protection of the left circumflex for truly ostial LAD occlusions approached retrogradely, proximal aspiration from an over-the-wire balloon to restore retrograde filling after large anterograde dissections, extreme caution in handling the catheter in the donor vessel, continuous attention to contrast and radiation dose and rapid access to coils and covered stents were some of the lessons learned by the attendees. Hopefully these presentations will help in diminishing the incidence of such events in the future. The very low incidence of periprocedural death (0.3%) and cardiac tamponade requiring pericardiocentesis (0.6%) reported in more than 4,000 procedures from Euro CTO Club members (Figure 2) suggest CTO recanalisation can remain safe when performed by expert operators.
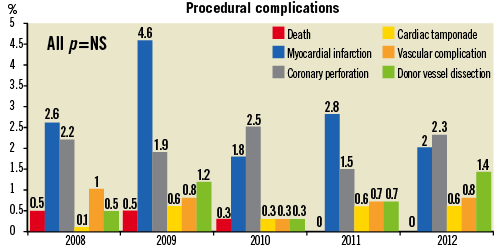
Figure 2. 2008-12 European Club database. Procedural complication rates between 2008 and 2012.
Conclusions
Reading these two pages has probably helped you to get a flavour of the topics presented in the recent Euro CTO congress, but watching the live presentations and lectures with all the slides and images available will give you more. However, you will miss a key benefit of this congress; it is the largest in the world focused on the specific topic of CTO recanalisation, but it is still sufficiently small to allow interaction among participants. During the get-togethers between congress days, participants shared their experience, their criticisms of the cases presented and their recipes to create and maintain an active CTO programme in their hospitals. The organisers promised interaction and live participation: this was achieved. The feedback received was very positive and the few constructive criticisms will help the Club to make an even better edition next time, The Experts “Live” CTO Workshop, Paris, September 27-28, 2013.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Appendix. Sentinel Registry of Transcatheter Valve Treatment: participating centres
TCVT Executive Committee: Carlo Di Mario, UK (Chairman), European Association of Percutaneous Cardiovascular Interventions (EAPCI); Aortic Valve Registry: Neil Moat, UK, Bernard Iung, France, ESC WG on Valve Disease; Gerhard Schuler, Germany, EAPCI; Pepe Zamorano, Spain, European Association of Echocardiography (EAE). Mitral Valve Registry: Ottavio Alfieri, Italy, ESC WG of Cardiovascular Surgery; Olaf Franzen, Denmark, EAPCI; Susanna Price, UK, ESC WG Acute Cardiac Care, L. Tavazzi (Oversight Committee), A. Maggioni (Board consultant for the EURObservational Research Programme)
National Coordinators:
BELGIUM E. Schroeder, M. Claeys; CZECH REPUBLIC P. Kala; FRANCE H. Eltchaninoff; GERMANY G. Nickenig; ISRAEL H. Danenberg; ITALY F. Romeo, GP. Ussia; POLAND M. Zembala; SPAIN J. Goicolea; SWITZERLAND R. Corti, P. Wenaweser; UNITED KINGDOM B. Prendergast.
EURObservational Research Programme team:
M. Manini (Head of Dept); G. Gracia, V. Missiamenou, M. Konte (data monitors); C. Laroche (statistician), C. Taylor (IT specialist), E. Fiorucci, E. Folkesson, M. Glemot, PA. McNeill (assistants)
FUNDING
The following companies are supporting the EURObservational Research programme: GOLD: Abott Vascular, Bayer Pharma, Bristol Myers Squibb (BMS), Pfizer, Boehringer Ingelheim, Daiichi Sankyo Europe, Menarini international Operations, Novartis Pharma, Sanofi-Aventis, Servier International. SILVER: Amgen. BRONZE: Boston Scientific International, Merck & Co. (MSD). The contribution of NICOR to the collection and transfer of the 2011 UK TAVI Registry is gratefully acknowledged.
