


Abstract
Background: Surgical management is the basic treatment for hydatid disease. Overall, the recurrence rate appears to be high (4.6%–22.0%). The purpose of this study was to report our results in the management of recurrent hydatid disease, evaluating the methods for identifying recurrence, prognostic factors and therapeutic options.
Methods: We retrospectively reviewed the medical records of patients who underwent surgery for cystic hydatidosis between 1970 and 2003.
Results: Of the 584 patients who underwent surgery during our study period, follow-up was complete for 484 (82.8%). Cysts recurred in 51 patients (8.7%). Abdominal ultrasonography and computed tomography appeared to be efficient for diagnosing recurrence. The 2 most important determinants for recurrence were minute spillage of the hydatid cyst and inadequate treatment owing to missing cysts or incomplete pericystectomy. All but 2 recurrences required surgery. There were 14 postoperative complications for a rate of 27.0%. Thirteen re-recurrences were observed in the follow-up of these patients and also required surgery.
Conclusion: Avoidance of minute spillage of cyst contents and cautious removal of the parasite with as much of the pericyst as possible are fundamental objectives of primary hydatid surgery. Conservative surgery (removal of the cyst contents plus partial pericystectomy with drainage when necessary) plus chemotherapy and local sterilization is suggested for both primary and secondary operations and appears to achieve satisfactory long-term results. Radical surgery (resection, cystopericystectomy) is preferred only in select patients.
Despite advances in surgical techniques and the use of chemotherapy, recurrence remains one of the major problems in the management of hydatid disease.1 There is no consensus on the type of follow-up needed after primary interventions or on the management of diagnosed recurrences. Many factors have been suggested to lead to recurrence.
The purpose of this study was to present our results in the management of recurrent hydatid disease, evaluating the methods for identifying postoperative recurrence and therapeutic options. We also sought to determine prognostic factors for recurrence.
Methods
We retrospectively evaluated patients with surgically treated hydatid cysts who were followed subsequently at Aristotle University of Thessaloniki, AHEPA Hospital, 1st Propedeutic Clinic of General Surgery, Thessaloniki, Greece, between January 1970 and December 2003. Patients who underwent surgery elsewhere for hydatid disease and were referred to our clinic for recurrence were also included in the study. We extracted demographic data and information on clinical features, comorbid conditions, diagnostic methods, surgical interventions and long-term results with special emphasis on postoperative complications and recurrence from the patients’ medical records.
Recurrence is defined as the appearance of new active cysts after therapy, including reappearance with continuous growth of live cysts at the site of a previously treated cyst or the appearance of new distant disease resulting from spillage.1,2
Postoperatively, a follow-up program was carried out routinely. Our standardized protocol used the enzyme-linked immunosorbent assay (ELISA) indirect hemagglutination test for echinococcosis (IHA) and abdominal ultrasonography in the sixth postoperative month. After 6 months, annual ELISA, IHA and ultrasonography were performed. Any suspicion of recurrence based on the ultrasound was confirmed with computed tomography (CT). We considered a follow-up of at least 4 years to be complete. Time of recurrence, localization of the new cyst, complications caused by the new cyst, type of surgical intervention and complications resulting from surgical treatment were also evaluated in patients with recurrence.
Statistical analysis
All data were recorded using SPSS software, version 16 for Windows (SPSS Inc.). We tabulated data comparing groups of patients who experienced recurrences with those who remained recurrence-free according to sex, age, cyst characteristics (location, size, suppuration, calcification, multiplicity, multivesicularity, rupture) and type of surgery. Statistical comparisons were performed using the χ2 test for independence for categorical dependent variables and the independent samples t test for continuous dependent variables (patient age and cyst size). The assumptions that apply to these techniques were not violated. We considered results to be significant at p < 0.05. We analyzed postoperative recurrence rates and the disease-free time period using the Kaplan–Meier survival analysis and Cox regression analysis (the proportional hazards model).
Results
In all, 584 patients (740 cysts) underwent surgery for primary cystic hydatidosis. The male:female ratio was 212: 372, and the mean age of patients was 42 (standard deviation [SD] 1.33, range 9–68) years. Among these patients, 538 were treated for primary echinococcosis at our institute and 46 were referred with identified recurrent disease after previous surgery at other centres. Follow-up was complete for 484 (83%) patients. The median follow-up period was 58 (range 48–204) months.
