

Abstract
Background: We sought to investigate the altered brain responses to emotional stimuli in patients with schizophrenia.
Methods: We analyzed data from 14 patients with schizophrenia and 14 healthy controls who performed an emotional face matching task. We evaluated brain activity and connectivity in the amygdala and cortical regions during the initial (first 21 seconds of each stimulation block) and sustained (last 21 seconds) stages of an emotional processing task, and we determined changes in amygdala activity across the emotional processing task.
Results: The patients with schizophrenia showed similar amygdala activation to the controls during the initial stage of processing, but their activation decreased during the sustained stage. The controls showed increasing amygdala activity across the emotional blocks, whereas activity progressively decreased in the schizophrenia group. The patients with schizophrenia showed increased cortical activity and interconnectivity in the medial frontal and inferior parietal cortex in the initial stage of emotional processing. There was increased activity in the superior temporal cortex and greater connectivity with the inferior parietal cortex in the sustained stage. Performance accuracy was lower in the schizophrenia group in the first part of the block, while their reaction time was longer in the latter part of the block.
Limitations: It was not possible to specify the moment at which the switch in amygdala response occurred.
Conclusion: Our findings suggest that patients with schizophrenia have an initial automatic emotional response but that they need to switch to a compensatory cognitive strategy to solve the task.
Introduction
Judgment of facial affect is crucial for optimal social functioning. It involves both automatic and controlled evaluative processing, which require different cognitive resources and engage discrete brain areas.1 In schizophrenia, a deficit in facial affect recognition has often been reported.2,3 However, the nature of this impairment is not clear. Several studies suggest that, in schizophrenia, there may be a dissociation between the automatic response and the conscious judgment to emotional stimuli. For instance, although the literature consistently reports a deficit in patients’ ability to identify facial emotions, normal or even increased automatic processing of facial affect has been demonstrated by physiologic evaluation and by studies of priming or attentional allocation.4,5
The neural substrates of facial affect recognition in schizophrenia are also unclear, notably for the activity of the amygdala, a crucial brain nucleus implicated in emotional processes. Whereas the majority of neuroimaging studies in schizophrenia have demonstrated decreases in amygdala activity,6–13 2 studies have shown an increased response of the right amygdala to happy,14 fearful and neutral faces.15 These differences across different studies may be related to differences in symptomatology and the medications used. However, a further potential factor could be a shift between automatic and conscious judgment of emotional stimuli over time in patients with schizophrenia.
We based this hypothesis on 3 main observations. First, simple presentation of emotional material normally causes an automatic emotional experience.16 Second, emotional experience is often reported to be exaggerated in patients with schizophrenia.17–19 And third, a careful assessment of the neuro imaging literature reveals that only studies using a design with blocks shorter than 28 seconds have reported amygdala activation in schizophrenia.14,15
We believe that a heightened automatic emotional response could interfere with basic emotional processing and subsequently require compensatory strategies to make emotional judgments. We have shown in a previous study6 that, during performance of an emotional recognition task, patients with schizophrenia resort to alternative cognitive strategies consisting of the use of a feature-based analysis to identify facial emotions, implying deactivation of amygdala. Our objective in the present study was to test the hypothesis that schizophrenia patients show a shift in their amygdala response during emotional tasks (i.e., initially normal amygdala activity followed by a decrease).
On the basis of data reporting an association between abnormal amygdala activity and impairment of emotional recognition in schizophrenia,20 we also hypothesized that this pattern would reflect the need to resort to alternative cognitive mechanisms as a result of a primarily inefficient emotional reaction, in particular the use of a cognitive strategy based on the analysis of individual features.6
To test this, we reanalyzed part of a data set from a previous study,6 in which we found that when schizophrenia patients and healthy controls were confronted with a task requiring judgment of emotional stimuli (labelling emotional expressions), both groups had a similar downregulation of limbic brain activity in the prefrontal cortex. Unlike healthy controls, however, schizophrenia patients seemed to continue to use this strategy when confronted with a task normally involving instinctive and automatic emotional processing (matching faces with emotional expressions). We concluded that the patients with schizophrenia were resorting to a cognitive strategy to perform the emotional recognition task. In the present study, we examined only data concerned with matching, because this task normally requires automatic and intuitive processing and shows differences between schizophrenia patients and healthy participants. We conducted 2 complementary analyses: we evaluated both initial and sustained brain responses during each emotional block of the matching task compared with the control task, and we explored changes in amygdala activity throughout each matching block. We also examined differences between the groups in brain cortical and subcortical connectivity and behavioural performance during each stage of emotional processing.