Participating Centres with local PIs:
BELGIUM Aalst: M. Vanderheyden, Edegem: M. Claeys, Liège: V. Legrand, J. Beckers, J. Boland, Q. Desiron, D. Henroteaux, S. Pourbaix, O. Vanderperren, Yvoir: M. Buche, P. Chenu, A. Guédès, E. Schroeder.
CZECH REPUBLIC Brno: P. Kala, P. Nemec, M. Tretina, Ceske Budejovice: L. Pesl, Hradec Kralove: J. Stasek, J. Bis, Usti n. Labem: P. Cervinka, Olomouc: R. Stipal, Trinec: M. Branny, Praha: V. Kocka, P. Widimsky, M. Zelizko, M. Mates, J. Horak.
FRANCE Angers: J. Debrux, S. Delepine, A. Furber, F. Pinaud, Besançon: S. Chocron, N. Meneveau, F. Schiele, Bois-Bernard: O. Fabre, A. Gommeaux, P. Hochart, M. Pecheux, Brest: E. Bezon, J. Boschat, JN. Choplain, M. Gilard, Bron: R. Dauphin, G. Durand De Gevigney, G. Finet, O. Jegaden, JF. Obadia, G. Rioufol, Caen: G. Grollier, T. Lognone, M. Massetti, R. Sabatier, Caluire-et-Cuire: JP. Claudel, F. Gabrielle, F. Pelissier, G. Tremeau, Clermont-Ferrand: K. Azarnouch, N. Durel, A. Inorta, JR. Lusson, G. Souteyrand, Créteil: JL. Dubois Rande, M. Kirsch, E. Teiger, Grenoble: B. Bertrand, O. Chavanon, P. Porcu, G. Vanzetto, Le Chesnay: O. Bical, P. Deleuze, X. Favereau, A. Jegou, Le Plessis Robinson: A. Azmoun, C. Caussin, S. Ghostine, R. Nottin, Lille: F. Juthier, T. Modine, A. Sudre, E. Van Belle, Marseille: JL. Bonnet, F. Collart, T. Cuisset, D. Grisoli, F. Collet, A. Vaillant, J. Vicat, O. Wittenberg, R. Houel, P. Joly, R. Rosario, Massy: B. Chevalier, A. Farge, P. Garot, T. Hovasse, T. Lefevre, MC. Morice, M. Romano, Monaco: F. Bourlon, Montpellier/Nimes/Perpignan: B. Albat, M. Krastevich, F. Leclercq, C. Piot, L. Schmutz, Neuilly-sur-Seine: JC. Dib, B. Gerardin, T. Waldmann, Paris: D. Blanchard, JN. Fabiani, A. Lafont, R. Zegdi, F. Beygui, J. Collet, P. Leprince, A. Pavie, D. Himbert, P. Nataf, Pessac: E. Choukroun, P. Dos Santos, JP. Guibaud, L. Leroux, Rennes: M. Bedossa, D. Boulmier, H. Le Breton, JP. Verhoye, Rouen: JP. Bessou, A. Cribier, H. Eltchaninoff, C. Tron, Saint-Denis: N. Bonnet, F. Digne, P. Guyon, P. Mesnidrey, Saint-Herblain: D. Crochet, R. Gaudin, JC. Roussel, A. Tirouvanziam, Strabourg: M. Kindo, JP. Mazzucotelli, P. Ohlmann, Toulouse: D. Carrie, G. Fournial, B. Marcheix, D. Tchetche, Tours: O. Bar, C. Barbey, D. Blanchard, S. Chassaing, D. Chatel, O. Le Page, A. Tauran, Vandoeuvre les Nancy: M. Angioi, JP. Carteaux, F. Moulin, JP. Villemot, Villeurbanne: D. Champagnac, V. Doisy, Y. Lienhart, R. Roriz.