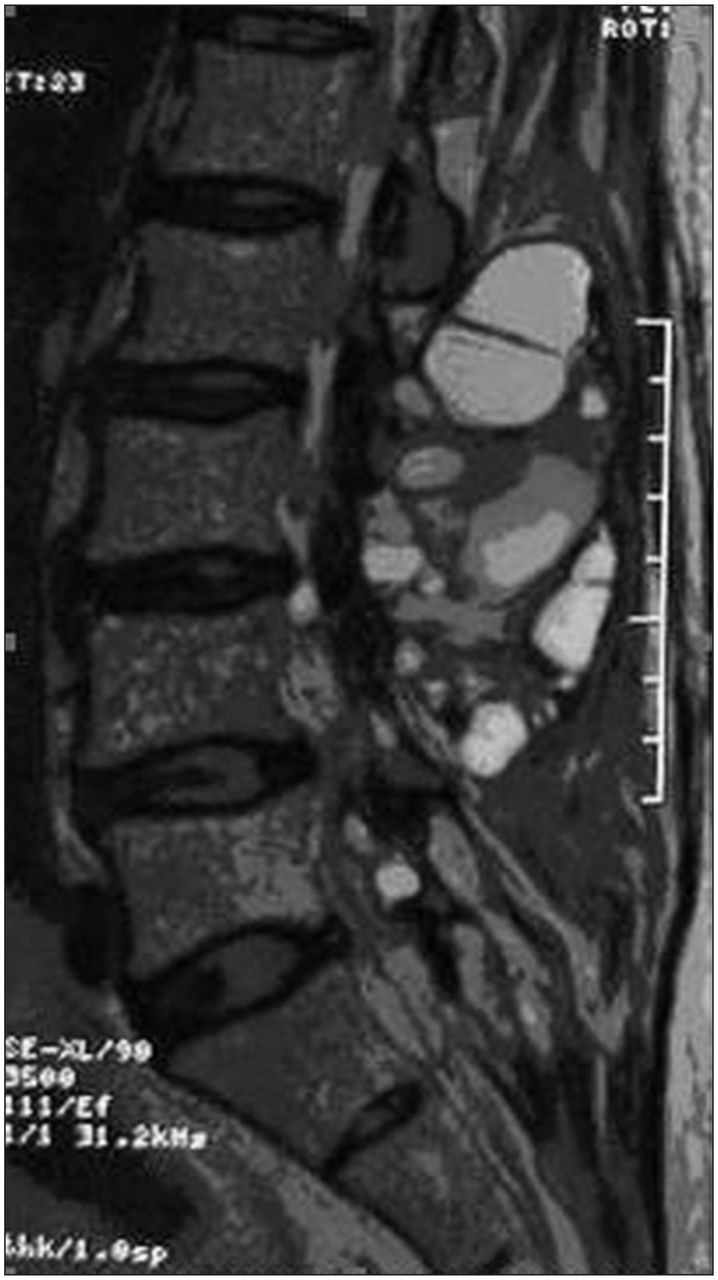
The recurrence rate was 8.7% (51 patients). In 42 patients, recurrence manifested as reappearance of live cysts at the site of a previously treated cyst, whereas in 9 patients new cysts developed at remote sites (Table 1, Figs. 1–3). Of these patients, 18 were men and 33 were women, and the mean age was 45 (range 10–68) years. The organ initially involved and the type of the primary operation performed in patients who experienced recurrences are presented in Table 2. The guidelines followed to select and perform patients’ primary operations were consistent throughout the study period. Our operative strategy was either total removal of cyst contents with pericystectomy or sterilization and obliteration of the cystic cavity, with drainage in case of intrabiliary ruptured, secondarily infected or huge calcified cysts. The characteristics of primary cysts are shown in Table 3. The period of recurrence development ranged from 6 months to 17 years. The remote time of recurrences was compatible with a differential diagnosis of frank recurrence or reinfestation.

Spinal column magnetic resonance imaging scan demonstrating paravertebral polycyclic opacities with clear boundaries (recurrent echinococcal cyst of the spine).

Removal of the parasite in patients with hydatid disease who had previously treated cysts.

Abdominal magnetic resonance imaging scan demonstrating peritoneal (perihepatic) rounded opacities (re-recurence from previously thrice-operated echinococcosis of the liver).
Postoperative recurrence in patients with previously operated hydatid cysts,* 1970–2003
Operative procedure and site of initial cysts in patients with recurrence
Characteristics of initial cysts in patients with recurrence
The onset of recurrent disease was frequently asymptomatic, and clinical evaluation was not diagnostic. Blood titres decreased slowly over months to years, even with complete removal of disease. A positive serologic test during follow-up was therefore not necessarily indicative of recurrence, but a rising titre was. However, a clinical picture appeared to be important in case of complications like rupture in the biliary or bronchial tree. One patient with a history of cysts located at the myocardium and pericardium who had presented with stroke and cysts in the arterial circulation, was readmitted with signs of arterial embolism.
