
Abstract
Background
Preoperative magnetic resonance imaging (MRI) utilization in breast cancer treatment has increased significantly over the past 2 decades, but its use continues to have interprovider variability and disputed clinical indications.
Objective
The aim of this study was to evaluate non-clinical factors associated with preoperative breast MRI utilization.
Methods
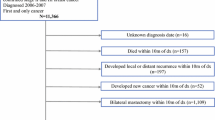
This study utilized TRICARE claims data from 2006 to 2015. TRICARE provides health benefits for active duty service members, retirees, and their dependents at both military (direct care with salaried physicians) and civilian (purchased care under fee-for-service structure) facilities. We studied patients aged 25–64 years with a breast cancer diagnosis who had undergone mammogram/ultrasound (MMG/US) alone or with subsequent breast MRI prior to surgery. Facility characteristics included urban–rural location according to the National Center for Health Statistics classification. Adjusted multivariable logistic regression tests were used to identify independent factors associated with preoperative breast MRI utilization.
Results
Of the 25,392 identified patients, 64.7% (n = 16,428) received preoperative MMG/US alone, while 35.3% (n = 8964) underwent additional MRI. Younger age, Charlson Comorbidity Index score ≥ 2, active duty or retired beneficiary category, officer rank (surrogate for socioeconomic status), Air Force service branch, metropolitan location, and purchased care were associated with an increased likelihood of preoperative MRI utilization. Non-metropolitan location and Navy service branch were associated with decreased MRI use.
Conclusion
After controlling for expected clinical risk factors, patients were more likely to receive additional MRI when treated at metropolitan facilities or through the fee-for-service system. Both associations may point toward non-clinical incentives to perform MRI in the treatment of breast cancer.