Methods
Participants
We included 14 right-handed patients with a DSM-IV21 diagnosis of schizophrenia. Patients were recruited from the psychiatry department of Sainte Marguerite Hospital in Marseille. Two psychiatrists established the diagnoses after independent assessments performed at least 1 year before study entry and at study entry. The sample consisted of both outpatients12 and inpatients,2 and all were receiving stable antipsychotic treatment at the time of the study (i.e., they had been receiving the same antipsychotic drug at the same dosage for at least 6 weeks). Most patients were taking atypical antipsychotics (amisulpride 3, risperidone 3, olanzapine 3 and aripiprazole 2), but 3 patients were taking conventional antipsychotics (haloperidol). We based our psychopathological assessment on the Positive and Negative Syndrome Scale (PANSS; Table 1).22
Clinical and demographic characteristics of schizophrenia patients and health controls
The schizophrenia patients underwent 2 separate interviews to ensure that they fully understood the study. In the first interview, the investigator described the study and gave to the patient a written synopsis. In the second interview, the schizophrenia patients (and any person who accompanied the patient) were given the opportunity to ask questions about the study. After clarification of all issues and after the investigator judged the patient to have sufficient knowledge and understanding of the study, the patient was asked to read and sign a consent form.
Schizophrenia patients were matched to 14 healthy controls for handedness, sex, age and parents’ socio-economic status (expressed as the highest level of education completed by either parent). The healthy participants had no history of psychiatric or neurologic disease. They also had no history of drug abuse and were not taking psychotropic medication.
This study was conducted in accordance with the principles of the declaration of Helsinki. Approval was obtained from the local ethics committee (Comité consultatif de protection des personnes dans la recherche biomédicale, Marseille). Each participant was registered with the French national file and gave informed written consent before entering the study.
Study design
The experimental design was described in detail in our previous study.6 Briefly, the design included 2 emotional tasks (matching and labelling) and a simple sensorimotor control task. Here, we report data from the matching task only, because this is the only task to have previously shown differences between schizophrenia patients and healthy people. Human faces depicting angry or fearful expressions were presented to the participants, who were asked to select which of the 2 faces presented on the same screen expressed the same emotion. As a control task, participants viewed a target oval shape and chose which of 2 ovals matched the target exactly.
The whole experiment consisted of 2 sessions of 12 blocks, 3 blocks each of either matching or labelling facial emotion (44.5 s duration each) interleaved with 6 control blocks of 22 seconds’ duration; the interblock interval was 2 seconds. The total scan length was 14:03 minutes. For each emotional condition, 60 different images were used, all derived from the Karolinska database.23 Images were presented for 4 seconds with an interstimulus interval of 0.5 seconds. The design was counterbalanced across participants.
Magnetic resonance imaging and processing
We acquired data using a 3-T MedSpec 30/80 AVANCE imager (Bruker). Stimuli were back-projected onto a screen that the participants viewed though a mirror. Functional magnetic resonance imaging (fMRI) scans were acquired using a T2-weighted gradient-echoplanar sequence (repetition 3000 ms, echo time 35 ms, field of view 19.2 × 19.2 cm, matrix 64 × 64, flip angle 90°). In all, 36 interleaved axial slices were obtained with a contiguous slice thickness of 3 mm.
Data analysis
We processed the data using SPM2 (www.fil.ion.ucl.ac.uk/spm/). The first 12 seconds of each session, corresponding to signal stabilization, were discarded. The remaining scans were corrected for differences in slice acquisition time. Head movement was corrected, and we added movement parameters as confounding covariates in the statistical analysis if they exceeded 1.5 mm or 1.5° or both. Data were rejected if the movement in any axis was greater than 3 mm or 3° or both. All images were spatially normalized and smoothed with an isotropic Gaussian kernel (6 mm).