The benefit of local scolicidal agents is controversial. However, we routinely performed intracystic injection of hypertonic normal saline. To avoid caustic complications, the usual concentration ranged from 6% to 10%.
The total oral dose of albendazole varied between 600 mg and 800 mg, usually for 7 days preoperatively and for 2–3 monthly cycles postoperatively. Besides the common use of anthelminthic drugs in the last 6 years of the study, these drugs had been prescribed only in selected patients with multiple cysts or difficult location of a previous “vital” cyst (since 1980). Among patients who experienced recurrences, anthelminthic drugs were used for the initial operation in 21 patients and for recurrence in 10 patients. The incidence of recurrence was equal in both groups, with and without antiparasitic prophylaxis.
Abdominal ultrasonography and CT appeared to be sensitive (59% and 78%, respectively) and reasonably specific (63% and 75%, respectively) for diagnosing recurrence, with growth of the cyst being the best imaging marker for locally recurrent disease. Despite the progressive technology, imaging was satisfactory throughout all the years of the study, leading to efficient selection of patients requiring treatment.
Regarding the factors leading to recurrence, 16 patients had presented with clinical signs of intraperitoneal spillage (history of pain and allergic reactions) before the initial surgery. Two other patients had intraoperative findings of preceding intra-abdominal contamination due to leakage of cystic contents. The development of new cysts at remote locations in 9 of these patients reflected the manifestation of disseminated disease. As mentioned in the operative report, spillage during surgical removal in the first operation occurred in 10 patients: 5 with extrahepatic intra-abdominal cysts and 5 with incomplete excision of huge multivesicular cysts with exophytic small cystic developments at inaccessible or difficult locations. In 10 of the patients, the initial cysts were localized in the posterior segment of the right hepatic lobe, resulting in incomplete pericystectomy. In 11 of the patients, there was inability to kill or evacuate all of the living cysts and protoscolexes during the first operation. These cysts were small and located at inaccessible or difficult locations.
Except for 2 patients under observation, 1 of advanced age with local recurrence and serious comorbid diseases and 1 asymptomatic patient with intrahepatic recurrence in a difficult location for surgery, all of the patients underwent repeat surgery. The operations performed for recurrent disease are shown in Table 4. In 31 patients, there were major technical difficulties that required special management (dense adhesions n = 8, hemorrhage n = 3, multiple cysts below the incision n = 19, intestinal obstruction n = 1), and in 22 of these patients they were causative mechanisms of re-recurrence.
Reoperation for recurrent cysts
There were 14 postoperative complications for a rate of 27.0%; 10 patients experienced morbidities with prolonged hospital admission owing to long-standing bile leakage or surgical site infection, whereas 4 patients experienced common respiratory or circulatory complications. The median length of stay in hospital was 18 (range 6–77) days in these patients. The patient with myocardium cysts died because of cardiorespiratory problems unrelated to the disease.
Thirteen (27%) re-recurrences (liver n = 7, lung n = 2, heart n = 1, peritoneum n = 3) were observed during the follow-up of these patients and required additional surgery. The interval of development of re-recurrences ranged from 4 months to 22 years.
