


Abstract
Background: Robotic surgery has emerged as a minimally invasive alternative to traditional laparoscopy. Robotic surgery addresses many of the technical and ergonomic limitations of laparoscopic surgery, but the literature regarding clinical outcomes in colorectal surgery is limited. We sought to compare robotic and laparoscopic colorectal resections with respect to 30-day perioperative outcomes.
Methods: The American College of Surgeons National Surgical Quality Improvement Program database was used to identify all patients who underwent robotic or laparoscopic colorectal surgery in 2013. We performed a logistic regression analysis to compare intraoperative variables and 30-day outcomes.
Results: There were 8392 patients who underwent laparoscopic colorectal surgery and 472 patients who underwent robotic colorectal surgery. The robotic cohort had a lower incidence of unplanned intraoperative conversion (9.5% v. 13.7%, p = 0.008). There were no significant differences between robotic and laparoscopic surgery with respect to other intraoperative and postoperative outcomes, such as operative duration, length of stay, postoperative ileus, anastomotic leak, venous thromboembolism, wound infection, cardiac complications and pulmonary complications. On multivariable analysis, robotic surgery was protective for unplanned conversion, while male sex, malignancy, Crohn disease and diverticular disease were all associated with open conversion.
Conclusion: Robotic colorectal surgery has comparable 30-day perioperative morbidity to laparoscopic surgery and may decrease the rate of intraoperative conversion in select patients.
The use of minimally invasive techniques in colorectal surgery is generally regarded as a safe and feasible modality with a shorter postoperative recovery time.1–4 However, laparoscopic procedures can be technically and physically challenging to perform, necessitating conversion to open approaches, particularly for rectal resections.2,5 Moreover, 2 recent randomized trials have not been able to establish that laparoscopic surgery is not inferior to open techniques.6,7 When the da Vinci Surgical System was approved for patient use in 2000, it helped address some of the ergonomic limitations of laparoscopic surgery.8 Many of the reported advantages of the robotic platform are linked to the increased instrument dexterity and degrees of articulation.9 However, it remains unclear whether these advantages translate into improved clinical outcomes.
The literature surrounding robotic colorectal surgery is limited and mostly consists of case series from individual institutions.10–19 Prior studies have demonstrated that robotic surgery is feasible and safe7,11–18,20,21 but may be associated with higher cost and longer operative duration, particularly for rectal resections.10,25 Given the single-centre reporting bias present in much of the literature, there is a need for research using multi-institutional data. The objective of our study was to compare robotic and laparoscopic colorectal resections with respect to perioperative clinical outcomes.
Methods
Data sources
We used the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) participant use files (PUF) to obtain information on all robotic and laparoscopic colorectal resections performed in 2013. The ACS-NSQIP database is a validated program that prospectively collects preoperative, intraoperative, and 30-day outcome data from participating hospitals across North America and abroad.22,23
We used the ACS-NSQIP colon-targeted file to identify all patients who underwent a robotic or laparoscopic colorectal resection based on the following Current Procedural Terminology (CPT) codes: 44204–12, 44140–7, 44150, 44155, 44157–8 and 44160. We excluded patients who underwent a combined approach that involved open techniques. Similarly, we excluded abdominal-perineal resections. We merged selected cases from the colon-targeted database with the general ACS-NSQIP main database using the unique CASEID to collect all relevant demographic, intraoperative, and postoperative information. We performed an additional subgroup analysis for rectal procedures to compare the 2 modalities in patients undergoing pelvic resections. We used the CPT codes 44145, 44146, 44147, 44207 and 44208 to classify rectal resections for the subgroup analysis. The study protocol was approved by the Research Ethics Board of The University Health Network, Toronto, Canada.
Outcome measures
Our outcomes of interest included intraoperative variables, such as operative duration, conversion rate, and transfusion requirements. Postoperative complications included ileus, anastomotic leak, pulmonary embolism, myocardial infarction, pneumonia, superficial site infection and urinary tract infection. We also analyzed overall length of stay, unplanned readmissions, reoperations and 30-day mortality.