Initial and sustained block activity
To assess differences in initial and sustained activation in the matching blocks, each emotional block was divided in 2 parts of equal length, giving a design matrix with 3 conditions: “initial emotional” (consisting of the first 21 seconds of the emotional block), “sustained emotional” (consisting of the last 21 seconds) and “control.” The 2.5 seconds remaining in the middle of the emotional block were discarded from the analysis. The longest length of block in previous studies reporting amygdala activity in schizophrenia patients was 28 seconds. Because we used blocks of 44.5 seconds, we decided to divide the original block into two 21-second semiblocks; this ensured a minimal adequate block-length in the fMRI design. Individual statistical maps were calculated to evaluate the differences between each stage of the emotional condition and the control in the whole brain.
We were especially interested in the activity of the amygdala and the neocortical areas that we have previously demonstrated to be implicated in the compensatory cognitive strategy of feature-based stimulus processing used by schizophrenia patients.6 These areas included the bilateral amygdala (right: Talairach coordinates for the centre of the cluster 21 −2 −16, volume 904 mm3; left: −24 −4 −17, 616 mm3), left inferior parietal (IPC; −35 −60 43, 14792 mm3), left middle temporal (MTC; −49 0 −14, 328 mm3) and bilateral medial frontal (BMFC; −1 15 52, 3376 mm3) cortex.
Therefore, for the second-level analysis, we used a region-of-interest (ROI) approach. The ROI was derived from the original within-group results of whole brain activity by adding all clusters that showed task changes in both schizophrenia patients and healthy controls in the aforementioned regions. We then performed a random-effects ROI analysis to establish the pattern of each group in each task. The significance threshold was set at p < 0.05 (false discovery rate [FDR]–small volume corrected). We also conducted between-group analyses using the same ROIs and a random-effects approach. The significance threshold was set at p < 0.05 (FDR–small volume corrected).
Functional connectivity
To evaluate between-group differences in the interactions between different ROIs, we analyzed functional connectivity for each part of the matching block. This allowed us to compare the coactivity of these regions between schizophrenia and healthy participants separately for each emotional processing state.
We evaluated 6 separate ROIs: right amygdala (Talairach coordinates for the centre of the cluster 21 −2 −16, volume 904 mm3), left amygdala (−24 −4 −17, 616 mm3), left IPC (−35 −60 43, 14 792 mm3), left MTC (−49 0 −14, 328 mm3), bilateral posterior BMFC (−2 19 48, 3776 mm3) and anterior BMFC (−16 56 12, 208 mm3).
We extracted the time series for each region using the MarsBaR toolbox. We extracted the adjusted data separately from each part of the emotional block in the entire fMRI protocol and performed a correlational analysis. We evaluated the main effects and interactions of group and stage of the matching group (initial or sustained) for correlations between regions.
Individual correlation indices between regions were then submitted to 2 between-group analyses, one for each emotional stage, to test the null hypothesis that path coefficients were identical in schizophrenia and healthy participants. Because the conditions of normality (analyzed by use of the Shapiro–Wilk test) were met, parametric t tests were carried out by use of SPSS version 11.0. Statistical significance was set at p < 0.05 (FDR-corrected for multiple comparisons).
Parametric analysis of amygdala activity during the matching task
An additional parametric analysis, focused on the amygdala, was conducted to evaluate differences between the 2 groups of participants in terms of increasing and decreasing activity throughout the whole emotional matching block. We defined the design matrix using a parametric vector, ranging from 1 to 10, which modulated each block. The increasing vector was arbitrarily assigned a maximum value of 10, because 10 stimuli were presented in each block. This analysis tested changes in the regional brain response throughout each emotional block. We chose not to use temporal modulation as a parametric factor because we predicted an effect on the evaluation of each successive emotional stimulus in a block, rather than on the time taken to complete the experiment as a whole. Direct random-effects comparisons between the 2 groups were also conducted. The previously calculated amygdala ROI was used. The significance of threshold was set at p < 0.05 (FDR–small volume corrected).
Behavioural performance
We compared the accuracy scores, number of omitted responses and reaction times in each stage of the emotional task between schizophrenia patients and healthy participants. Nonparametric independent-samples Mann–Whitney tests from SPSS were used for accuracy and omitted responses because these variables were not normally distributed. For reaction time, however, the data were normally distributed, and a Student t test was used. Statistical significance was set at a threshold of p < 0.05.
