


Abstract
Background: Canada needs to increase capacity for bariatric surgery to reduce the wait for this cost-effective, life-saving surgery. The aim of this study was to test whether laparoscopic bariatric surgery, including gastric bypass, can be delivered safely in secondary health care centres (SHCCs).
Methods: In this prospective cohort study, patients received bariatric surgery at an SHCC that had no intensive care unit but had a dedicated operating room and ward teams and a patient-monitoring environment. Patients with life-threatening complications were transferred to an affiliated tertiary health care centre (THCC) via a dedicated “service corridor.”
Results: In all, 830 patients were treated: 676 at the SHCC and 154 at the THCC. Gastric bypass was performed in 85.4%, gastric band in 11.1% and gastric sleeve in 3.5%. The body mass index (BMI) was significantly higher in the THCC than the SHCC group (mean 54.4 [standard deviation (SD) 9.7] v. 47.5 [SD 7.4]). Obesity-associated diseases were similar between the groups. Major complications occurred in 2.6% of SHCC patients and 1.7% of THCC patients. Seven patients (1%) required direct transfer to the THCC, and all were treated successfully. There were 2 deaths (1.3%) in the THCC and none in the SHCC groups (combined mortality 0.2%). Weight loss was equivalent up to the fourth year of the study.
Conclusion: With proper patient selection, a dedicated health care team and a service corridor to an affiliated THCC, laparoscopic bariatric surgery, including gastric bypass can be performed safely in SHCCs. Further study is needed to determine whether the model can be applied across Canada.
According to the World Health Organization, obesity is reaching epidemic proportions. Canada is no exception to this epidemic: most Canadians are overweight or obese,1 and 2% of men and 4% of women are morbidly obese.2 Obesity-related death rates are at least on par with deaths related to smoking, and some authors believe that obesity is now the number 1 killer in North America.3
Bariatric surgery is the only treatment that produces substantial, sustained, long-term weight loss in patients with severe obesity.4,5 In addition, permanent weight loss through bariatric surgery reduces the relative risk of death by 35%–89%6–10 and produces substantial pharmacoeconomic benefits.11 Despite these well-documented findings, bariatric surgery is difficult to access in Canada.12,13
In 2006, a unique pilot project was initiated to determine whether laparoscopic bariatric surgery can be safely performed in smaller hospitals, designated as secondary health care centres (SHCCs), and linked via a dedicated service corridor to a full service tertiary health care centre (THCC). The model was proposed by l’Agence d’évaluation des technologies et des modes d’intervention en santé (AETMIS) in their report to the Quebec Minister of Health and Social Services as a means of increasing bariatric surgery capacity in the province.14 The present article outlines the findings of this pilot project.
Methods
This pilot project was initiated following publication of the AETMIS report and a meeting with the Quebec Minister of Health and Social Services at the time. The 534-bed McGill University Health Centre (MUHC), which has more than 40 years of bariatric surgery experience, is fully equipped with an intensive care unit (ICU) and has dialysis capability, was selected as the THCC. The SHCC was the Centre Métropolitain du chirurgie, a fully accredited 17-bed private hospital with a “Specialized Medical Centre” designation from the Ministry of Health and Social Services.15 The SHCC has no ICU, but has a patient-to-nurse ratio of 1:3 and oxygen saturation monitoring capacity for all patients, essentially providing “step-down unit” care for the patients until discharge. The same surgeon performed all procedures with the same dedicated operating room team, ward nurses and support staff over the duration of the study. Patients with potentially life-threatening complications were transferred to the THCC via a special ambulance using a priori determined protocol (dedicated “service corridor”).
All patients met the 1991 National Institutes of Health Consensus Conference guidelines16 for bariatric surgery: a body mass index (BMI) greater than 35 with associated comorbidities, or a BMI greater than 40. All patients were assessed, including medical, nutritional and psychological assessments, by a multidisciplinary team. Uncontrollable binge-eating disorders required treatment before surgery. All patients were also required to demonstrate an understanding of the surgical procedure they were scheduled to undergo, its mechanism of weight loss, potential long- and short-term complications, dietary and physical activity requirements, and the need for lifelong supplements and follow-up. The procedure choice was left up to the patient after a detailed formal presentation of the anatomy, mechanisms of action, short- and long-term complication rates and expected weight loss associated with each procedure.
Patients with American Society of Anaesthesiology (ASA) class 4 disease or an obesity surgery mortality risk score (OS-MRS17) greater than 4 were excluded from having surgery at the SHCC. Patients weighing more than 205 kg were also excluded owing to ambulance transfer restrictions. The surgeon was the only constant at the THCC, with patients treated on the ward or in the ICU as deemed appropriate. All patients were placed on a high-protein, low-carbohydrate diet for 2 weeks before surgery. Thromboprophylaxis included sequential compression stockings during the surgery, the administration of 5000 units of unfractionated heparin subcutaneously every 12 hours until discharge, and very aggressive and early mobilization, especially at the SHCC, where the patient-to-staff ratio made this feasible. No perioperative antibiotics were given. We followed “awake intubation” protocol for all patients at the SHCC using fibreoptic intubation under heavy sedation to secure the airway before administration of paralytic agents.
Our laparoscopic gastric bypass technique involves a 30–50 cm biliopancreatic limb and a 100 cm retrocolic, antegastric, alimentary limb. The jejunojejunal anastomosis is constructed side-to-side with a single firing of a linear endostapler, and the stapler entry point defect is hand sewn. The gastric pouch is small (2 × 7 cm) and vertically oriented, and the gastrojejunal anastomosis is hand sewn. Pneumatic and methylene blue tests are used to ensure the integrity of staple and suture lines at the time of surgery. The Petersen space and the transverse mesocolic defect are routinely closed with running polypropylene sutures. Vertical sleeve gastrectomy is performed “loosely” over a 36 F bougie using the appropriate endostapler with no reinforcements. Integrity of the staple line is verified, as for the gastric bypass. All gastric bands are inserted using the pars flaccida technique.