Statistical analysis
We performed an exploratory series of univariate analyses to compare the 2 cohorts with respect to patient demographics and study outcomes. Converted cases were analyzed based on the initial approach (i.e., intention-to-treat analysis). We used a Student t test to test mean differences across groups for continuous variables and a χ2 test or Fisher exact test where appropriate for categorical variables. We also conducted a subgroup analysis of rectal resections and performed a multivariable analysis for outcomes that were found to be significantly different in the univariate regression, to adjust for potential cofounders. Regardless of statistical significance, all factors that were likely to have clinical influence on the outcome of interest were included in the multivariable model. All data analyses were carried out using SAS software version 9.4 (SAS Institute).
Results
A total of 472 robotic and 8392 laparoscopic colorectal resections were identified from the ACS-NSQIP database. Demographic and surgical characteristics as well as 30-day outcomes for all patients who underwent either a colon or rectal resection are compared in Table 1. The groups were similar in terms of age, sex, body mass index (BMI), comorbidities and functional status. In the robotic group, more patients underwent surgery for a cancer diagnosis than for other indications (p < 0.001). There was no difference between the robotic and laparoscopic approach in operative duration (190 v. 187 min, p = 0.48) or requirement for blood transfusion (8.1% v. 7.4%, p = 0.59). Of note, there was a significantly lower incidence of unplanned conversion to an open procedure within the robotic group (9.5% v. 13.7%, p = 0.008). There were no significant differences in any of the postoperative outcomes studied. The incidences of ileus (9.4% v. 10.5%, p = 0.49), anastomotic leak (3.8% v. 3.1%, p = 0.34), venous thromboembolism (0.9% v. 1.1%, p = 0.82), wound infection (4.8% v. 5.8%, p = 0.47), cardiac complication (0.6% v. 0.4%, p = 0.45), and pulmonary complication (1.9% v. 1.0%, p = 0.06) were similar between the 2 groups.
Comparison of robotic versus laparoscopic colon and rectal resection
We compared patients who underwent a rectal resection in a separate subgroup analysis (Table 2). There were 79 robotic rectal resections and 1370 laparoscopic rectal resections. There was no significant difference in any of the baseline patient characteristics. In terms of perioperative outcomes, no difference was observed in operative duration, requirement for blood transfusion, or rate of unplanned conversion. However, with respect to 30-day outcomes, robotic rectal resections had a lower incidence of ileus than laparoscopy (3.80% v. 11.18%, p = 0.039).
Comparison of robotic versus laparoscopic rectal resection
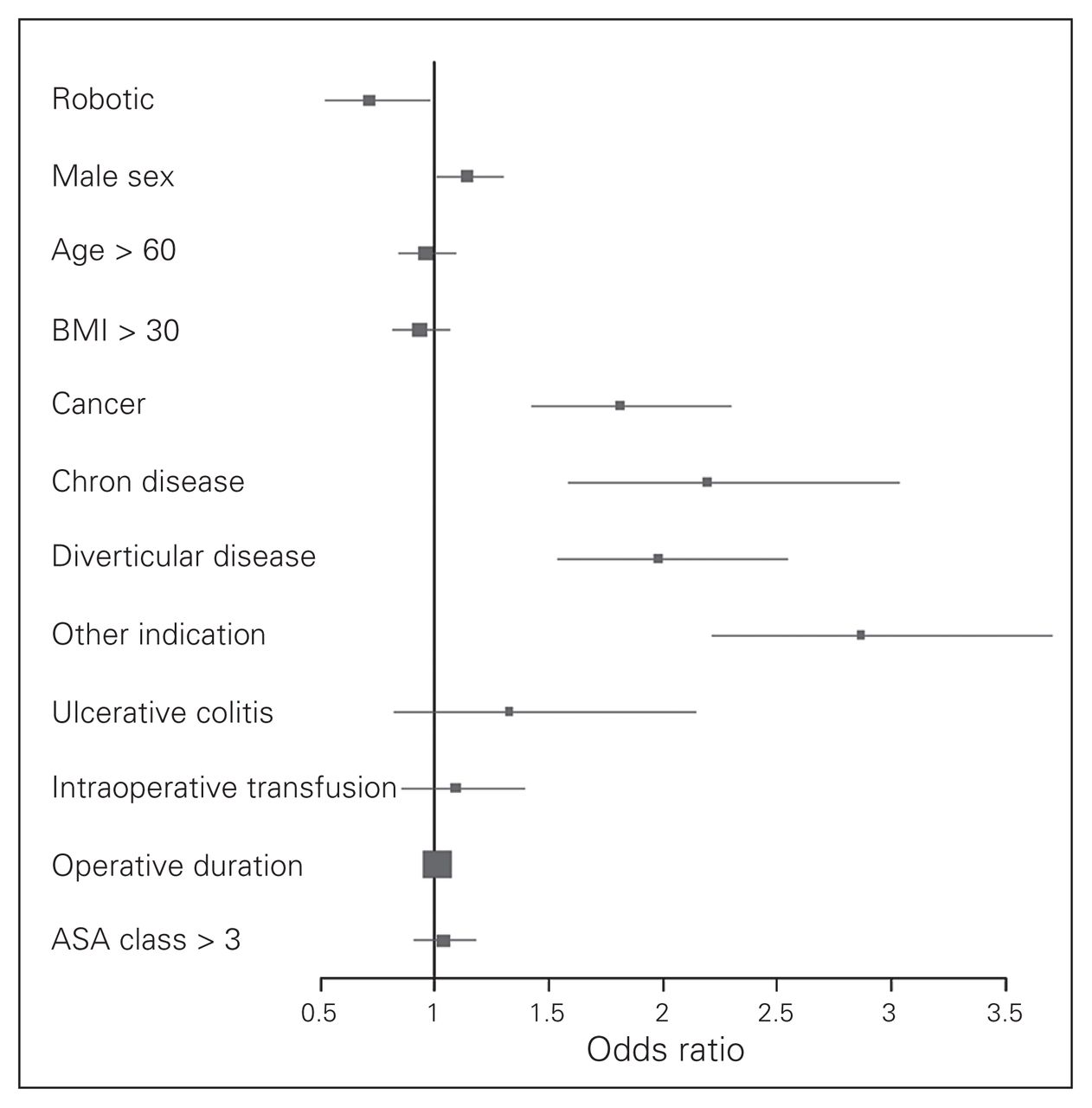
