


Abstract
Background: Fine needle aspiration biopsy represents the critical initial diagnostic test used for evaluation of thyroid nodules. Our objectives were to determine the cytological distribution, the utility of clinicopathologic characteristics for predicting malignancy and the true proportion of cancer among individuals who presented with indeterminate cytology and had undergone thyroid surgery for suspicion of cancer.
Methods: We retrospectively reviewed 1040 consecutive primary thyroid operations carried out over an 8-year period at a tertiary care endocrine referral centre. Follicular neoplasm (FN), Hürthle cell neoplasm (HN), neoplasms suspicious for but not diagnostic of papillary carcinoma (IP) and neoplasms with cellular atypia (IA) were reviewed.
Results: In all, 380 individuals presented with cytologically indeterminate thyroid nodules. Of these, 252 (66%) patients had FN, 47 (12%) HN, 44 (12%) IP, 26 (7%) IA and 11 (4%) had mixed diagnoses. Biopsied lesions were found to be malignant on pathological evaluation in 102 (27%) patients: 49 (19%) with FN, 11 (23%) HN, 28 (64%) IP and 9 (35%) with IA. Hemithyroidectomy was adequate definitive treatment in 196 of 225 (87%) patients with FN and 39 of 42 (93%) with HN. Significant associations with a cancer diagnosis were identified for smaller tumour size in patients with FN (p = 0.004) and right thyroid lobe location in patients with IP (p = 0.012), although these factors were nonsignificant in the corrected analyses for multiple comparisons.
Conclusion: In a review of the experience at a Canadian centre, 4 operations were carried out to identify each cancer, and hemithyroidectomy was the optimal initial and definitive surgical approach for most patients.
Thyroid nodules are common in the general population; they are identified in about 5% of patients by palpation and 50% by ultrasound examination.1 Fine needle aspiration biopsy (FNAB) represents the critical initial diagnostic test used for evaluation of thyroid nodules. However, in a large number of patients, the distinction between benign and malignant thyroid nodules has remained challenging for clinicians. In a review of more than than 18 000 thyroid FNABs carried out at the Mayo Clinic in Rochester, Minn., FNAB had a reported sensitivity of 83%, specificity of 92% and accuracy of 95%.2 Furthermore, in up to 15% of patients, the preoperative diagnosis of cancer was classified as indeterminate or suspicious for cancer.2–6 Indeterminate cytological diagnoses occur for follicular patterned thyroid lesions owing to overlapping cytomorphologic characteristics of benign and malignant lesions.2,3 In these patients, pathologic evaluation of the tumour specimen is required to identify additional tumour characteristics, such as the presence of capsular or vascular invasion, for an accurate diagnosis of cancer. Furthermore, the cytological evaluation of FNAB specimens of papillary carcinoma can often be challenging owing to differences in the interpretation of the required threshold of nuclear change for a cancer diagnosis.6 The major diagnostic criteria for papillary thyroid carcinoma (PTC) include an irregular and enlarged nucleus, eccentric micronucleoli, fine chromatin, longitudinal nuclear grooves and intranuclear pseudoinclusions. However, thyroid FNAB specimens can have some, but not all, of the features required to fulfill the cytological diagnostic criteria required for a cancer diagnosis. Such lesions may be classified as being “suspicious” or “highly suspicious” for cancer.4 There is also substantial inter- and intraobserver variability in cytological and pathological assessment of follicular patterned thyroid lesions.7
Thus, when an individual presents with a thyroid nodule and an FNAB cytological diagnosis of Hürthle cell neoplasm (HN), or an aspirate suspicious for papillary carcinoma, the current recommended approach of the American Thyroid Association is removal of either a portion of or the entire thyroid gland.8 Furthermore, in patients with follicular neoplasms (FN) diagnosed by FNAB, radioiodine thyroid imaging may be considered, and a diagnostic lobectomy or total thyroidectomy is recommended especially in individuals with nonfunctioning nodules.8 Total thyroidectomy carries a low but increased risk of permanent hypoparathyroidism and the need for lifelong calcium supplementation as well as increased risk for bilateral recurrent laryngeal nerve dysfunction and subsequent possible need for a lifelong tracheostomy compared with thyroid lobectomy. Some individuals will also require lifelong thyroid hormone replacement therapy. Surgical series have reported malignancy rates of 13%–30% for patients with FN9–13 and 21%–42% for those with HN.14–16
At our centre, a thyroid lobectomy and isthmusectomy is performed as the initial operation for patients with an indeterminate cytological diagnosis and no clinical evidence of regional or distant metastatic disease or any other concurrent indication for total thyroidectomy (i.e., goitre, Graves disease). If gross extrathyroidal tumour extension or lymph node metastasis is found at the time of operation, a total thyroidectomy is then carried out. Intraoperative frozen section examination is not used in our management approach for FN or HN, but may be used for other cytologically indeterminate nodule types at the discretion of the operating surgeon. Consistent with the current literature, in prior reports of our experience, only about 1 in 5 patients undergoing thyroid operation for FN or HN were eventually found by histopathologic evaluation to have cancer.17,18 Hemithryoidectomy was considered to be adequate definitive treatment in 96% of individuals with FN and 82% with HN diagnosed preoperatively with FNAB cytology.