The outcome data (demographic characteristics, weight loss, complications) were recorded prospectively in our bariatric surgery registry. We calculated the kilogram weight loss, percent body weight loss (weight loss ÷ baseline body weight × 100) and percent excess weight loss (%EWL; 100% × ([W0–Wi] ÷ EW0), where W0 is the weight in kilograms at the time of surgery, Wi is the weight in kilograms at the last follow-up, and EW0 is the excess weight at the time of surgery). Excess weight was estimated according to the formula described by Deitel and Greenstein18 and is based on the Metropolitan Tables for middle frame individuals. Complications occurring within 30 days of the date of surgery were defined as short-term complications, and complications occurring after 30 days were defined as long-term. We also determined 30-day mortality and the number of deaths during the long-term follow-up that could be related to the original bariatric surgery.
Statistical analysis
We used IBM SPSS Statistics 20 for the computations and statistical analysis. Continuous variables were tested for significance using unpaired t tests; the χ2 was used to compare proportions. Logistic regression analysis was used to compare individual variable contribution to mortality.
Results
In all, 830 patients were enrolled in the study: 676 (81.4%) were treated at the SHCC and 154 (18.6%) were treated at the THCC. Table 1 shows the patient demographic and clinical characteristics and the type of surgery performed at each centre. There were significantly more women treated at the SHCC than the THCC, and patients treated at the SHCC were slightly younger by about 1 year than those treated at the THCC. The patients at the THCC were heavier and their BMI significantly higher than those treated at the SHCC. Laparoscopic gastric bypass was the most common procedure (85.4%), followed by gastric banding and gastric sleeve. There was a significant discrepancy in the distribution of the surgeries performed at each centre; gastric bypass was the predominant procedure because gastric banding was not publicly funded in Quebec until recently.
Demographic and clinical characteristics of the study population
The distribution of obesity-associated comorbidities is shown in Table 2. Most comorbidities were equally distributed; however, heart disease was more common among patients treated at the THCC, as was expected based on patient selection criteria, and weight-bearing osteoarthropathy was also more common among those treated at the THCC, as was expected based on the higher BMI in that group. Table 3 shows the types of complications recorded within the first 30 days after the surgery. As expected, complication rates were slightly higher in the THCC group given the patient selection criteria. Obesity surgery mortality risk scores and ASA score were also significantly higher in the THCC group (Table 4).
Obesity-associated diseases and conditions in the 2 cohorts
The types of complications recorded within the first 30 days after surgery at each site
Patient stratification and complications recorded within the first 30 days after surgery at each site
The major complication rate was 2.3% at the SHCC and 5.8% at the THCC (p = 0.036). Similarly, minor complications were significantly more frequent in the THCC group (p = 003). The readmission rates in the 30 days after surgery were equivalent between the groups. There were 7 direct transfers (1.2%) from the SHCC to the THCC via the dedicated “service corridor.” The reasons for the transfer as well as the treatment and outcomes are shown in Table 5. All 7 patients made a full recovery. An additional 9 patients returned to the hospital on average 11 (standard deviation [SD] 9, range 3–33) days after surgery for the reasons outlined in Table 6. All of them were successfully treated and made a full recovery.
Reason for direct transfer from the SHCC to the THCC
Reason for readmission to the THCC after discharge from the SHCC
There were 2 deaths at the THCC. The first was a woman with a BMI of 75.5, ASA of 3 and OS-MRS of 3 who underwent an uneventful laparoscopic gastric bypass but suffered a massive pulmonary embolism on day 4 post-surgery, the day of her planned discharge. The second was a woman with a BMI of 59, ASA of 4 and OS-MRS of 4, who was on home oxygen and who underwent an uneventful laparoscopic gastric bypass. She was admitted to the ICU as planned for progressive weaning from the ventilator, but nosocomial pneumonia developed and she died in the ICU. No deaths occurred in the SHCC. Overall mortality was 0.2%. Logistic regression analysis failed to identify any variables (age, sex, location of surgery, starting BMI, ASA score, OS-MRS) contributing to the risk of death owing to low incidence of death.