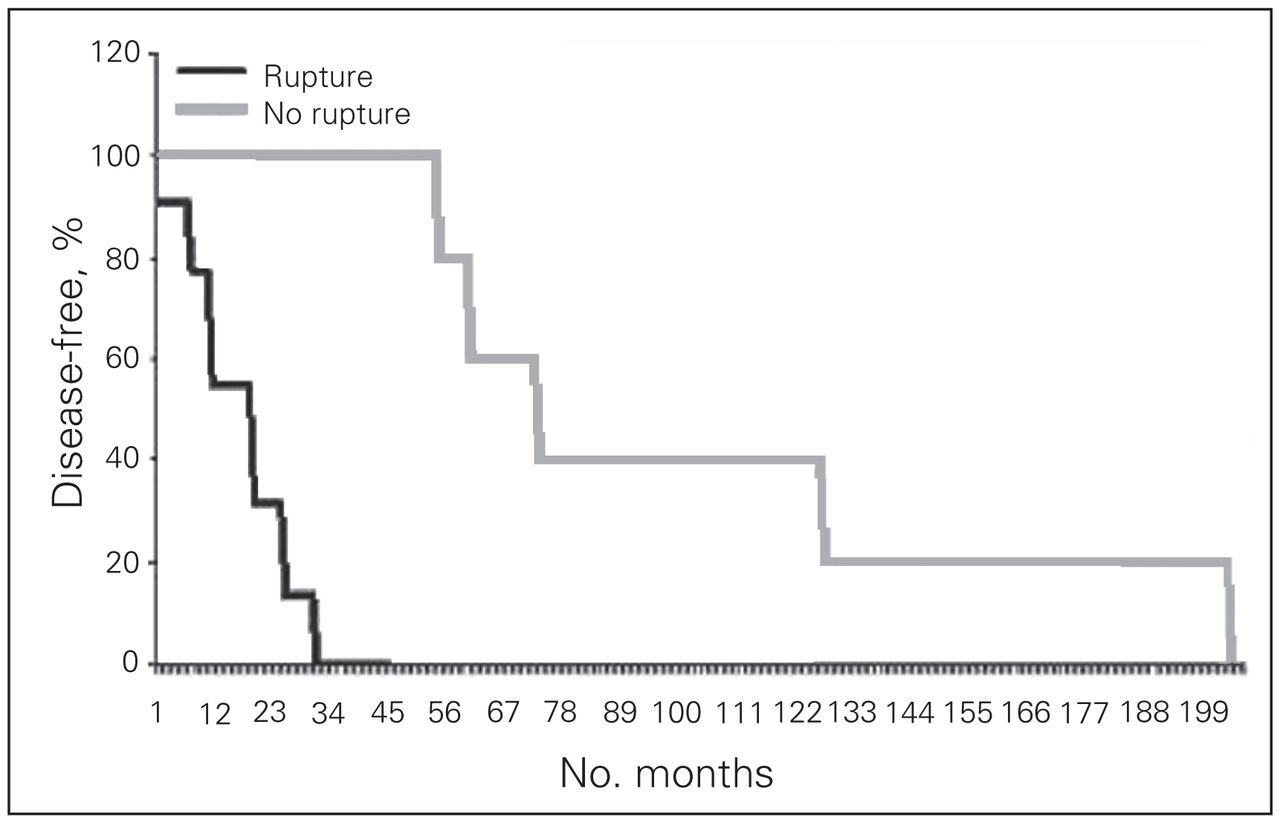
The results of our statistical comparisons are presented in Appendix 1, available at www.cma.ca/cjs. Cox regression analysis (the proportional hazards model) revealed that the most important determinants for recurrence of hydatid cysts were spillage of the hydatid cyst, missing the cysts pre- or intraoperatively and incomplete pericystectomy. The value of Exp (B) for spillage was 1.330 (95% confidence interval [CI] 0.643–2.720), indicating that the recurrence risk for a patient with microscopic rupture is 1.330 times higher than that of a patient without a ruptured hydatid cyst. Similarly, the value of Exp (B) for missing the cysts or incomplete pericystectomy was 1.194 (95% CI 0.260–5.489). We performed a Kaplan–Meier survival analysis to identify the disease-free elapsed time following successful surgery. Specifically, for patients with rupture of hydatid cysts, we found that, radiographically, 90.9% were apparently disease-free at 6 months. Freedom from recurrent disease was 77.3% at 10 months, 54.5% at 18 months, 31.8% at 24 months and 13.6% at 30 months. Finally, there was recurrence in all patients at 44 months. On the other hand, 80% of patients without known rupture of the cyst remained free of recurrent disease at 54 months, 60% at 60 months, 40% at 72 months and 20% at 126 months. Finally, there was recurrence in all patients at 204 months. These results are depicted in Figure 4. Overall comparison (Mantel–Cox log-rank test) showed that this difference was statistically significant (χ2 = 18.132, p < 0.001).

A Kaplan–Meier survival analysis shows the disease-free elapsed time after successful surgery.
Discussion
The goal of surgical management of hydatid disease is to eliminate local disease, treat associated complications and avoid recurrence while minimizing morbidity and mortality associated with the treatment itself. Various therapies include radical surgical resections, operative conservative interventions, medical therapy with antihelminthic agents and drainage after sterilization visualized by ultrasonography.1,3–6 Despite the number of therapies now available, recurrence remains one of the major problems in the management of hydatid disease, ranging from 4.6% to 22.0% in different series.1,2,7–10 In our series, the rate of recurrence was 8.7%, regardless of the type of intervention. The main reasons for recurrence appeared to be microscopic spillage of live parasites, failure to remove all viable cysts at inaccessible or difficult locations or leaving a residual cyst wall at the initial operation. The latter was especially true among patients with long-standing active cysts where there may have been penetration through the original pericyst. Recurrence detected during the early postoperative period is indicative of inadequately treated cysts in the first operation.1,7,8,11 Recurrence is actually never seen following complete resection of an intact cyst with radical surgical interventions when feasible. However, with more conservative procedures, the rate of recurrence reaches 12%.1,4,8,10–17 Our results are in line with these reports, since statistical analysis indicated that the most important determinants for recurrence of hydatid cysts were rupture and minute spillage of the hydatid cyst, missing the cysts pre- or intraoperatively and incomplete pericystectomy.