The present study was carried out with the aim of evaluating our current algorithm for the surgical treatment of thyroid nodules in a large prospectively collected patient cohort. Thus, our review represents a real-world experience of the treatment of thyroid nodules at a regional Canadian tertiary endocrine surgical referral centre. The aim of the study was to determine the optimal surgical approach for individuals presenting with a cytologically indeterminate thyroid nodule. We sought to determine the cytological distribution, the utility of clinicopathological characteristics for predicting malignancy and the true proportion of cancer among individuals with indeterminate cytology who undergo thyroid operation.
Methods
We retrospectively reviewed a prospectively maintained database of 1040 consecutive primary thyroid operations performed over an 8-year period (January 2000 to July 2008) at St. Paul’s Hospital in Vancouver, British Columbia. Individuals presenting with 1 or more thyroid nodules with indeterminate cytology by FNAB who had undergone thyroid lobectomy or total thyroidectomy were included in the study. Indeterminate cytology was defined as FN, HN, suspicious for but not diagnostic of papillary carcinoma (IP) and cellular atypia (IA). Cellular atypia refers to nonspecific nuclear changes on cytology that do not reflect any of the previous categories. A small number of patients presented with cytological diagnoses of FN and IP in separate FNAB specimens, and they were categorized as having “mixed diagnoses.” Each of these FNAB cytological groups carries a different probability for malignancy,4 and thus each group was analyzed and discussed separately. This study was conducted with ethics approval from the Providence Health Care and University of British Columbia Research Ethics Boards.
Statistical analysis
We compared clinicopathological characteristics between patients with final pathological diagnoses of benign and malignant thyroid lesions, and associations with a cancer diagnosis were determined using Mann–Whitney U and χ2 tests; we considered results to be significant at p < 0.05.
Results
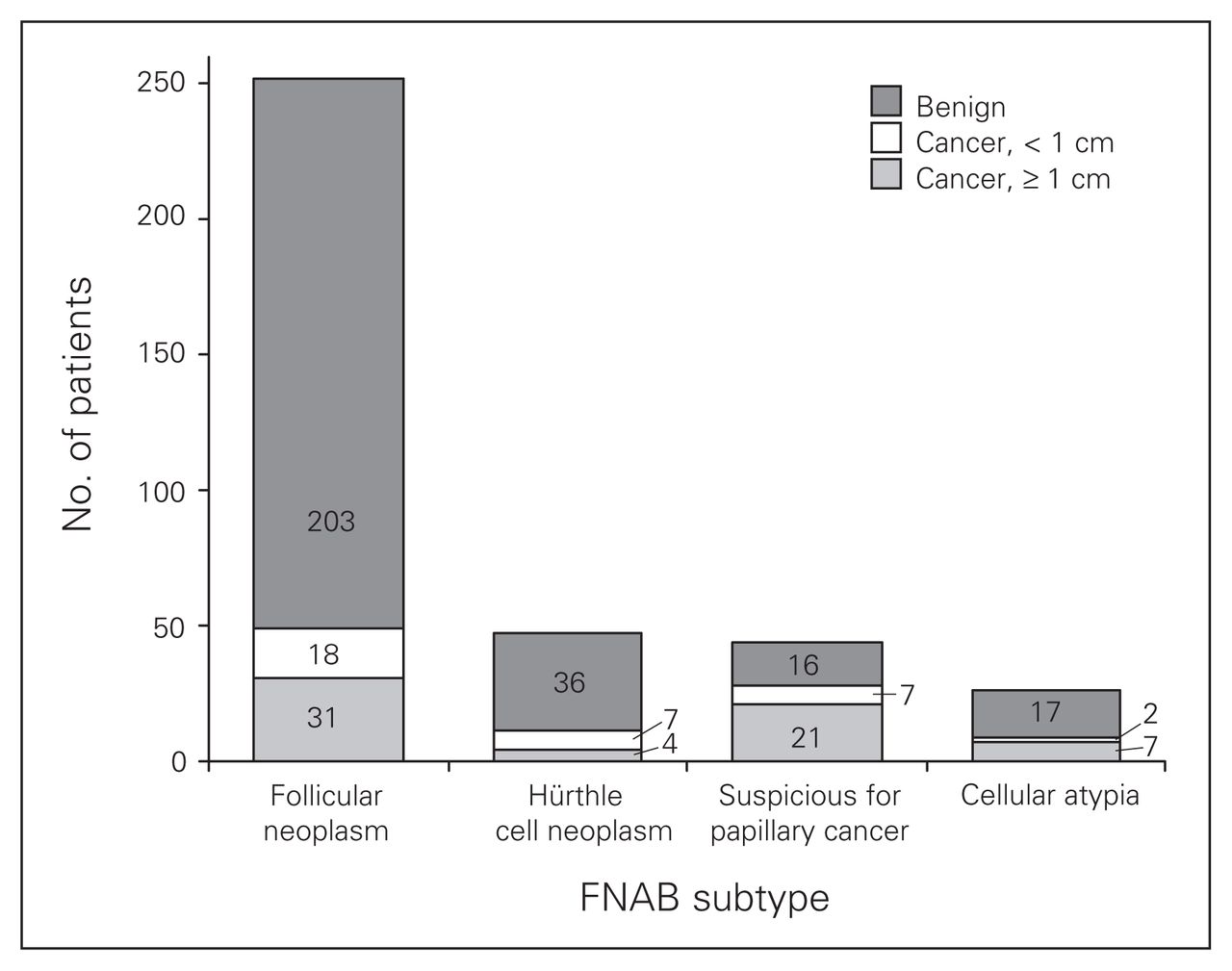
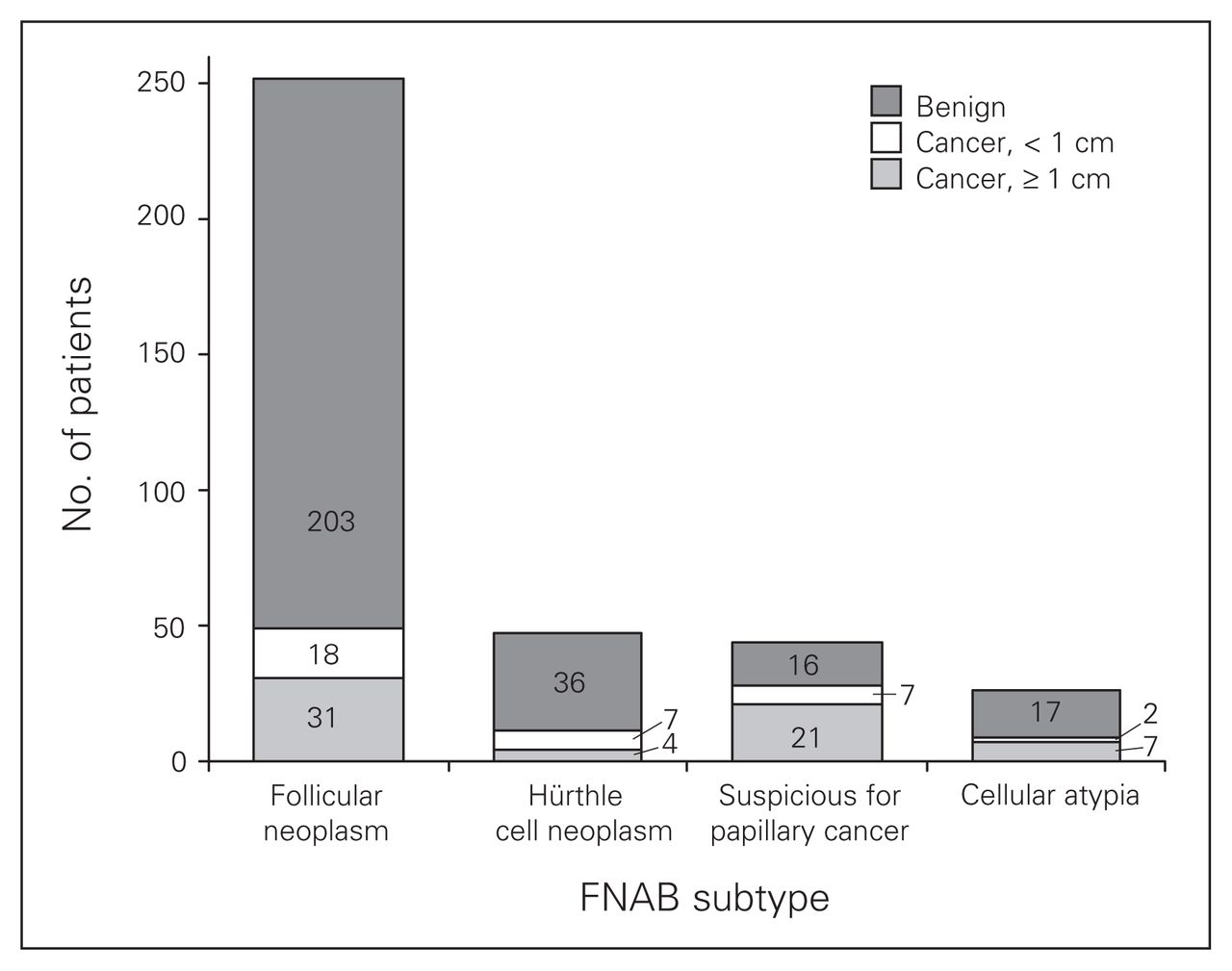
During the study period, 1040 primary thyroid operations were performed at our centre. In all, 380 (37%) patients presented with an indeterminate FNAB diagnosis. Of these patients, 252 (66%) had FN, 47 (12%) HN, 44 (12%) IP, 26 (7%) IA and 11 (3%) had mixed diagnoses. The cytological distribution of the indeterminate cases is presented in Figure 1. All patients underwent surgical resection according to our management algorithm. By pathological examination, cancer was identified in 49 (19%) patients with FN, 11 (23%) with HN, 9 (35%) with IA and 28 (64%) with IP (Fig. 2).