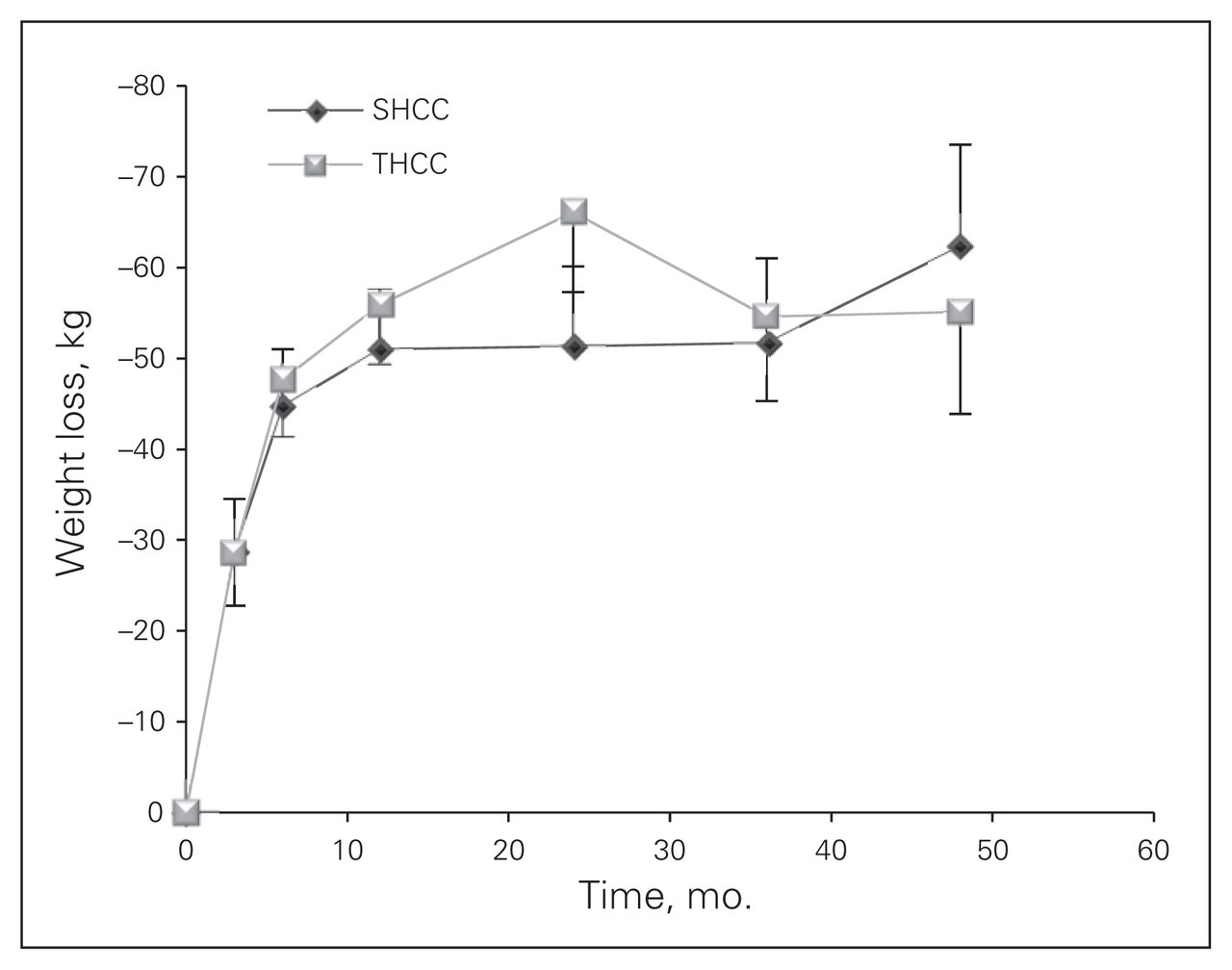
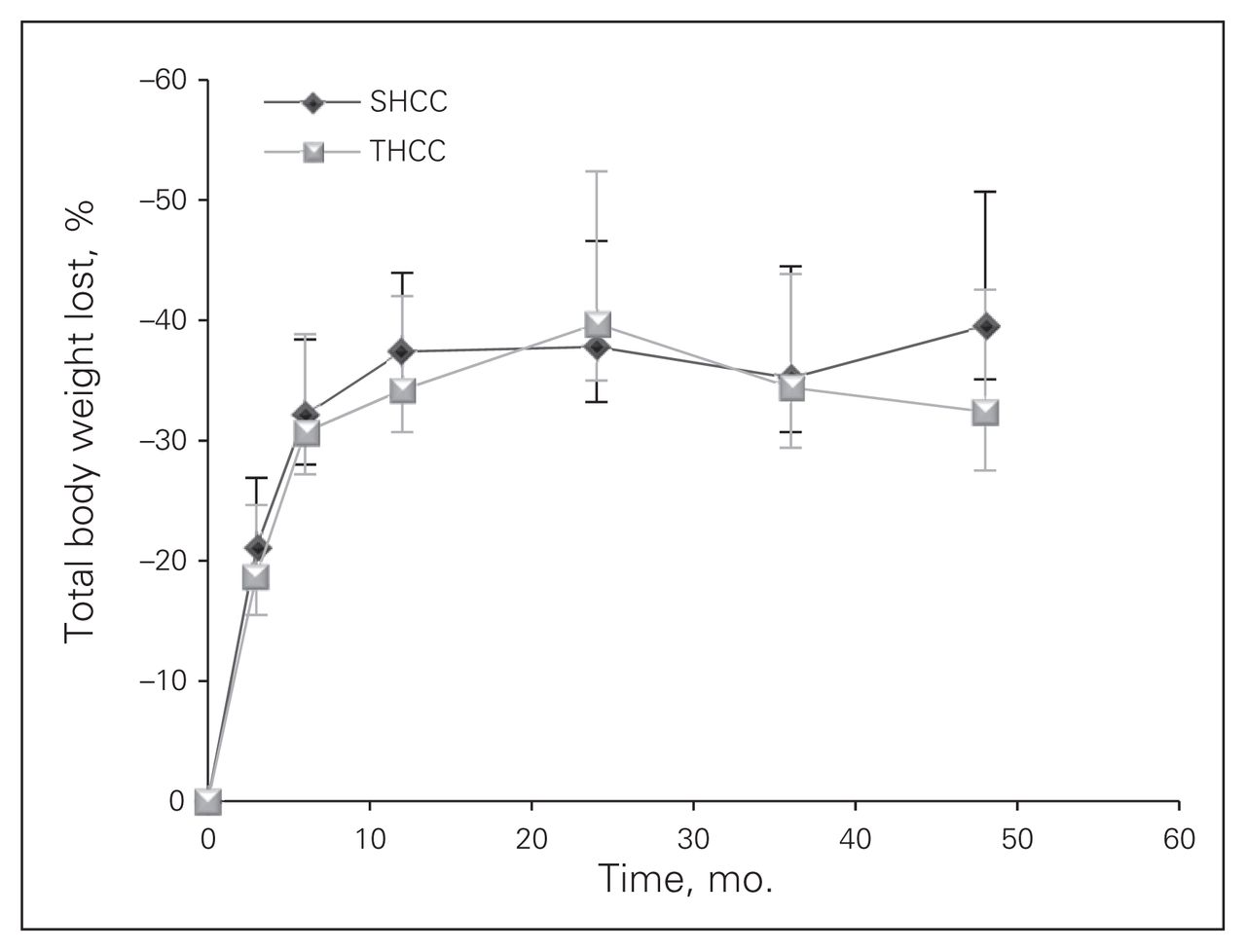
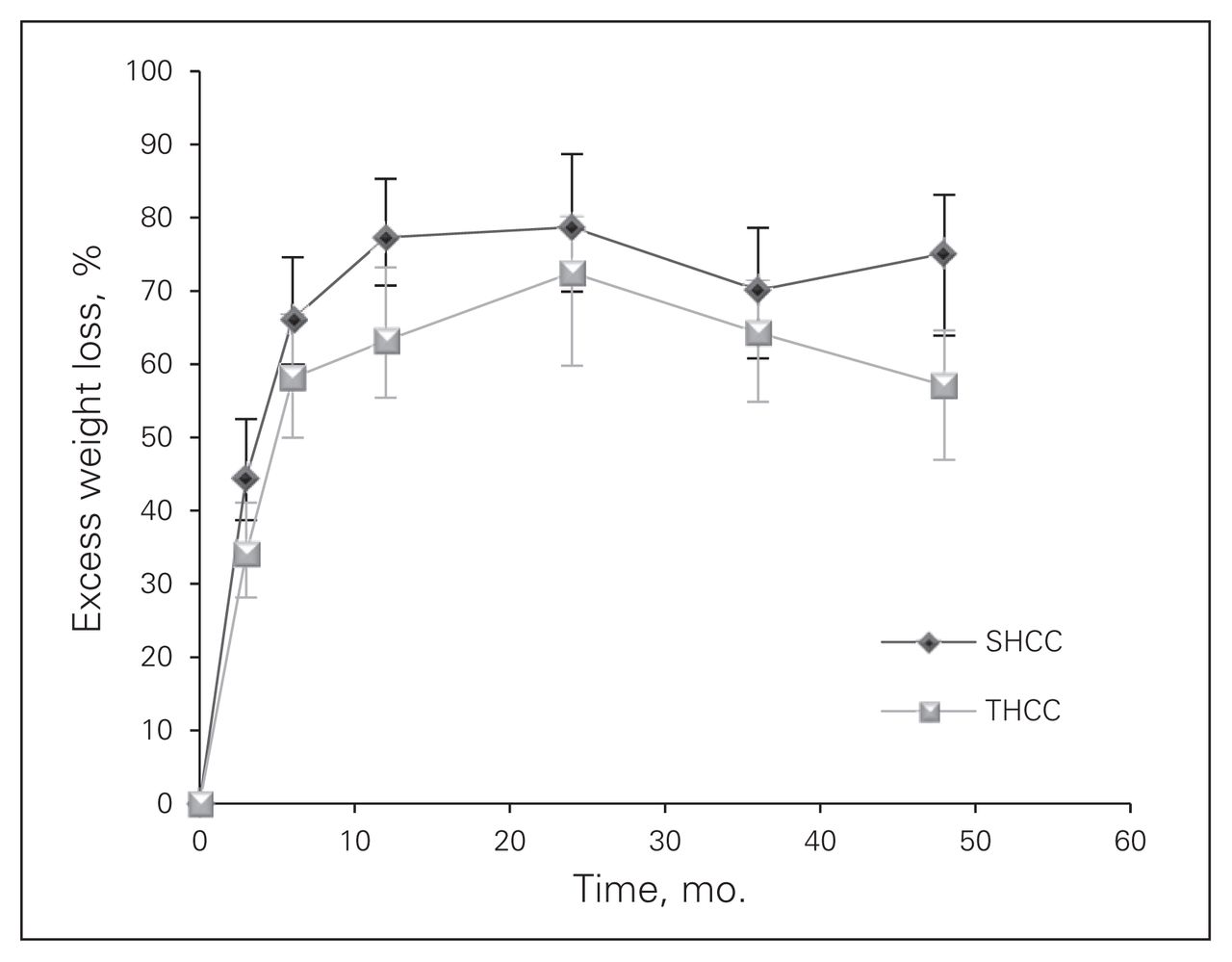
Weight loss in kilograms (Fig. 1) and the percentage of total weight loss (Fig. 2) were equivalent between the 2 centres. This method of weight loss data presentation is not affected by the starting patient weight or BMI. The %EWL (Fig. 3) appears to be better at the SHCC than the THCC. Since the %EWL is affected by the starting BMI (i.e., better %EWL in patients with lower BMI), we adjusted the %EWL calculation for starting BMI and found no difference between the 2 groups.