Correlations between clinical symptoms (PANSS scores) and accuracy scores were also examined.
Results
Brain activity
Within-group effects
Healthy participants showed bilateral activation of the amygdala and medial frontal cortex, as well as activation of the left inferior parietal cortex, for both the initial and sustained parts of the block. They also showed activation of the left cingulate gyrus in the initial part of the block.
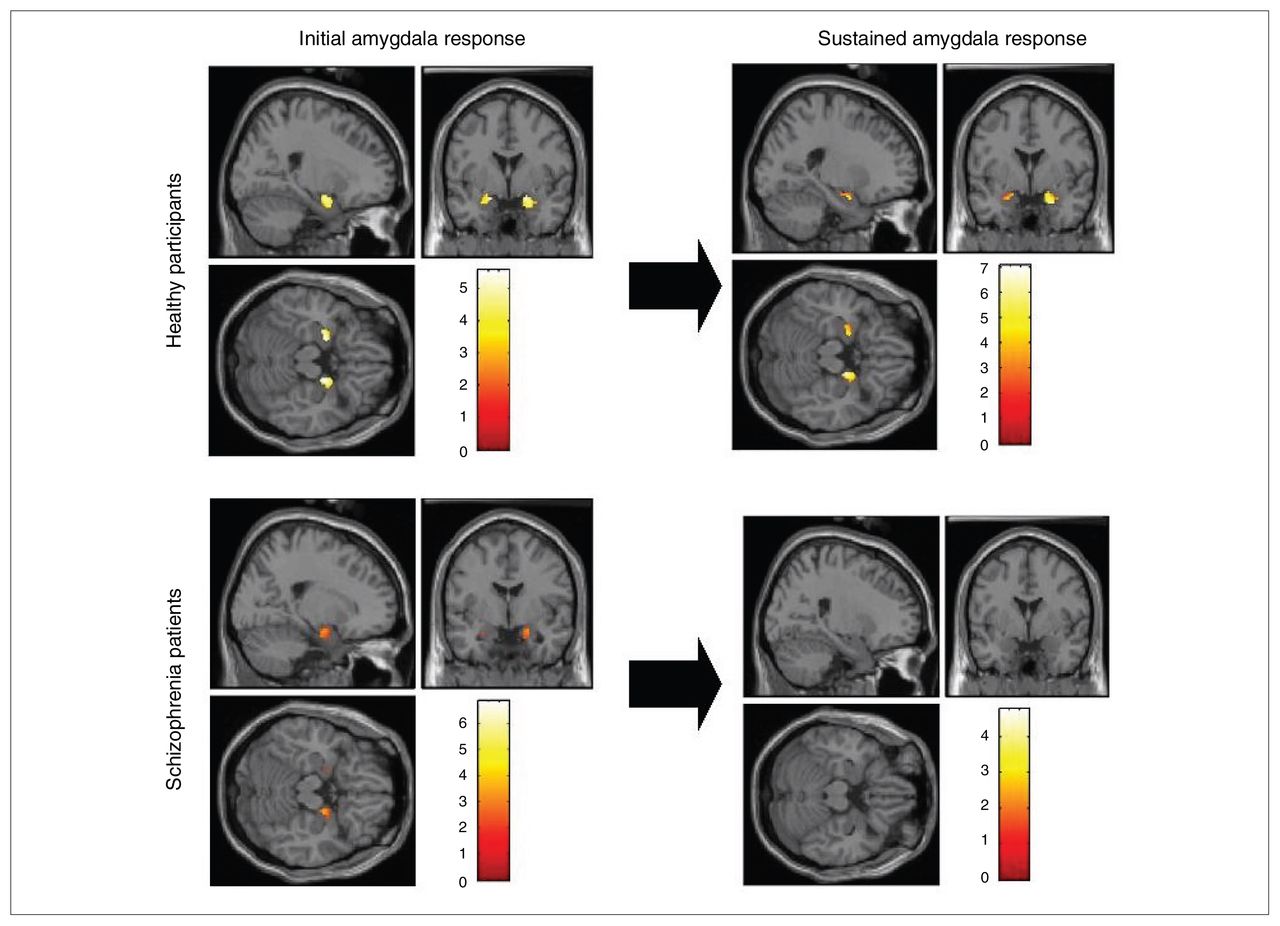
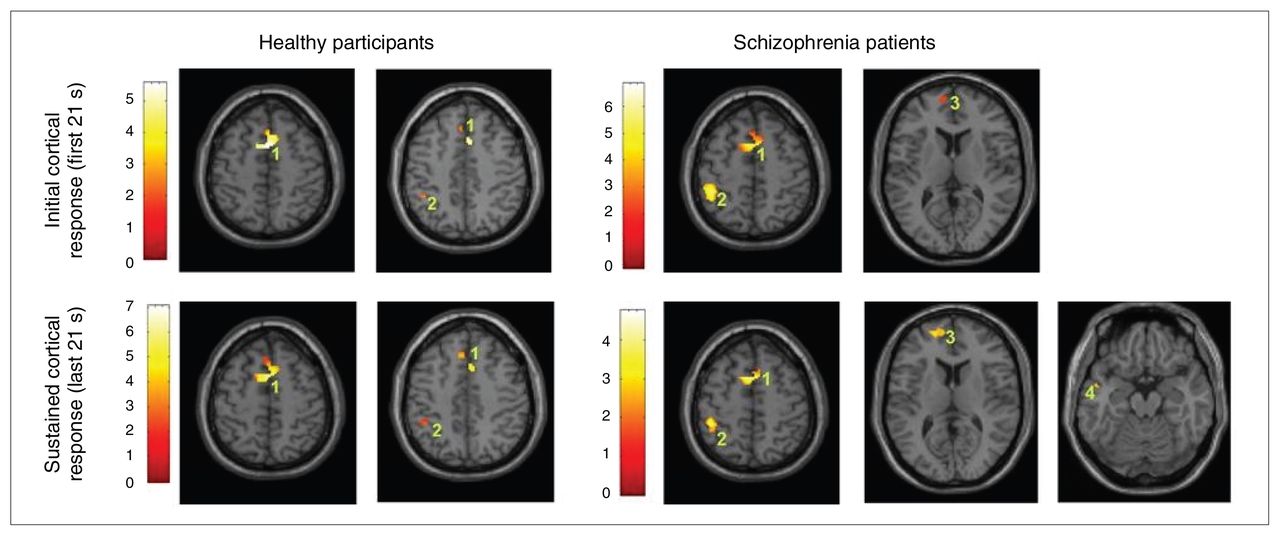
Schizophrenia patients showed significant activation in the bilateral amygdala only during the initial part of the block (Fig. 1). Activity of the bilateral medial frontal gyrus and left inferior parietal cortex was observed in the schizophrenia group for both parts of the block. Schizophrenia patients showed additional activation in the superior temporal cortex in the sustained part only (Fig. 2).

Individual patterns of the initial (the first 21 seconds of the emotional block) and sustained (the final 21 seconds of the block) amygdala response in each group of participants.

Individual patterns of initial and sustained cortical responses in each group (1: medial frontal gyrus, Brodmann area 6; 2: inferior parietal cortex, Brodmann area 40; 3: medial frontal cortex, Brodmann area 10; 4: middle temporal gyrus, Brodmann area 21).
Between-group effects
There was similar activation in the amygdala across groups in the initial part of the emotional block, but decreased activity bilaterally in the amygdala in the schizophrenia group in the sustained part of the emotional block (Table 2).
Brain activity responses across regions of interest during the initial (first 21 seconds of the emotional block) and the sustained (final 21 seconds of the block) performance of the facial emotional recognition task
Compared with healthy participants, schizophrenia patients had increased activity in the left IPC, BMFC and MTC in both parts of the block.
Functional connectivity
A main effect of group was found in the correlation between left BMFC and IPC (F1 = 6.68, p = 0.013), bilateral posterior dFG and IPC (F1 = 5.33, p = 0.025), bilateral posterior dFG and MTC (F1 = 5.5, p = 0.023) and IPC and MTC (F1 = 4.81, p = 0.033).