Cytologic distribution of 380 patients presenting with indeterminate fine needle aspiration biopsy thyroid nodules.
Pathologic results for patients with indeterminate fine needle aspiration biopsy (FNAB) diagnoses of thyroid lesions.
Among patients presenting with indeterminate FN cytology, 49 of 252 (19%) had tumours that were determined to be malignant on pathological evaluation. Of these, there were 11 with follicular carcinomas (FTC), 2 with Hürthle cell carcinomas (HTC), 1 with medullary carcinoma (MTC) and 35 with papillary carcinomas (PTC). Of the 35 patients with PTCs, 18 (51%) had papillary thyroid microcarcinomas (PTMC; tumour of less than 1 cm in maximal diameter) and 13 of these 18 (72%) PTMCs were associated with a benign dominant nodule (Fig. 3). Although we cannot determine whether the preoperative FNAB specimens were derived from the PTMC or an associated dominant nodule or both, we suspect that most PTMCs were incidental findings.
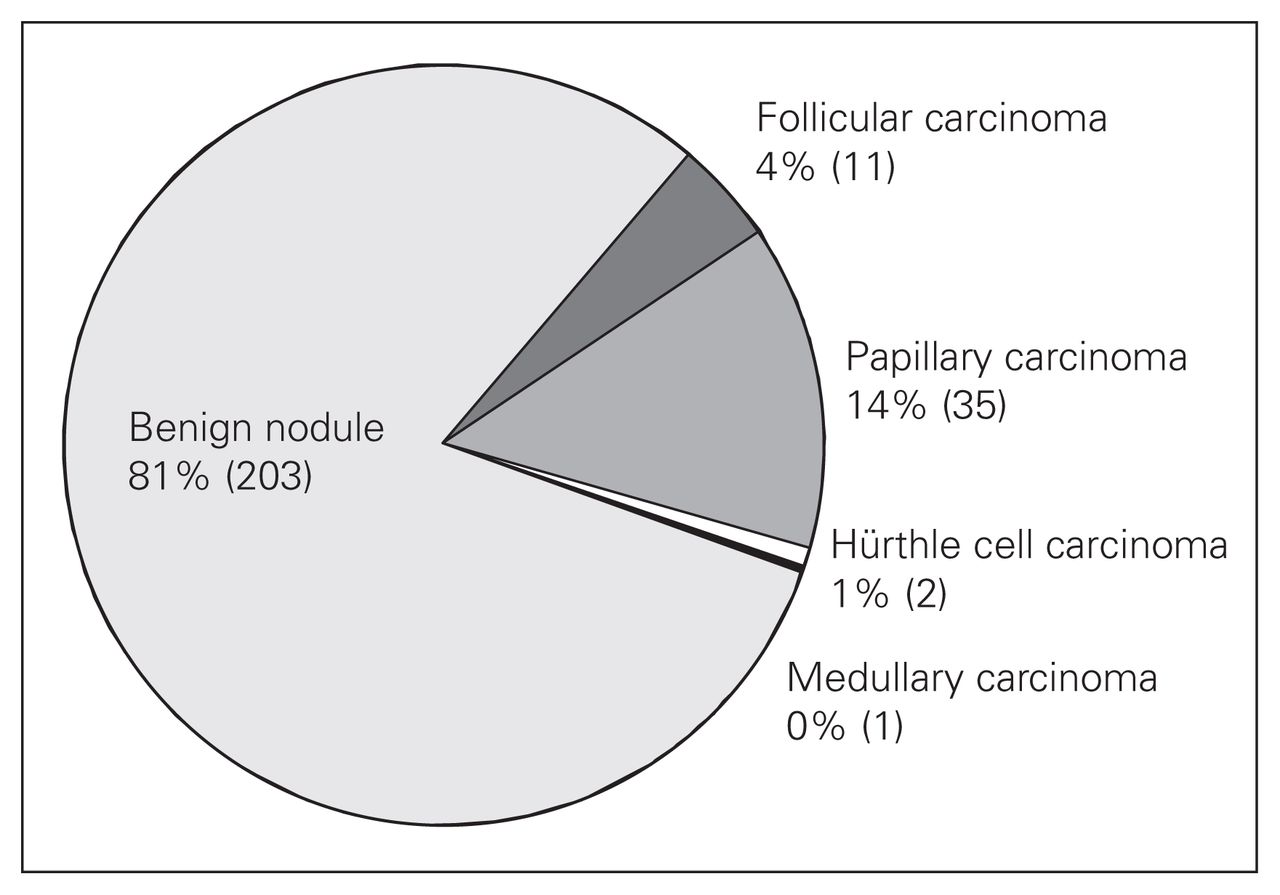
Pathologic diagnoses of 252 patients with follicular thyroid neoplasms undergoing surgery for suspicion of cancer.