Given that unplanned conversion to an open approach was the only significant variable on univariate analysis, we developed a subsequent multivariable model to identify independent factors associated with conversion (Table 3). While male sex (odds ratio [OR] 1.143, p = 0.038), colon cancer (OR 1.810, p < 0.001), Crohn disease (2.194, p < 0.001) and diverticular disease (OR 1.980, p < 0.001) were all associated with an increased incidence of conversion on multivariable analysis, robotic surgery was found to be protective against unplanned conversion when compared with laparoscopic surgery (OR 0.713, p = 0.035). Ulcerative colitis was not significantly associated with unplanned conversion. Similarly, age older than 60 years, BMI greater than 30, American Society of Anesthesiologists (ASA) classification greater than 3, intraoperative transfusion and operative duration did not appear to increase the risk of conversion. A Forest plot illustrates the results of the multivariable model (Fig. 1).

Factors predicting unplanned intraoperative conversion. ASA = American Society of Anesthesiologists; BMI = body mass index.
Multivariable analysis for unplanned conversion in colon and rectal resection
Discussion
Whether robotic surgery offers improved clinical outcomes over laparoscopic surgery remains controversial. In the present study, we found that robotic surgery was associated with a decreased incidence of conversion. We found no significant difference in operative duration between the robotic and laparoscopic approaches. Moreover, we found no difference in any 30-day postoperative complications between the 2 modalities. In the subgroup analysis of rectal resections, robotic surgery was associated with a decreased incidence of ileus.
Our results support the finding from a recent series that demonstrated robotic surgery had a lower incidence of unplanned conversion to open procedures than laparoscopic surgery.24 Given that our study was nonrandomized, potential selection bias between patients who received robotic surgery versus laparoscopic surgery may have influenced this finding. For this reason, we performed a multivariate analysis to further inform what factors were independently associated with conversions. Upon further analysis, we found that several factors were independently associated with unplanned conversions, including male sex, malignancy and most inflammatory diseases of the colon. In patients with these risk factors, the benefit of robotic surgery may be substantial. In our subgroup analysis of rectal resections, we did not observe a significant difference in the conversion rate. Given the sample size, this finding may reflect the low event rate rather than meaningful clinical differences in the operative approach. Other published series have supported the benefit of robotic surgery in rectal resections with regards to conversion.25,26 Preliminary results of the Robotic Versus Laparoscopic Resection for Rectal Cancer (ROLARR) randomized control trial did not show a statistically significant difference in conversion rates between the 2 modalities overall.27 However, subgroup analysis supported a benefit with the robotic approach for male patients, obese patients, and those with lower tumours. It is difficult to assess whether the difference in conversion rate with robotic surgery warrants widespread adoption of this technique given the increased cost. Ramji and colleagues28 report on a Canadian series comparing robotic, laparoscopic and open rectal cancer resections. They found an incremental cost difference of approximately $6000 per case for robotic resections versus either laparoscopic or open resections. Robotic surgery may become less financially prohibitive in the future, as new platforms are expected to make costs more competitive.