GERMANY Bad Krozingen: M. Bockstatt, HJ. Buettner, T. Comberg, R. Hoewisch-Pengel, E. Maurer, B. Steiger, Bonn: K. Brunsmann, C. Hammerstingl, P. Lang, M. Lennarz, G. Nickenig, R. Schueler, JM. Sinning, C. Zimmermann, Frankfurt: M. Bürgstein, S. De Bruijn, R. Eckhardt, S. Esfajani, M. Kroth, H. Sievert, M. Sirotina, N. Staiger, R. Talea, Hamburg: S. Baldus, K. Heitmann, B. Kolodzick, Lubeck: P. Radke, H. Schunkert, Münster: H. Baumgartner, A. Hellige, G. Kaleschke, G. Kerckhoff, München: M. Block, D. Brill, A. Erbsloeh, M. Fueller, Neuss: H. Degen, M. Haude, A. Kezic, L. Schürmann, Wuppertal: G. Haltern, M. Seyfarth, J. Szymanski, K. Tiroch.
ISRAEL Jerusalem: H. Danenberg, S. Loncar, G. Perlman.
ITALY Ospedale Ferrarotto Catania, C. Tamburino; Villa Maria Cecilia, Cotignola-Ravenna, A. Cremonesi; C. Grattoni, Lecce Hospital, Lecce, A. Liso; F. Castriota, Ospedale Arnas Civico, Palermo, A. Stabile; Ospedale Cisanello, Azienda Ospedaliera Universitaria, Pisa, A. Petronio; Policlinico Tor Vergata, Roma, F. Romeo; Istituto Humanitas, Milano, P. Presbitero; Policlinico Umberto I, Roma, G. Sardella.
POLAND Bialystok: S. Dobrzycki, M. Frank, T. Hirnle, P. Kralisz, A. Lukaszewicz, B. Sobkowicz, Bydgoszcz: L. Anisimowicz, J. Kubica, G. Lau, W. Ogorzeja, W. Pawliszak, M. Radomski, A. Sukiennik, I. Swiatkiewicz, M. Woznicki, Gdansk: D. Ciecwierz, D. Jagielak, R. Lango, G. Laskawski, J. Rogowski, R. Targonski, A. Wojtowicz, Katowice: M. Lelek, A. Ochala, R. Parma, G. Smolka, P. Weglarz, W. Wojakowski, Krakow: D. Dudek, B. Kapelak, P. Kleczynski, J. Konstanty-Kalandyk, J. Sadowski, R. Sobczynski, D. Sorysz, J. Trebacz, K. Zmudka, Poznan: M. Grygier, M. Jemielity, M. Lesiak, Warszawa: EK. Biernacka, Z. Chmielak, M. Dabrowski, M. Demkow, Z. Juraszynski, K. Kusmierski, J. Pregowski, W. Ruzyllo, A. Witkowski, Warszawa: R. Chichon, Z. Huczek, J. Kochman, M. Marchel, M. Michalak, G. Opolski, P. Scislo, R. Wilimski, K. Byczkowska, RJ. Gil, T. Kulawik, A. Pawlak, K. Suwalski, Wroclaw: W. Banasiak, P. Kubler, K. Reczuch, Zabrze: P. Chodor, Z. Kalarus, M. Krason, A. Lekston, T. Podolecki, R. Przybylski, W. Streb, P. Trzeciak, K. Wilczek, M. Zembala, J. Zembala-John.