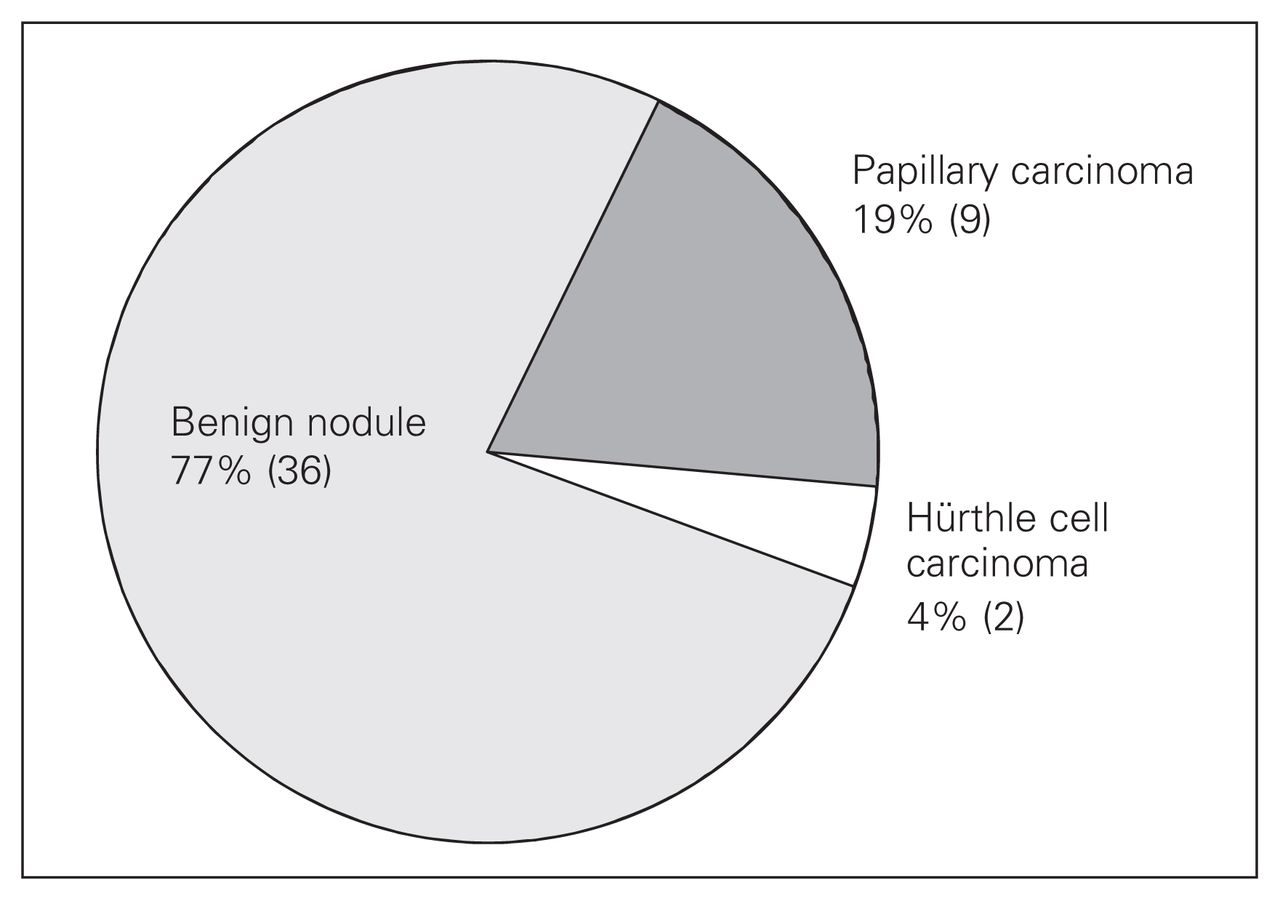
There were 47 patients with HN in our study cohort, 11 (23%) of whom had tumours that were found to be malignant on pathologic examination. Of these, 2 were HTCs, 9 were PTCs, and 7 of the 9 (78%) PTCs were PTMCs (Fig. 4).