In our study, we found no difference in operative durations, as has been reported in other recent publications.24,25 Earlier experiences with robotic resections reported significantly increased operative durations compared with laparoscopic surgery, representing a major limitation of the modality.29 The often reported longer duration associated with robotic surgery is likely explained by the port placement and robot docking. With increased use of robotic surgery, it is possible to overcome this learning curve and have comparable operative durations.
Bhama and colleagues30 recently published a report using the ACS-NSQIP database to compare all robotic and laparoscopic colorectal surgeries. That study compared aggregated results for a multitude of procedures, including formation of colostomy, rectopexy and other surgeries that did not involve resections. It is difficult to interpret results from this comparison of a wide variety of procedures. Our study was limited to colorectal resections without hybrid approaches in order to better characterize the effect of a robotic approach. Bhama and colleagues30 found that robotic surgery was associated with longer operating duration. Nonresectional surgery includes a variety of smaller procedures that may not warrant a robotic approach. Comparison of operative durations over a multitude of procedures is problematic, given a selection bias for one modality over another, depending on the procedure. When we compared only the resections, we did not find a significant difference in operative durations. Furthermore, Bhama and colleagues30 reported a significantly shorter length of stay in patients who underwent robotic surgery. Again, this finding is difficult to interpret given that comparison was made over a broad range of procedures. In our analysis of colon and rectal resections, we did not find any difference in length of stay between the 2 groups. Both studies report a decreased rate of conversion with robotic surgery in select patients.
Limitations
There are several important limitations to consider in our study. As a retrospective nonrandomized analysis, our study cannot eliminate potential selection bias. Patients may be preferentially selected for either robotic or laparoscopic procedures based on the anticipated degree of difficulty with the resection. As robotic surgery has been proposed to address some of the ergonomic and anatomic difficulties encountered in laparoscopic surgery, challenging cases may be preferentially performed robotically. In other situations, the choice of surgical modality may be motivated by patient preference or financial considerations. We chose to use the ACS-NSQIP database as it includes a variety of demographic variables and pre-existing patient comorbidities. This enabled us to mitigate selection bias by adjusting for clinically relevant variables with a multivariable analysis. Moreover, the variables collected by ACS-NSQIP have standardized definitions but do not provide details for the individual cases. In particular, a standard definition of the operating procedure is not available. Possible variations in the operative approach may include open components or a combination of robotic and laparoscopic surgery. We attempted to minimize this effect by excluding all patients who underwent procedures with a planned open component, but there are likely more subtle differences in operative procedure that were not captured. Furthermore, ACS-NSQIP data do not enable identification of institutional characteristics or surgeon experience, both of which may influence patient outcomes. Surgeon experience has been highly correlated with rates of conversion to open procedures.31 It is possible that the group of surgeons performing robotic surgery are proportionally more proficient in minimally invasive surgery, influencing the finding that robotic surgery is associated with a lower rate of conversion.
Conclusion
We found that robotic colorectal resection has comparable 30-day perioperative morbidity relative to laparoscopic surgery. In certain patients, robotic resection may have a lower rate of unplanned conversion to an open procedure. Given that our study focused on short-term outcomes, it is possible differences between the 2 techniques may be related to long-term outcomes, such as sexual and urinary function. There is a need for a randomized control trial to definitively compare robotic and laparoscopic modalities in terms of both short-term perioperative outcomes and long-term results.
Footnotes
Presented at the Canadian Surgery Forum, Sept. 17, 2015, Québec, Que.
Competing interests: None declared.
Contributors: A. Feinberg, M. Cleghorn and F. Quereshy designed the study. A. Feinberg and A. Elnahas acquired the data, which S. Bashir and F. Quereshy analyzed. A. Feinberg wrote the article, which all authors reviewed and approved for publication.
- Accepted April 11, 2016.
References
In this issue

{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.