SPAIN La Coruña: JJ. Cuenca Castillo, J. Salgado Fernandez, N. Vazquez Gonzalez, Alicante: P. Llamas, V. Mainar, Asturias: R. Del Valle, C. Moris De La Tassa, Badajoz: F. Gonzalez De Diego, J. Gonzalez Rodriguez, JR. Lopez Minguez, A. Merchan, Barcelona: A. Cequier Fillat, R. Romaguera, M. Castella, J. Mulet, M. Sabate Tenas, M. Jimenez, JM. Padro, A. Serra, F. Mauri, C. Oliete, X. Ruyra, B. Garcia, A. Igual, V. Serra Garcia, Bilbao: J. Alcibar, JI. Aramendi, JM. Aguirre Salcedo, L. Andraka, AA. Morist, J. Zuazo Meabe, Granada: E. Molina Lerma, Guipuzcoa: I. Gallo, J. Goiti, M. Larman, A. Saenz, Huelva: J. Diaz Fernandez, A. Gomez Menchero, Leon: M. Alvarez García, M. Castano, F. Fernandez Vazquez, J. Gualis Cardona, Madrid: F. Navarro Del Amo, A. Albarran Gonzalez-Trevilla, JM. Cortina, J. Tascon, J. Cobiella, E. Garcia, R. Hernandez Antolin, E. Rodriguez Hernandez, L. Martinez Elbal, F. Fernandez-Aviles Diaz, A. Gonzalez Pinto, J. Rodriguez Roda, JL. Zunzunegui, O. Al-Razzo, JM. Mesa, R. Moreno, P. Salinas, J. Goicolea Ruigomez, JF. Oteo Dominguez, J. Ugarte, A. Epeldegui, I. Garcia Andrade, J. Pey Yllera, Malaga: OG. Albarova, JH. Alonso Briales, JM. Hernandez Garcia, AJ. Munoz Garcia, C. Urbano Carrillo, Murcia: R. Arcas, E. Pinar, M. Valdes, Salamanca: I. Cruz, J. Martin Moreiras, Santander: JM. Revuelta, J. Zueco, Santiago de Compostela: AL. Fernandez Gonzalez, D. Lopez, R. Trillo Nouche, Sevilla: JM. Barquero Aroca, RR. Salmeron, JM. Borrego, JM. Cubero Gomez, A. Sanchez, Toledo: A. Canas, J. Moreu Burgos, Valencia: O. Albarova, A. Berenguer, S. Canovas Lopez, Valencia: J. Anastasio Romero, Vigo: A. Iniguez, V. Jimenez, J. Montoto Lope, G. Pradas.
SWITZERLAND Bern: P. Wenaweser, C. Huber; Basel: R. Jeger, F. Rütter; Geneve: M. Roffi, S. Noble; Lugano: G. Pedrazzini, F. Siclari; Lausanne: D. Locca, E. Ferrari Triemlispital, Zurich: David Tueller, Michele Genoni; Zurich: L. Altwegg, J. Grünenfelder.
UNITED KINGDOM Belfast: G. Manoharan, R. Jeugnathan; Birmingham: S. Doshi, P. Ludman, J. Mascaro; Brighton: D. Hildick-Smith, U. Trevedi; Bristol: A. Baumbach, M. Turner; Blackpool: DH. Roberts, A. Tang; Cambridge: C Densem, S. Tsui; Cardiff: Derriford; Leeds: D. Blackman, M. McLenegham, P. Kaul; Leicester: J. Kovac, T. Spyt; Liverpool: R. Stables, M. Kuduvalli; London: C. Knight; C. Di Mario, N. Moat, S. Price, T. Snow; M. Dalby, M. Amrani; I. Mallik, G. Michail, A. Chuckwemeka; P. McCarthy, O. Wendler; S. Brecker, M. Jahangiri; S. Redwood, M. Thomas, C. Young; M. Mullen, J. Yap; Manchester: F. Ordoubadi; Middlesborough: M. de Belder, A. Goodwin; Morriston: A. Chase, A. Youhana; Newcastle; Nottingham: R. Henderson, I. Mitchell; Oxford: B. Prendergast, R. Sayeed; Plymouth: I. Cox, C. Lloyd; Southampton: A. Calver, N. Curzen, G. Tsang; Stoke-on-Trent: M. Gunning, A. Levive; Wolverhampton: S. Khogali, B. Moninder.