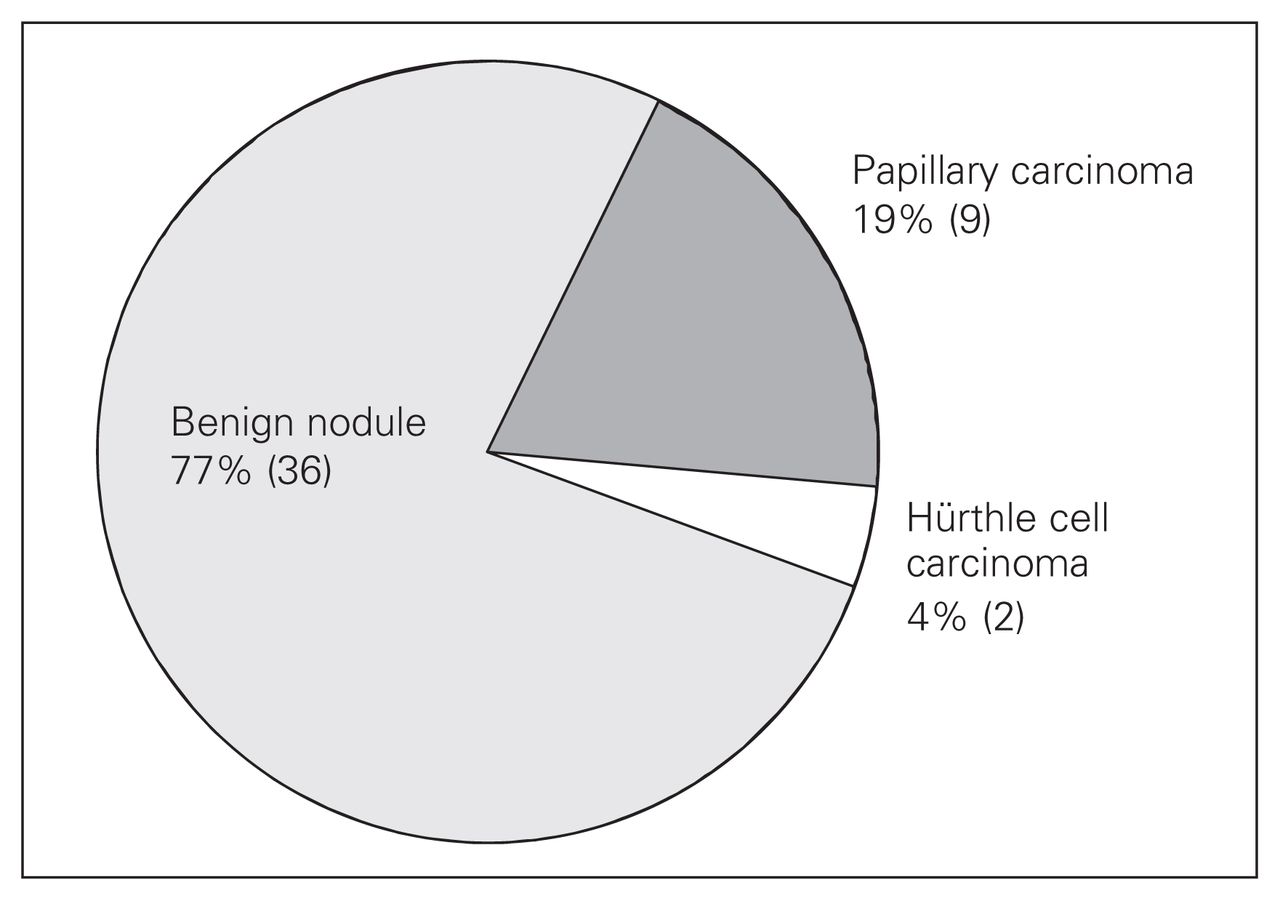
Pathologic diagnoses of 47 patients with Hürthle cell thyroid neoplasms undergoing surgery for suspicion of cancer.
Most patients (28 of 44, 64%) with an IP diagnosed by FNAB were found to have cancer. Intraoperative frozen section consultation was performed at the discretion of the operating surgeon. Intraoperative frozen section was used in 25 of 41 (61%) patients. The specimens were found to be malignant in 9 (36%) patients and benign in 5 (20%), and 11 (44%) patients had their diagnoses deferred to final pathologic evaluation. Data on the use of intraoperative frozen section were unavailable for 3 patients.
In the 26 patients presenting with a cytological IA thyroid nodule, 9 (35%) were found to have cancer on pathologic evaluation. These included 3 patients with FTCs and 6 with PTCs (of which 2 were PTMCs).
The clinicopathological characteristics of the study cohort are presented in Table 1. Individuals with preoperative diagnoses of FN, HN and IP were evaluated for patient and nodule characteristics predictive of cancer. Patients with PTMCs were included in the calculation, as the diagnosis of incidental PTMC still represents an important finding for subsequent management and follow-up. Significant associations with a cancer diagnosis were identified for smaller tumour size (mean of 2.16 cm for cancers and 3.04 cm for benign specimens, p = 0.004) in patients with FN and for left thyroid lobe tumour location (p = 0.012) for patients with IP. No other clinicopathological parameters (including age, sex, tumour laterality, size of tumour, gland nodularity and location of tumour) reached statistical significance for the cytological groups analyzed. Furthermore, no clinicopatholgical factors evaluated were significant for cancer diagnosis after Benjamini–Hochberg correction. A summary of these findings is presented in Table 2.
Clinicopathological characteristics of patients with indeterminate fine needle aspiration biopsy diagnoses
Results of univariate analysis of clinicopathological characteristics and a cancer diagnosis
Papillary thyroid microcarcinoma generally has a good prognosis and, unless multifocal or associated with aggressive characteristics (e.g., lymph node metastases), does not require a completion thyroid lobectomy.19 Excluding the 5 patients with multifocal PTMCs, hemithyroidectomy was considered adequate treatment in 196 of 252 (78%) of patients with FN and 39 of 47 (83%) of those with HN. Of these, 27 patients with an FN diagnosis and 5 with an HN diagnosis underwent a total thyroidectomy at their initial operation for a concurrent indication of goitre or intraoperative evidence of gross extrathyroidal tumour extension and/or nodal metastases. In the FN cohort, there were 188 benign nodules, 13 PTMCs (5 multifocal), 12 PTCs greater than 1 cm, 9 FTCs, 1 MTC and 2 HTCs. In the HN cohort, there were 34 benign nodules, 6 PTMCs (1 multifocal), 1 PTC and 1 HTC. Of the patients with cancer treated at our centre, the recommendation for completion thyroidectomy and adjuvant radioactive iodine therapy was determined by tumour histology, patient characteristics, and willingness to undergo further surgery.8,20–22
Discussion
Fine needle aspiration biopsy is currently the critical initial test for the preoperative assessment of individuals presenting with nodular thyroid disease. Even though it has proven clinical utility in guiding the surgical treatment of thyroid tumours, follicular patterned thyroid lesions have remained a diagnostic challenge.