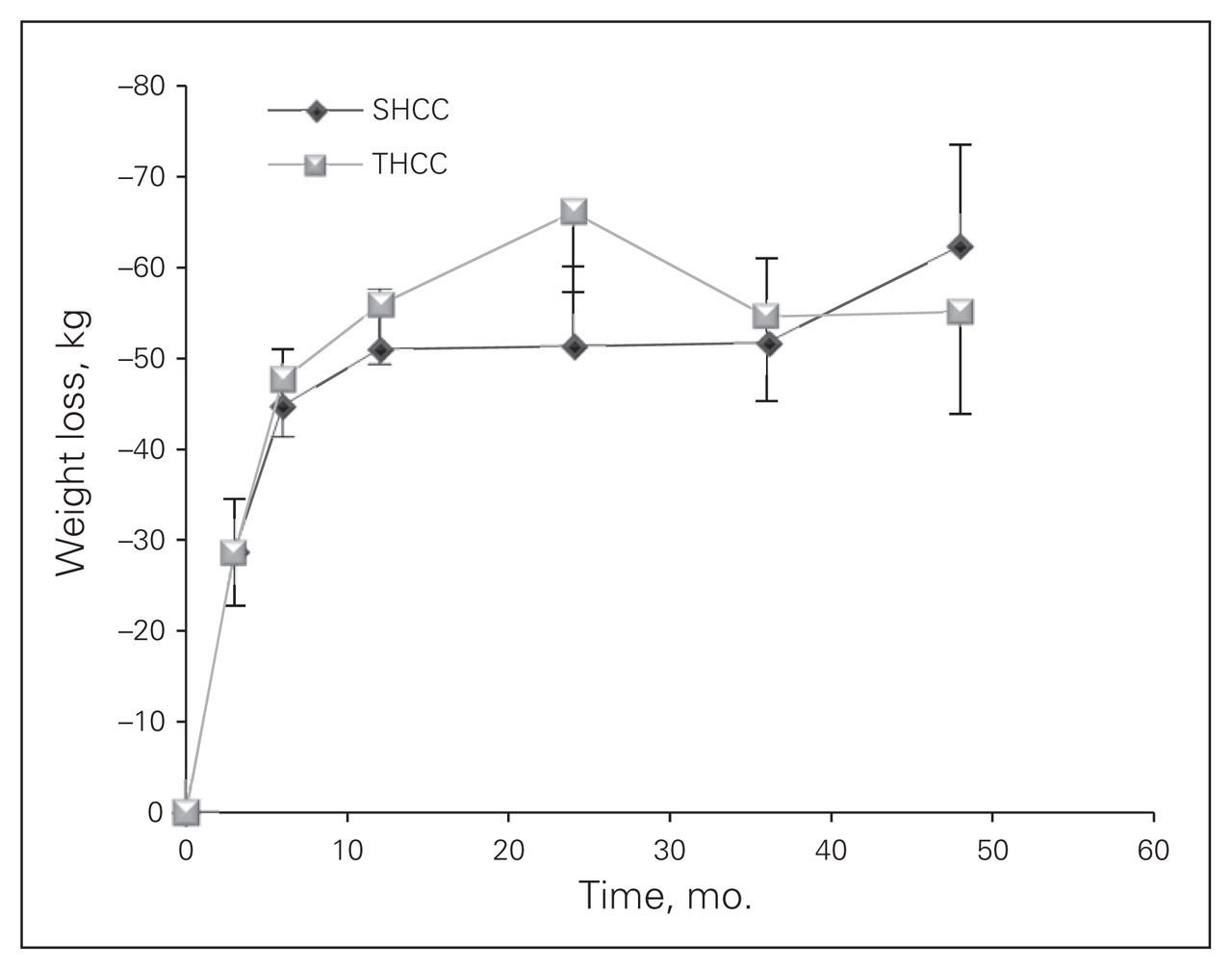
Weight loss in kilograms in patients with laparoscopic gastric bypass at each site. Mean and standard deviation are shown as well as the number of cases followed-up at each time point. SHCC = secondary health care centre;THCC = tertiary health care centre.
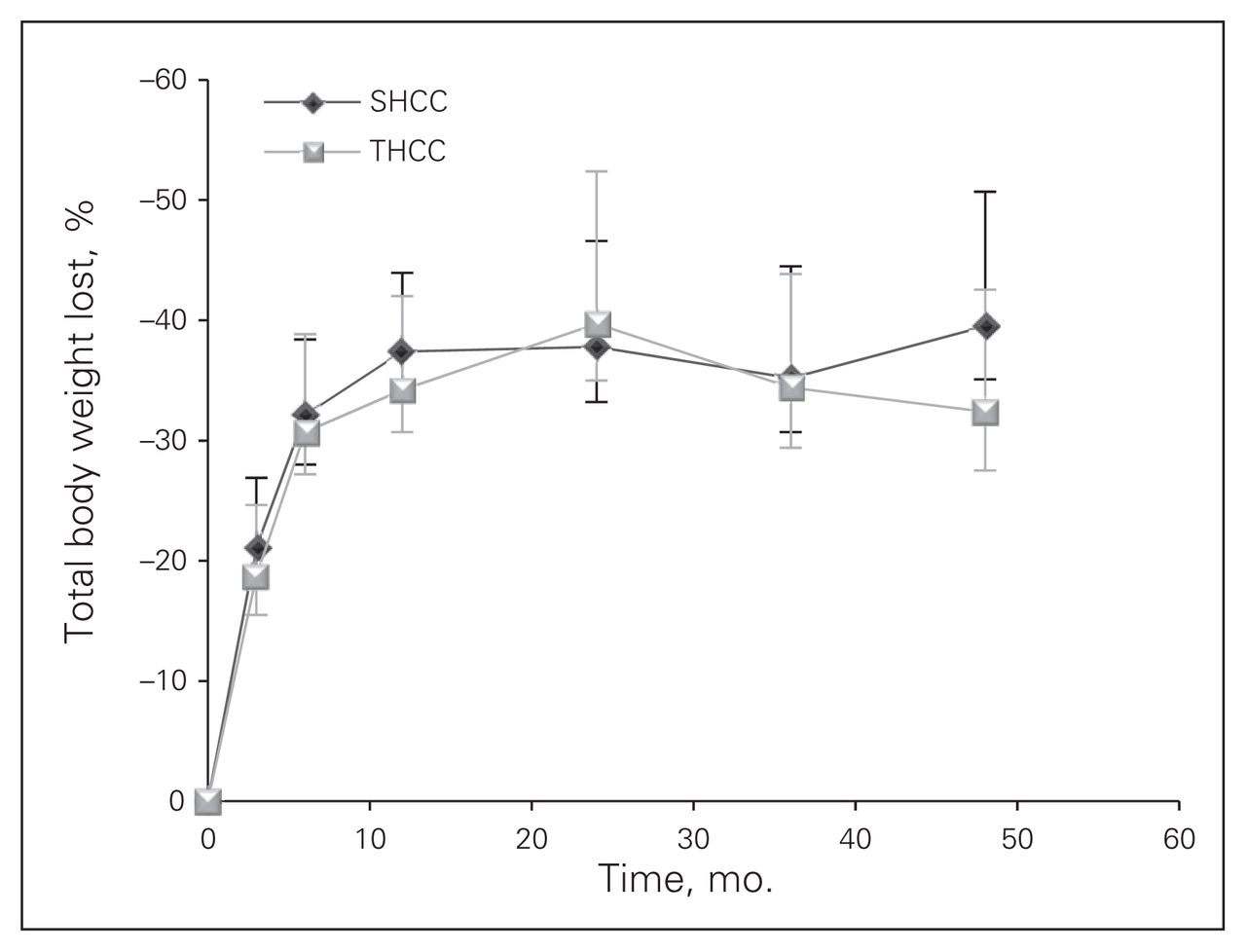
Percent total body weight loss in patients with laparoscopic gastric bypass at each site. Mean and standard deviation are shown as well as the number of cases followed-up at each time point. SHCC = secondary health care centre;THCC = tertiary health care centre.