Considering these findings, radical excision may be the best treatment for hydatid disease. However, there is a trade-off between a low recurrence rate and increased mortality associated with the procedure.1,8,13,16,17 In our clinic, we do not usually perform radical excisions, which entail increased mortality, for such nonmalignant disease. We usually perform radical excisions in selected patients without any comorbid diseases, especially in patients with solitary cysts located peripherally, with good long-term results. On the other hand, when performing conservative surgery, we emphasize avoiding spillage and removing all cyst contents, including any exophytic cyst development.
The confirmation of therapeutic efficacy is difficult since recurrences may develop many years later, the onset is frequently asymptomatic and clinical evaluation, even supplemented by serum liver tests and serologic tests, may not be diagnostic.18 Thus, the postoperative follow-up period should be at least 3 years and continued as long as possible.1,7,19,20 In our series, follow-up of at least 4 years was considered to be complete. Recurrence was evident after 80 months in 16 patients. However, the absence of symptoms in many patients and the fact that many patients from remote places of residence are not referred to centres familiar with complex hepatic surgery lead to low follow-up yield (about 30% reported in large series8).
Blood titres did not return to normal values soon after the operation, therefore positive serologic tests were not significant for the diagnosis of recurrence, which had to be confirmed by ultrasonography or CT. Differentiation of remaining cavities of effectively treated cysts from locally recurrent disease was difficult, therefore we relied on the accepted imaging marker of the increase in size of the cyst on serial examination, which proved to be effective.1,21,22
We routinely used CT for patients in whom a second operation was planned to reveal the nature of the cyst, association with the biliary system, vascular structures and related organs as well as to demonstrate the extent of compensatory hyperplasia.23 The choice of operation (radical or conservative) was based on cyst location, size, morphology, complications (infection or biliary obstruction), prior treatment and presence of technical difficulties owing to adhesions. The fact that appropriate primary treatment had failed owing to “vitality” of the parasite suggested that more radical treatment might be indicated. In patients with recurrence after evacuation of cyst contents, complete cyst resection could appear to be reasonable, so long as it would be done safely. However, these radical operations are technically more difficult, and reoperations have higher morbidity and mortality rates.7 Recurrence itself appeared to increase technical difficulties due to adhesions in the secondary operations. This finding is in line with other reported mortality rates of 10%.2,4,7,8 In most recurrent cases, we preferred conservative treatment (repeat evacuation with or without partial cystectomy). Satisfactory long-term palliation was attained and was preferable to the likelihood of mortality subsequent to excessively enthusiastic attempts at a complete cure with radical excisions. Complications, such as infection or biliary obstruction, were treated first. Moreover, unlike recurrent malignant disease, recurrent hydatid disease progresses slowly and is rarely life-threatening, therefore not all patients have to be treated.1 In our series, 1 patient of advanced age with local recurrence and serious comorbid diseases and 1 asymptomatic patient with intrahepatic recurrence in a difficult location were followed expectantly and would be treated only for complications.
Conclusion
The management of patients with recurrent hydatid disease is difficult and should be carried out in centres familiar with complex hepatic surgery. Occasionally it is necessary to treat recurrent disease repeatedly. We observed 12 (27%) re-recurrences that required additional surgery. Monotherapy with antihelminthic agents or percutaneous inactivation plus chemotherapy as well as treatment by laparoscopic approach and use of intraoperative ultra-sonography seem reasonable to apply in patients with recurrent hydatid disease.9,17,19 We did not make use of the modern methods mentioned; we preferred to perform well-established, conventional operations plus chemoprophylaxis to treat this complex disease.
Footnotes
Competing interests: None declared.
Contributors: J. Prousalidis and E. Fachantidis designed the study. C. Kosmidis, K. Kapoutzis and E. Karamanlis acquired the data, which C. Kosmidis and G. Anthimidis analyzed. J. Prousalidis, C. Kosmidis, G. Anthimidis, K. Kapoutzis and E. Karamanlis wrote the article, which C. Komidis, K. Kapoutzis, E. Karamanlis and E. Fachantidis reviewed. All authors approved publication of the article.
- Accepted October 28, 2010.
References

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.