Similar content being viewed by others


References
Esserman L, Hylton N, Yassa L, Barclay J, Frankel S, Sickles E. Utility of magnetic resonance imaging in the management of breast cancer: evidence for improved preoperative staging. J Clin Oncol. 1999;17(1):110–119.
Berg WA, Gutierrez L, NessAiver MS, et al. Diagnostic accuracy of mammography, clinical examination, US, and MR imaging in preoperative assessment of breast cancer. Radiology. 2004;233(3):830–849.
Sardanelli F, Giuseppetti GM, Panizza P, et al. Sensitivity of MRI versus mammography for detecting foci of multifocal, multicentric breast cancer in Fatty and dense breasts using the whole-breast pathologic examination as a gold standard. AJR Am J Roentgenol. 2004;183(4):1149–1157.
Bleicher RJ, Ciocca RM, Egleston BL, et al. Association of routine pretreatment magnetic resonance imaging with time to surgery, mastectomy rate, and margin status. J Am Coll Surg. 2009;209(2):180–187; quiz 294-185.
Lobbes MB, Vriens IJ, van Bommel AC, et al. Breast MRI increases the number of mastectomies for ductal cancers, but decreases them for lobular cancers. Breast Cancer Res Treat. 2017;162(2):353–364.
Turnbull L, Brown S, Harvey I, et al. Comparative effectiveness of MRI in breast cancer (COMICE) trial: a randomised controlled trial. Lancet. 2010;375(9714):563–571.
Peters NH, van Esser S, van den Bosch MA, et al. Preoperative MRI and surgical management in patients with nonpalpable breast cancer: the MONET—randomised controlled trial. Eur J Cancer (Oxford, England: 1990). 2011;47(6):879–886.
Shin HC, Han W, Moon HG, et al. Limited value and utility of breast MRI in patients undergoing breast-conserving cancer surgery. Ann Surg Oncol. 2012;19(8):2572–2579.
Houssami N, Turner R, Macaskill P, et al. An individual person data meta-analysis of preoperative magnetic resonance imaging and breast cancer recurrence. J Clin Oncol. 2014;32(5):392–401.
Choi WJ, Cha JH, Kim HH, et al. Long-term survival outcomes of primary breast cancer in women with or without preoperative magnetic resonance imaging: a matched cohort study. Clin Oncol (Royal College of Radiologists (Great Britain)). 2017; 29:653–661
Katipamula R, Degnim AC, Hoskin T, et al. Trends in mastectomy rates at the Mayo Clinic Rochester: effect of surgical year and preoperative magnetic resonance imaging. J Clin Oncol. 2009;27(25):4082–4088.
Wang SY, Virnig BA, Tuttle TM, Jacobs DR, Jr., Kuntz KM, Kane RL. Variability of preoperative breast MRI utilization among older women with newly diagnosed early-stage breast cancer. Breast J. 2013;19(6):627–636.
Solin LJ, Orel SG, Hwang WT, Harris EE, Schnall MD. Relationship of breast magnetic resonance imaging to outcome after breast-conservation treatment with radiation for women with early-stage invasive breast carcinoma or ductal carcinoma in situ. J Clin Oncol. 2008;26(3):386–391.
Miller BT, Abbott AM, Tuttle TM. The influence of preoperative MRI on breast cancer treatment. Ann Surg Oncol. 2012;19(2):536–540.
Ko ES, Han BK, Kim RB, et al. Analysis of the effect of breast magnetic resonance imaging on the outcome in women undergoing breast conservation surgery with radiation therapy. J Surg Oncol. 2013;107(8):815–821.
Nguyen LL, Smith AD, Scully RE, et al. Provider-induced demand in the treatment of carotid artery stenosis: variation in treatment decisions between private sector fee-for-service versus salary-based military physicians. JAMA Surg. 2017;152(6):565–572.
Stewart KA, Higgins PC, McLaughlin CG, Williams TV, Granger E, Croghan TW. Differences in prevalence, treatment, and outcomes of asthma among a diverse population of children with equal access to care: findings from a study in the military health system. Arch Pediatr Adolesc Med. 2010;164(8):720–726.
Military Health System Review: Final Report. http://www.defense.gov/Portals/1/Documents/pubs/140930_MHS_Review_Final_Report_Main_Body.pdf. Accessed 9 June 2016.
Bagchi AD, Schone E, Higgins P, Granger E, Casscells SW, Croghan T. Racial and ethnic health disparities in TRICARE. J Natl Med Assoc. 2009;101(7):663–670.
Ambrosio A, Brigger MT. Surgery for otitis media in a universal health care model: socioeconomic status and race/ethnicity effects. Otolaryngol Head Neck Surg. 2014;151(1):137–141.
Schoenfeld AJ, Jiang W, Harris MB, et al. Association between race and postoperative outcomes in a universally insured population versus patients in the State of California. Ann Surg. 2017;266(2):267–273.
Pak LM, Fogel HA, Chaudhary MA, et al. Outpatient spine clinic utilization is associated with reduced emergency department visits following spine surgery. Spine (Phila Pa 1976). 2017;43(14):E836–E841.
NCHS Urban-Rural Classification Scheme for Counties. 2013. https://www.cdc.gov/nchs/data/series/sr_02/sr02_166.pdf. Accessed July 2018.
Whitehead J, Carlile T, Kopecky KJ, et al. Wolfe mammographic parenchymal patterns. A study of the masking hypothesis of Egan and Mosteller. Cancer. 1985;56(6):1280–1286.
van Gils CH, Otten JD, Verbeek AL, Hendriks JH. Mammographic breast density and risk of breast cancer: masking bias or causality? Eur J Epidemiol. 1998;14(4):315–320.
Lehman CD, Gatsonis C, Kuhl CK, et al. MRI evaluation of the contralateral breast in women with recently diagnosed breast cancer. N Engl J Med. 2007;356(13):1295–1303.
Dwyer M, Rehman S, Ottavi T, et al. Urban-rural differences in the care and outcomes of acute stroke patients: systematic review. J Neurol Sci. 2019;397:63–74.
Benchimol EI, Kuenzig ME, Bernstein CN, et al. Rural and urban disparities in the care of Canadian patients with inflammatory bowel disease: a population-based study. Clin Epidemiol. 2018;10:1613–1626.
Chen X, Orom H, Hay JL, et al. Differences in rural and urban health information access and use. J Rural Health. 2019;35(3):405–417.
Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155(2):97–107.
Onega T, Lee CI, Benkeser D, et al. Travel burden to breast MRI and utilization: are risk and sociodemographics related? J Am Coll Radiol. 2016;13(6):611–619.
Parker A, Schroen AT, Brenin DR. MRI utilization in newly diagnosed breast cancer: a survey of practicing surgeons. Ann Surg Oncol. 2013;20(8):2600–2606.
Helmchen LA, Lo Sasso AT. How sensitive is physician performance to alternative compensation schedules? Evidence from a large network of primary care clinics. Health Econ. 2010;19(11):1300–1317.
Hendrick RE, Cutter GR, Berns EA, et al. Community-based mammography practice: services, charges, and interpretation methods. AJR Am J Roentgenol. 2005;184(2):433–438.
Stout NK, Nekhlyudov L. Early uptake of breast magnetic resonance imaging in a community-based medical practice, 2000–2004. J Womens Health. 2011;20(4):631–634.
Bassett LW, Dhaliwal SG, Eradat J, et al. National trends and practices in breast MRI. AJR Am J Roentgenol. 2008;191(2):332–339.
Saslow D, Boetes C, Burke W, et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clins. 2007;57(2):75–89.
U.S. Preventive Services Task Force. Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2009;151(10):716–726, w-236.
Position Statement on the Use of Magnetic Resonance Imaging in Breast Surgical Oncology. 2010. https://breast360.org/wp-content/uploads/filer_public/cf/b9/cfb91322-7fb0-4bfa-a673-7a5efcbd375f/mri.pdf. Accessed Mar 2019.
Mann RM, Hoogeveen YL, Blickman JG, Boetes C. MRI compared to conventional diagnostic work-up in the detection and evaluation of invasive lobular carcinoma of the breast: a review of existing literature. Breast Cancer Res Treat. 2008;107(1):1–14.
Balmana J, Diez O, Castiglione M. BRCA in breast cancer: ESMO clinical recommendations. Ann Oncol. 2009;20 Suppl 4:19–20.
Acknowledgments
None.
Funding
The Center for Surgery and Public Health is jointly supported in part with the Uniformed Services University of the Health Sciences by a grant from the Department of Defense Defense Health Agency.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Linda M. Pak, Amanda Banaag, Tracey P. Koehlmoos, Louis L. Nguyen, and Peter A. Learn have no conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Disclaimer: The views expressed in this work are those of the authors and do not reflect the official policy or position of the Uniformed Services University of the Health Sciences, the Department of Defense, or the US government.
Rights and permissions
About this article

Cite this article
Pak, L.M., Banaag, A., Koehlmoos, T.P. et al. Non-clinical Drivers of Variation in Preoperative MRI Utilization for Breast Cancer. Ann Surg Oncol 27, 3414–3423 (2020). https://doi.org/10.1245/s10434-020-08380-2
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-020-08380-2