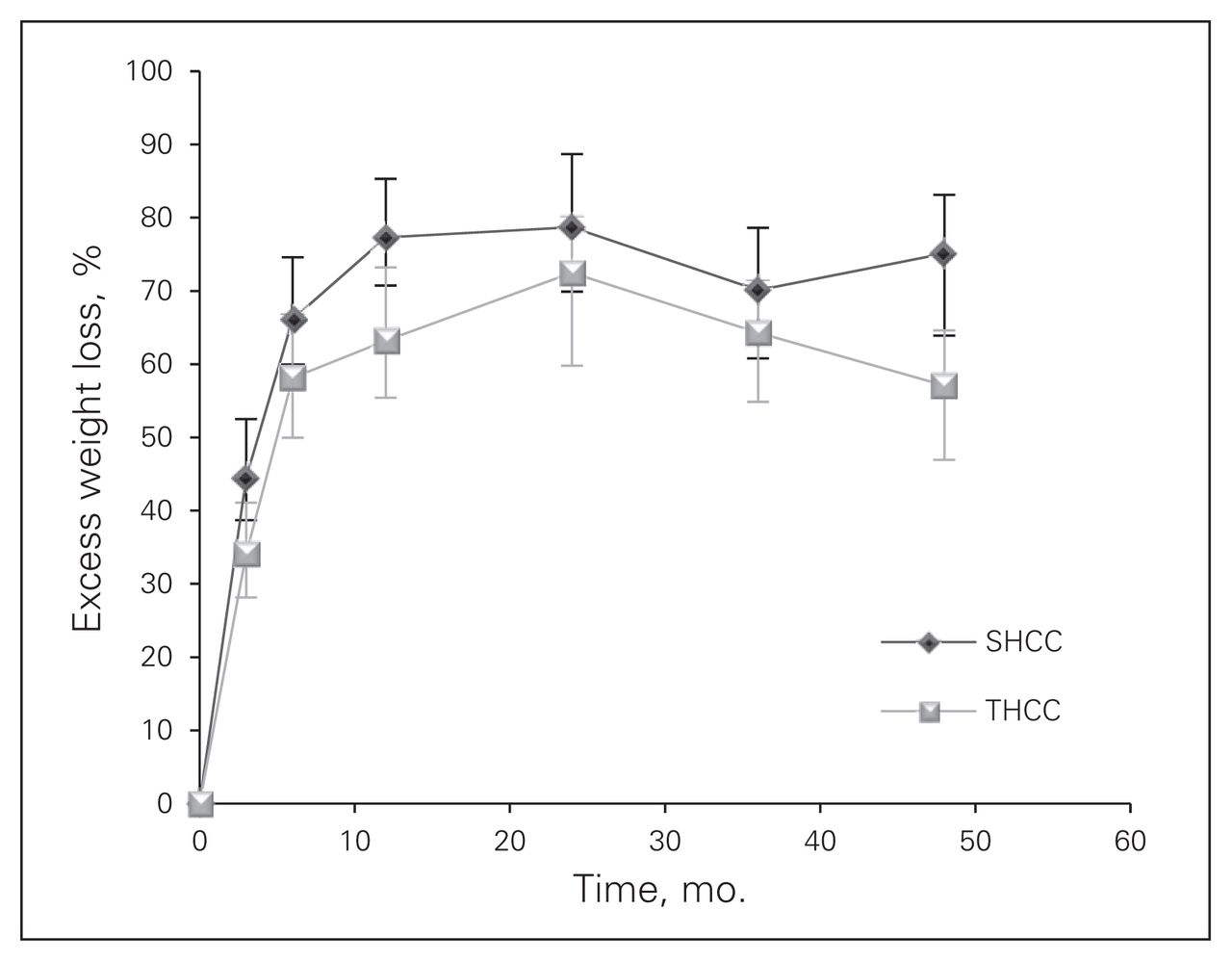
Percent excess weight loss in patients with laparoscopic gastric bypass at each site. Mean and standard deviation are shown as well as the number of cases followed-up at each time point. SHCC = secondary health care centre;THCC = tertiary health care centre.
