


A 33-year-old man with a history of intravenous drug use presented to the emergency department with fever, rigors, cough and malaise of seven days’ duration. He had been injecting heroin for five years and was known to be hepatitis-C positive. On physical examination, he appeared acutely ill with a fever of 39.5°C, moderate respiratory distress (respiratory rate 26 breaths/min, oxygen saturation 94%) and basilar rales over his right lung. He had a painful nodular skin lesion on his left arm corresponding to an injection site and track marks on both arms. His leukocyte count was 29.1 (normal 4.0–10.5) × 109/L, hemoglobin level was 120 (normal 130–175) g/L, platelet count was 83 (normal 140–450) × 109/L, alanine transaminase level was 104 (normal 5–40) U/L and C-reactive protein level was 108.4 (normal < 10) mg/L. A peripheral-blood smear showed extracellular and intracellular budding yeasts being phagocytized by neutrophils. The yeast forms consisted of pseudohyphae and blastospores (Figure 1; Appendix 1, available at www.cmaj.ca/cgi/content/full/cmaj.101947/DC1).
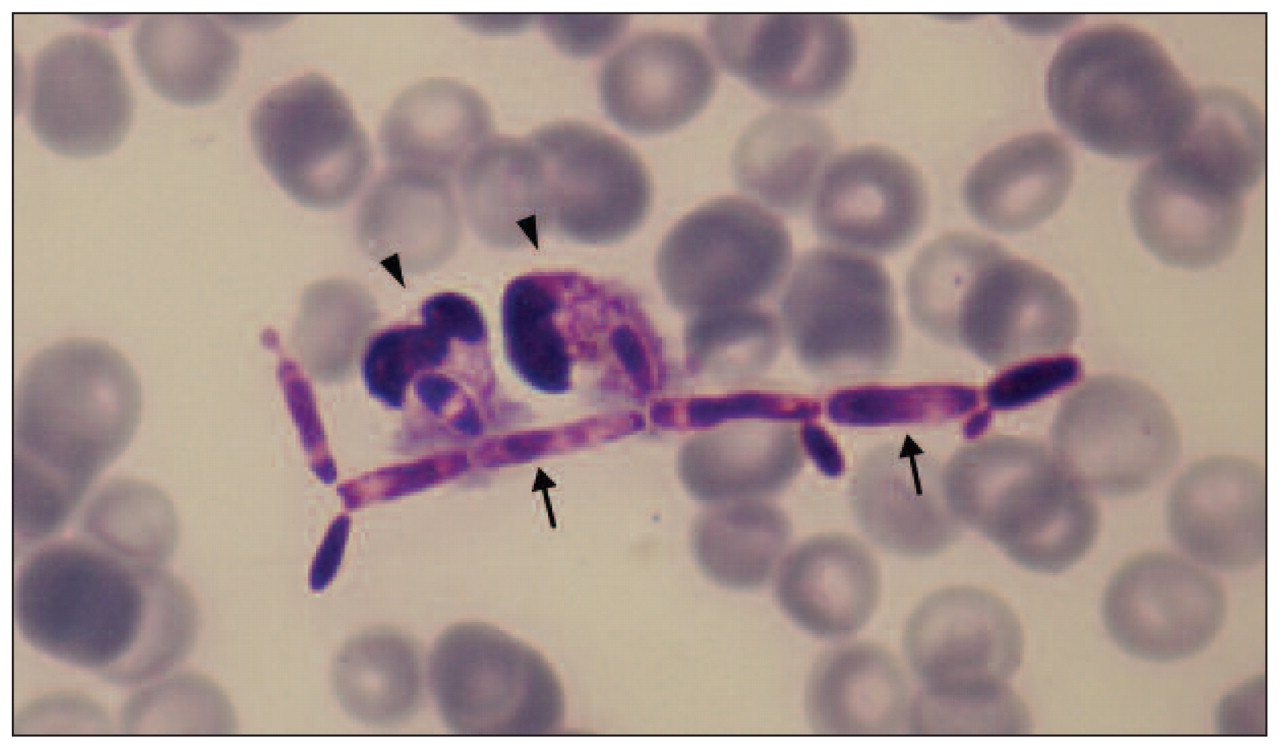
Peripheral-blood smear from an acutely ill 33-year-old man with a history of intravenous drug use, showing branched pseudohyphae (arrows) and two neutrophils in the process of phagocytizing fungal elements (arrowheads) (May–Grünwald, original magnification × 1000).
After gathering blood and urine cultures, we started the patient on liposomal amphotericin B. Computed tomography showed three nodular opacities affecting the patient’s right lung and a small hypodense lesion in his left kidney. Trans-esophageal echocardiography and ophthalmologic evaluation were unremarkable. Two days later, Candida parapsilosis was isolated in blood and urine cultures, and serologic tests came back positive for antibodies against the hepatitis C virus and negative for HIV. After 15 days of treatment with amphotericin B, our patient received a two-week course of fluconazole. One month later, he had no signs of residual or recurrent infection.
Injection drug users are at increased risk for blood-borne invasive bacterial and fungal infections.1 Deep candidiasis is the most frequent invasive fungal infection among this group, although its precise incidence is unknown. Candidiasis may be disseminated or confined to one organ, frequently presenting as endocarditis or endophthalmitis.1,2 Its pathogenesis involves mycotic contamination of drug paraphernalia (e.g., reused syringes) or contaminated drug solutions (e.g., through lemon juice used as an acidic solvent for brown heroin and crack cocaine).2
Candidemia in a peripheral-blood smear occurs only when fungal elements are present in high concentrations, in the range of 1–5 × 106 CFU/mL, and is therefore associated with high-grade infection and increased mortality.3,4 Because most candidemic episodes are characterized by much lower fungal loads, peripheral-blood smears play a limited role in early detection of disease.4
Footnotes
-
Competing interests: None declared.
-
This article has been peer reviewed.
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