An interaction between stage of emotional processing and group was found for the correlation between left IPC and MTC (F1 = 4.12, p = 0.047).
A greater positive correlation between left BMFC and IPC was observed among schizophrenia patients than among controls in the initial part of the block (t26 = 2.88, p = 0.008, mean correlation for healthy participants = 0.04, mean correlation for schizophrenia patients = 0.22). In the sustained part of the block, the schizophrenia patients showed a greater positive correlation between left IPC and MTC (t26 = 2.65, p = 0.014, mean correlation for healthy participants = −0.04, mean correlation for schizophrenia patients = 0.18). There were no greater correlations in the healthy participants compared with schizophrenia patients in any part of the block.
Parametric activity changes in the amygdala
The healthy participants showed a greater increase in activity in the bilateral amygdala throughout the block than did schizophrenia patients (right: Talairach coordinates 18 −7 −15, t = 3.14, p FDR-corrected = 0.014; left: −18 −6 −16, t = 3.62, pFDR-corrected = 0.014). The schizophrenia patients, relative to healthy participants, showed greater decrease in activity in the bilateral amygdala (right: 18 −5 −14, t = 2.83, pFDR-corrected = 0.042; left: −19 −4 −22, t = 3.29, pFDR-corrected = 0.037).
Behavioural performance
In the initial part of the emotional block, healthy participants had greater accuracy scores than did the schizophrenia patients. There was no difference between groups in the sustained part of the block. Schizophrenia patients omitted more responses than did healthy participants in the initial part of the block, but there was no difference between groups in the sustained part. For reaction time, the groups did not differ in the initial part of the emotional block, but longer reaction times were found in the schizophrenia group during the sustained part (Table 3).
Behavioural performance of participants in the initial and sustained parts of the emotional blocks
Positive correlations were found between negative symptoms and percentage of omissions in both the initial (r = 0.6, p = 0.03) and the sustained (r = 0.55, p = 0.04) stage of emotional processing.
Discussion
The central findings of the present study were, first, that there were similar degrees of amygdala activation in healthy and schizophrenia participants during the initial stages of emotional processing, but that there was decreased amygdala activation in patients with schizophrenia during the sustained stages. Second, we found increased cortical activity in schizophrenia patients compared with in healthy participants in both the initial and sustained stages of emotional processing. Third, in contrast with amygdala activation, we found significantly lower accuracy scores in the schizophrenia group than in the healthy group in the initial part of the block, but there were similar scores in the sustained part. Conversely, the reaction time was longer in the schizophrenia group in the sustained part of the block only.
The most interesting finding was the observation that, compared with healthy participants, schizophrenia patients initially showed normal activation of the amygdala, but that this activation was diminished in the sustained part of the emotional block. This result is exemplified by the activity in each half of the block and was confirmed by the more pronounced decrease in activation throughout the emotional matching block, as revealed by the parametric analysis, in the schizophrenia group than in the healthy group.
Amygdala activation in the initial part of the block suggests that patients with schizophrenia initially process the first few emotional stimuli automatically, although probably in co-occurrence with cognitive processing, as indicated by the abnormally increased cortical recruitment. However, this automatic processing is reversed over time in favour of cognitive evaluation, with consequent decreases in amygdala activity. This hypothesis is consistent with the observation that schizophrenia patients displayed increased reaction times only during the last part of the emotional block. Together, these observations suggest that in the initial part of the block, schizophrenia patients predominantly use a rapid, implicit, amygdala-mediated pathway for processing emotional facial expressions, but that they use a more voluntary, strategic, cortically mediated pathway in the sustained part.