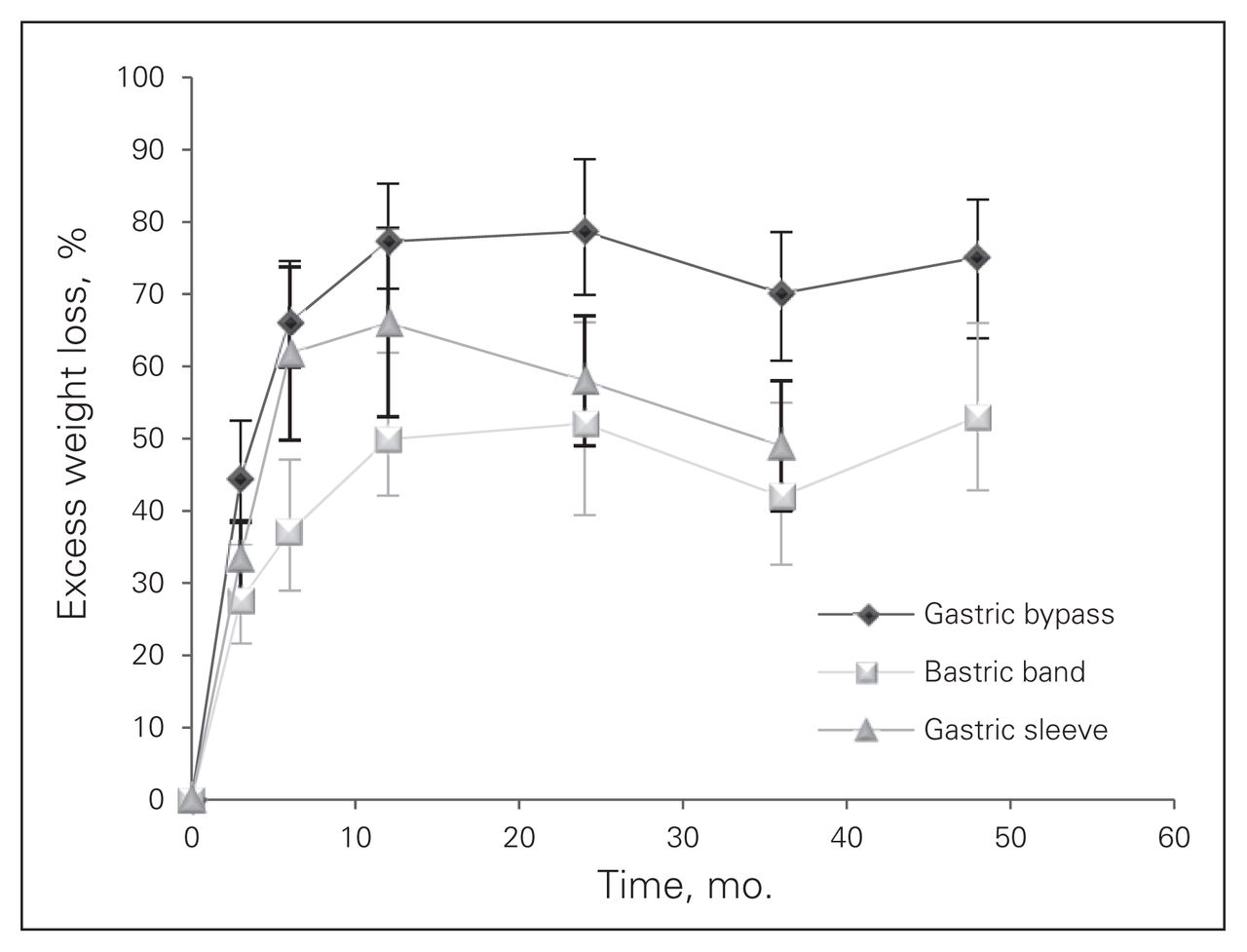
Figure 4 shows a comparison of the excess weight loss between the 3 laparoscopic bariatric surgery procedures at the SHCC (there were insufficient data to compare the 3 procedures at the THCC). Gastric bypass was associated with significantly better weight loss results than the gastric band and gastric sleeve procedures.
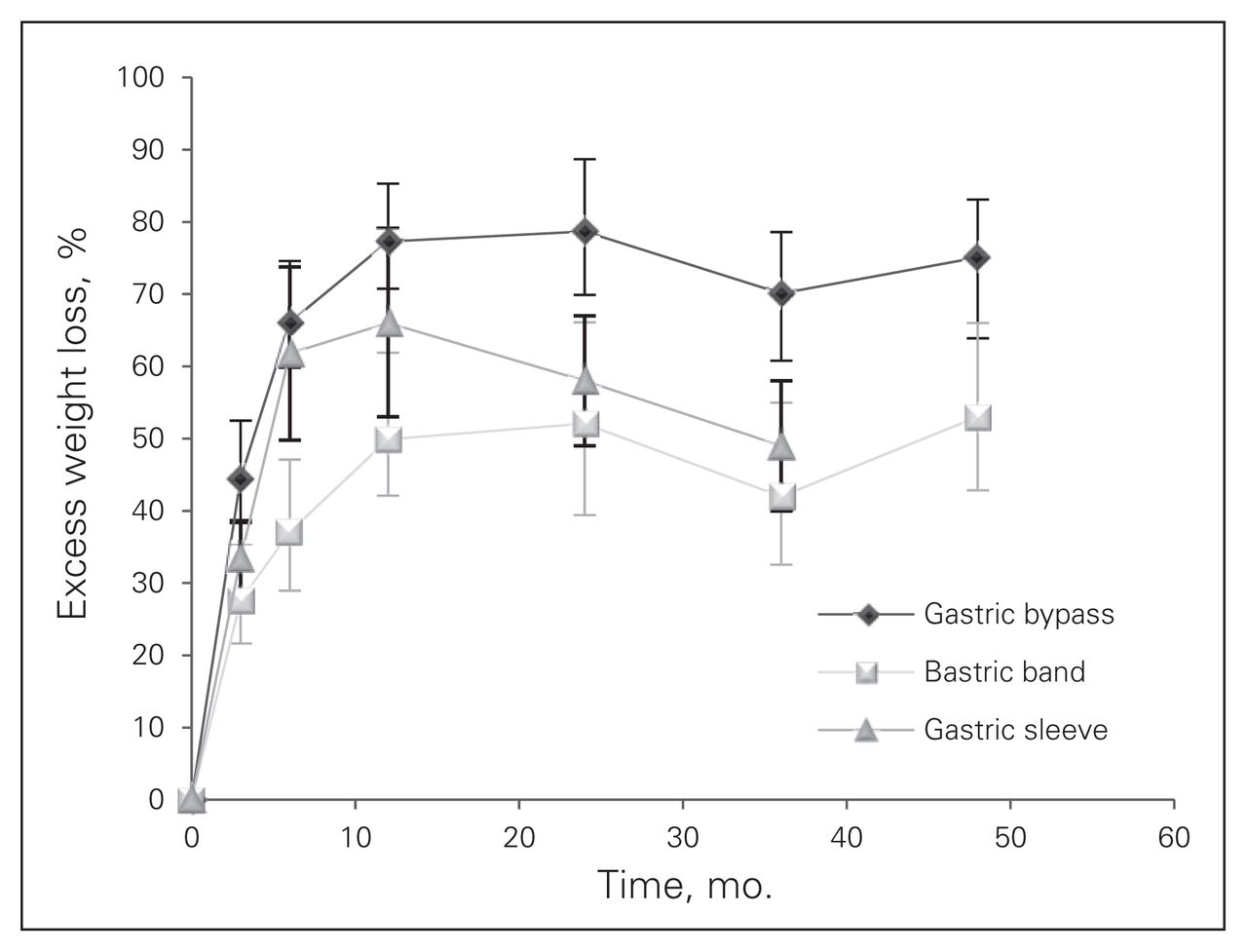
Comparison of the excess weight loss between the 3 laparoscopic bariatric surgery procedure sat the secondary health centre (insufficient data to compare the tertiary health care centre. Mean and standard deviation are shown.
Discussion
The number of Canadians who are morbidly obese is estimated as 3% of 34 million (2010 data from Statistics Canada) or about 1 million people. If 10% of morbidly obese people in Canada were to request bariatric surgery to treat obesity in the next 10 years, this would mean performing about 10 000 operations per year. However, this estimate does not take into account the exponential increases in the prevalence of obesity and type 2 diabetes that have been projected for the coming 10–20 years.19
A recent survey of centres known to perform more than 20 bariatric surgical procedures per year conducted by the MUHC team provides the best available data on the volume of bariatric surgery in Canada.12 The survey results showed that the 12 Canadian centres that responded performed 1313 procedures in 2007. Given that 6783 patients were waiting for bariatric surgery, the authors estimated the wait time for bariatric surgery in Canada to be 5.2 years.
The Ontario Ministry of Health and Long-Term Care stated in their December 2005 report that the province should increase its bariatric surgery capacity to at least 3500 surgeries per year, as did the AETMIS recommendation. This latter report, released in 2005, recommended that that the province of Quebec substantially increase its capacity for bariatric surgery from 716 operations per year in 2005 to more than 3500 by 2012 to meet demand.
Since the release of these reports, Ontario has increased bariatric surgery capacity in the public system to an estimated 2085 per year in 2011, and Quebec has increased capacity to an estimated 1757 per year. Both estimates are below the targets. The present study was initiated to determine if one of the AETMIS report recommendations could be implemented: the strategy of designating several SHCCs and mandating them to complete about 200 select cases of bariatric surgery each year. Each centre would be linked by a “service corridor” to a THCC within each of the 4 integrated health networks. With the addition of 10 such SHCCs (200 cases each) to the 4 THCCs (500 cases each) within Quebec’s 4 integrated health networks, the yearly bariatric surgery capacity could be increased to 4000. The SHCCs could include some specialized medical centres15 that deliver publicly funded, private delivery bariatric surgeries according to law 33 enacted in 2006. We have now collected sufficient statistics to suggest that, with proper patient selection, this approach could be feasible.