Numerous adjunctive tools have been investigated for their diagnostic utility in thyroid cancer management, including use of clinicopathological scores, ultrasound characteristics and molecular markers. Clinicopathological parameters have formed the foundation for commonly used thyroid cancer risk group prognostic indices and, thus, for determining utilization of postoperative adjuvant therapy. The AGES score was developed at the Mayo Clinic and uses patient age, tumour grade, tumour extent (extrathyroidal tumour extension or distant metastasis) and tumour size for categorization of individuals at low and high risk for disease recurrence and death.23 Similarly, AMES, a risk assessment system developed at the Lahey Clinic in Burlington, Mass., uses patient age, tumour metastases, capsular or extrathyroidal tumour involvement and tumour size for disease prognostication.24 In a similar fashion, investigators have attempted to identify clinicopathological characteristics that will aid in the preoperative distinction between benign and malignant thyroid nodules.12,25–28 Reports have shown varied results. Characteristics that have been reported to be of clinical utility in predicting malignant pathology have included male sex, large nodule size, nodule fixation, solitary nodules, hard nodules and extremes of patient age. However, other groups have not found these, or any other clinicopathological characteristics, to be useful predictors of a cancer diagnosis.9,29
In the present study, smaller tumour size was significantly associated with a cancer diagnosis, although it was nonsignificant in the corrected analyses for multiple comparisons. This is in sharp contrast to prior reported surgical series. In the FN cohort, 203 patients had benign and 49 had malignant disease. Papillary thyroid microcarcinoma accounted for 18 of the 49 cases of thyroid cancer and was associated with a dominant benign nodule in 13 cases. Thus, the study findings must be interpreted in the context of these “incidental” findings of PTMC. In a study by Baloch and colleagues12 involving 122 patients undergoing thyroid resection with a cytologically diagnosed FN between 1998 and 2000, 37 (31%) patients were classified as having malignant disease on pathological assessment. Lesions that were 3 cm or greater were significantly associated with a cancer diagnosis. In an earlier report by Tuttle and colleagues28 involving 149 individuals with FN in the period 1990–1995, 103 patients underwent thyroid resection and 22 (21%) cancers were found in their cohort. Nodule size greater than 4 cm by palpation was predictive of cancer. Reasons for the opposite observations in the present study may reflect a trend toward increased detection of smaller thyroid cancers with more widespread use of gland imaging. As a result, thyroid cancers are identified at a smaller size, including nodules that are otherwise not detectable by clinical examination.
Although patient age has been consistently used as a prognostic indicator for thyroid cancer risk stratification systems, the association between age and preoperative diagnosis of malignancy in individuals with indeterminate cytology has remained unclear. In a study by Tyler and colleagues26 involving 81 patients with cytologically indeterminate thyroid nodules, cancer was identified in 9 of 10 (90%) patients with IP lesions, 8 of 43 (19%) with FN and 5 of 18 (28%) with HN. Patient age older than 50 years was significantly associated with an increased risk of cancer. In contrast, Schlinkert and colleagues25 reported that younger patient age predicted malignancy in a cohort of 19 patients with FTCs among 219 patients with a diagnosis of FN who underwent thyroid surgery at the Mayo Clinic. Furthermore, in a study of 215 patients with FN in a Korean centre, cancer was identified in 102 individuals (29 PTCs, 57 FTCs, 15 HTCs and 1 PMC). In this group, patient age younger than 20 years or older than 60 years was significantly associated with a final pathologic diagnosis of cancer.27
Patient sex has also been extensively studied as a potential predictor of increased cancer risk in patients with indeterminate thyroid nodules. In the studies by Baloch and colleagues12 and Tuttle and colleagues,28 male sex was found to be significantly associated with increased cancer risk (47% for men v. 29% for women, p < 0.001 and 43% for men v. 16% for women, p = 0.007, respectively). However, other investigators have not found a similar association.9,29
Explanations for the variations in study results may arise from differences in cytological and pathological procedures and assessments carried out at those centres as well as differences in tumour epidemiology at different study locations. Furthermore, the rarity of patients presenting with HN (47 of 380 [12%] patients in our series) and HTC (5 of 380 [1.3%] patients in our series) makes identification of important clinical diagnostic tools a challenge. Currently, there has been no single or combination of patient clinical characteristics that can reliably differentiate benign from malignant thyroid tumours.