The pattern of cortical dominance in the patient group includes DFC and left IPC (as well as the correlation between them) during the initial stages of the block, and an additional engagement of MTC (and its correlation with IPC) in the later stages. The frontal–inferior parietal network is implicated in maintaining a state of alertness to salient facial stimuli and has an important role in the control of spatial attention.24,25 The superior and middle temporal gyri have consistently been implicated in feature analysis of facial stimuli.26,27 Our results are thus in keeping with our previous hypothesis that patients with schizophrenia resort to a compensatory cognitive strategy, based on a feature-based analysis of emotional faces, and that this strategy is not immediately useful but is only used when the automatic response is turned off. The use of this feature-based strategy, implicating temporal lobe regions, has also been reported in people with a damaged amygdala.26
In patients with schizophrenia, this strategy seems to be more efficient than the initial automatic emotional response, because accuracy scores were inversely related to the intensity of amygdala activation. This result is consistent with a recent event-related fMRI study showing that in healthy participants, greater amygdala activation was associated with the correct identification of facial emotions, whereas in schizophrenia patients, greater amygdala activation predicted a failure to identify anger and fear.20 The efficiency of this cognitive strategy has been suggested in a social–cognitive training study, in which the improvement in emotional recognition of schizophrenia patients entailed a redirection of visual attention to relevant features of emotional faces.28
The exact reasons why the initial automatic emotional response is inefficient in schizophrenia patients cannot be determined from our study. A consistent body of evidence emphasizes that patients with schizophrenia may have higher sensitivity to negative emotions than healthy participants.17–19 Moreover, higher levels of autonomic arousal to facial emotions have been observed in schizophrenia patients although their limbic activity appears reduced.13,29 A possible explanation for these data could be that, during emotional processing of threat-related emotions, schizophrenia patients engage alternative cognitive routes to avoid a potentially exaggerated automatic emotional reaction. However, in the absence of physiologic correlates, this interpretation should be treated with caution.
The deactivation of the amygdala observed in the sustained stage of emotional processing in our patients with schizophrenia is unlikely to be a consequence of a lack of sustained attention, because performance accuracy improved in the same time frame. Moreover, although the normal amygdala response rapidly habituates to emotional face presentation,30,31 we believe that the decreasing amygdala activity in schizophrenia patients was not because of habituation or extinction effects for 3 reasons: 1) all stimuli used in our task were different; 2) it has been shown that, unlike healthy participants, schizophrenia patients do not display habituation effects in the amygdale–hippocampus complex when passively presented with repetitive presentation of facial emotions;32 and 3) an additional analysis carried out (Appendix 1, available at www.cma.ca/jpn) to evaluate possible habituation effects throughout the entire experiment revealed no differences in brain activity between the beginning and end of the fMRI session for either initial or sustained parts of the block.
Limitations
A limitation of our study is that we were unable to specify the moment at which the switch in amygdala response occurred. Also, the use of antipsychotic medication could influence our results. However, we aimed to examine patients receiving stable antipsychotic treatment because medication is the habitual condition of most patients and therefore reflects their general day-to-day life and because we wanted to compare our results to previous neuroimaging studies, which have also involved patients taking medication. Moreover, the emotional response observed in patients not taking medication seems analogous to that observed in those taking medication.33,34
Conclusion
Our findings suggest that patients with schizophrenia initially show normal activity in the amygdala, which is then down -regulated compared with the activity in controls. This latter decrease in amygdala activity occurs concurrently with an increase in accuracy scores and reaction times, suggesting that schizophrenia patients resort to compensatory cognitive strategies based on the analysis of facial features. This idea is supported by the observation that the schizophrenia patients engaged more of the prefrontal and parietal cortex than did healthy participants during emotional processing, along with a major contribution from the MTC during the sustained part of the task. We postulate that patients with schizophrenia initially have a normal automatic response to emotional faces but that this initial reaction is inefficient, so they then prioritize cognitive evaluation to solve the emotional recognition task.
Acknowledgements
This study was supported by grants from the French National Center for Scientific Research and the Instituto de Salud Carlos III, Centro de Investigación Biomédica en Red de Salud Mental. The authors thank the group of Centre IRMf de Marseille for their technical support in image acquisition, as well as Jennifer Coull and Peter Mckenna for their correction of the English text. The authors also thank Raimon Salvador for providing statistical advice.
Footnotes
Competing interests: None declared.
Contributors: All authors designed the study, reviewed the written article and approved its publication. Drs. Salgado-Pineda, Fakra and Delaveau acquired the data, which Dr. Salgado-Pineda analyzed. Drs. Salgado-Pineda and Fakra wrote the article.
- Received February 13, 2009.
- Revision received July 9, 2009.
- Revision received August 31, 2009.
- Accepted September 3, 2009.
References
In this issue

{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.