Patient selection criteria allow for safe surgery to be delivered at SHCCs with acceptable mortality and short-term and long-term complications. Overall mortality and centre-specific mortality are well within accepted values.20 Weight outcomes are also favourable. Weight loss greater than 50% of the excess weight21 and reduction of the BMI22 to less than 35 have been proposed as potential definitions of success of a bariatric surgical procedure. The medical obesity literature uses actual weight loss and percent body weight loss. The weight loss results from the present study are reported using all these outcome measures and show that the weight loss is robust and maintained for the 4 years of follow-up available in the SHCC. These results suggest superior weight loss after gastric bypass than gastric band or sleeve.
Limitations
This study has several limitations. It represents the personal series of 1 experienced bariatric surgeon’s minimally invasive laparoscopic bariatric surgery practice, which is well beyond the learning curve for bariatric procedures.23 As such, there is no surgeon- or technique-related variability. Less experienced surgeons may not be able to duplicate these results. This is why it is imperative to select the SHCC very carefully and provide adequate training to the preoperative, perioperative and postoperative teams and surgeons who will be caring for these patients. This is not a randomized study and, as such, it is subject to all the potential bias of a prospective cohort study. The perioperative follow-up was adequate, and no deaths or life-threatening complications could have been missed. Despite determined efforts of long-term follow-up for all patients, this was not successful. Finally, resolution and improvement of comorbidities were not included in the analysis, as the aim of this study was to concentrate on weight loss and morbidity and mortality assessment.
Conclusion
With proper patient selection, a well-trained, dedicated health care team and a “service corridor” to an affiliated THCC, laparoscopic bariatric surgery, including gastric bypass, can be performed safely in an SHCC. This service model warrants more study to determine whether it can be widely applied across Canada.
Footnotes
Presented in part at the Canadian Surgery Forum in London, Ont., Sept. 15–18, 2011.
Competing interests: None declared.
- Accepted July 30, 2012.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.