Ultrasonographic features have also been investigated for their potential ability to identify cancer in individuals presenting with thyroid nodules.30,31 In a retrospective review of 849 thyroid nodules with available cytological or pathological diagnoses, ultrasonographic features that were found to be associated with cancer were taller than wide, had irregular margins, were hypoechogenic and had the presence of micro- and macrocalcification.32 However, in a report by Jeh and colleagues33 involving 127 patients with PTC and 23 with FTC, radiological findings reported to be predictive of carcinoma were commonly found in patients with PTC but inconsistently found in those with FTC. Furthermore, other investigators have reported conflicting results.34
The results of the present study should be interpreted with the recognition that the referral bias and the selection bias are inherent in most published surgical series. The number of patients that were not referred for surgical consultation or who deferred operation is not known. Thus, the true proportion of cancers among patients with indeterminate FNAB may be under- or overestimated in the present report. A recent study by Kihara and colleagues49 reported on 445 individuals presenting with a thyroid nodule and undergoing thyroidectomy for FNAB diagnosis of benign or follicular neoplasm: 125 patients were observed for a mean of 73.8 months (range 18.3–258.0 mo) before surgical resection, and cancer was found in 8 (6.4%) patients, which compared with 37 of 320 (11.6%) patients who underwent immediate thryoid resection for diagnosis. Immediate surgery was recommended for suspicious ultrasound features, elevated serum thyroglobulin, autonomously functioning tumours or symptomatic tumours.
Recently, the molecular characterization of thyroid tumours has shown promising results for the identification of clinically applicable diagnostic markers for malignancy. In particular, in the largest thyroid cancer diagnostic marker panel study reported to date to our knowledge, 100 benign and 105 malignant thyroid tumours were evaluated by our group for the expression of a panel of 57 different molecular markers.35 The application of a panel of molecular markers to FNAB specimens would have led to 91% of patients with indeterminate FNABs receiving correct diagnoses preoperatively. In particular, many studies have focused on thyroid tumour expression of Galectin-3 and have shown its utility in distinguishing benign and malignant thyroid tumours using pathologic and FNAB specimens.36–42 In a recent multicentre study by Bartolazzi and colleagues,39 the evaluation of Galectin-3 expression on preoperative FNAB specimens showed a sensitivity of 78%, specificity of 93% and accuracy of 88% for distinguishing benign and malignant thyroid tumours in patients presenting with cytological diagnosis of “follicular lesions” or “suspicious follicular tumours.” Preoperative testing for Galectin-3 levels in human serum43,44 and radio-labelled immunologic detection of Galectin-3 in murine thyroid cancer models45 are other novel techniques for improving preoperative thyroid cancer diagnosis that are currently under investigation.
During the review of our experience with thyroid FNAB, there were large variations in the data presented in cytology reports received from different centres and even from pathologists at our own institution. In a prospective comparative study by Tsan and colleagues,46 the implementation of a standardized cytological reporting system with defined diagnostic categories resulted in improved operating characteristics of FNAB for management of nodular thyroid disease. In particular, carcinoma was accurately identified in 100% of FNAB reports using synoptic reports compared with 67% of reports before its implementation. The Bethesda System for Reporting Thyroid Cytopathology47 is a standardized system for thyroid FNAB reporting that has been recently developed at the National Cancer Institute using a 6-tiered cytological classification system with associated cancer risk and guidelines for management.48
Conclusion
Despite its limitations, FNAB has remained the gold standard for the preoperative evaluation of individuals who present with nodular thyroid disease. In our review of the real-world experience at a single Canadian centre, cancer was identified in 49 of 252 (19%) patients with FN and 11 of 47 (23%) patients with HN. We found that by following our surgical algorithm, thyroid lobectomy was adequate definitive treatment for 196 of 252 (78%) patients with follicular patterned thyroid lesions. We also believe that our management protocol could potentially be improved with the utilization of a synoptic cytology reporting schema to ensure that individuals with diagnoses of thyroid nodular disease are treated in accordance with current clinical guidelines, such as those reported by the American Thyroid Association8 or the National Cancer Institute.4 Results from the present study suggest that the development of other clinically relevant diagnostic tools, such as the molecular characterization of FNAB specimens, would represent an important step forward in the management of individuals who present with an indeterminate FNAB diagnosis. Until improved diagnostic tests are available, hemithyroidectomy will remain the preferred, and usually only, surgical intervention required for the treatment of individuals who present with nodular thyroid disease and an indeterminate FNAB diagnosis.
Footnotes
Competing interests: None declared.
Contributors: C.G. Chiu was involved in data acquisition, data analysis and interpretation, manuscript drafting and statistical expertise. R. Yao and S.S. Strugnell were involved in data acquisition, manuscript revision and administrative support. S.K Chan and S.J. Jones were involved in data analysis and interpretation, manuscript revision and statistical expertise. S. Bugis, R. Irvine, D. Anderson and B. Walker were involved in data acquisition and manuscript revision. S.M. Wiseman was involved in study conception and design; data acquisition, analysis, and interpretation; manuscript revision; and supervision.
- Accepted May 4, 2011.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.