
Abstract
We investigated the relation between age and respiratory control during exercise in 80 children aged 6.4-17.6 y (42 male, age, 11.6 ± 3.3 y; body weight, 41.3 ± 14.7 kg; and 38 female, age, 12.6 ± 2.7 y; body weight, 42.5 ± 9.3 kg). Exercise tests were performed on a treadmill after a standard symptom-limited Bruce protocol. Data were analyzed separately for boys and girls. At rest and at peak exercise, the ratio of minute ventilation to carbon dioxide production(˙VE/˙VCO2), the ratio of effective alveolar ventilation to carbon dioxide production(˙VA/˙VCO2), the ratio of pulmonary dead space to tidal volume (Vd/V t), and arterial PCO2 (PaCO2) were not correlated with age. At the exercise intensity of ventilatory anaerobic threshold, the PaCO2 increased, and the ˙VA/˙VCO2 decreased, significantly with age, whereas the Vd/V t was not related to age. Linear regression analysis demonstrated that the slope of the relationship between ˙VE and ˙VCO2(Δ˙VE/Δ˙VCO2) and the slope of the relationship between ˙VA and ˙VCO2(Δ˙VA/Δ˙VCO2) decreased with age. There were no gender differences in the regression slopes and the intercepts of the relationships. Results show that younger children breathe more during exercise to eliminate a given amount of CO2 to keep PaCO2 set point slightly but significantly lower than older children. This age dependence must be considered in investigating ventilatory control during exercise in children.
Similar content being viewed by others


Main
Previous studies have identified age-related changes in the ventilatory response to exercise(1–3). Brischetto et al.(1) have reported that ventilation is increased in response to exercise and decreased in response to hypercapnea in elderly subjects compared with young subjects. The PaCO2 at rest is regulated at a lower level in infants than in adults(4). Thus the ventilatory response to exercise in children may be influenced by age.
Springer et al.(2) reported that the contribution of peripheral chemoreceptor to respiratory control during exercise is greater in normal young children than in adults. Cooper et al.(3) reported that the slope of the relationship between minute ventilation (˙VE) and carbon dioxide production(˙VCO2) during incremental exercise(Δ˙VE/Δ˙VCO2) was greater and the end-tidal PCO2 (PETCO2) during exercise was significantly lower in younger children than in teenagers(3), indicating that the PaCO2 was regulated at a lower level in younger children. Their study was the first to address the developmental process in relation to respiratory control during exercise. However, they assessed respiratory control during exercise using theΔ˙VE/Δ˙VCO2, which is affected by physiologic pulmonary dead space, as well as by the PaCO2 set point(5). Because the influence of dead space should be eliminated when assessing respiratory control, the effective alveolar ventilation (˙VA) is a more accurate index(6). Cooper et al.(3) also did not separately evaluate ventilatory response in boys and girls. We aimed to investigate the relation between age and respiratory control using ˙V A in boys and girls.
METHODS
Subjects. We studied 80 Japanese children and adolescents (aged 6.4-17.6 y) who volunteered to participate in the study, including 42 boys(age, 11.6 ± 3.3 y; body weight, 41.3 ± 14.7 kg; body surface area, 1.29 ± 0.3 m2) and 38 girls (age, 12.6 ± 2.7 y; body weight, 42.5 ± 9.3 kg; body surface area, 1.37 ± 0.2 m2). The differences in age and body weight and body surface area between the sexes were not significant. No cardiopulmonary or other diseases were detected by physical examinations or medical questionnaire. Children with a body mass index greater than 25 were excluded. No attempt was made to select subjects who were particularly active. Written informed consent was obtained from each participant and his/her parent(s).
Exercise tests. Exercise tests were performed on a treadmill(MAT-2500, Fukuda Denshi Co. Ltd., Tokyo, Japan) with a standard symptom-limited Bruce protocol. An ECG and the heart rate were monitored throughout the test with the stress test system (ML-5000, Fukuda Denshi Co. Ltd., Tokyo, Japan). The cuff blood pressure was also measured every minute with an automatic indirect manometer (STBP-680F, Collin Denshi, Nagoya, Japan).
Analysis of expired gas. Subjects breathed through a low impedance turbine volume transducer for measurement of expiratory volume. The external dead space of the mouthpiece and turbine device(Vdext = 90 mL) was subtracted from the tidal volume(Vt). The calculated ˙VE was as follows:Equation where RR = breaths/min.

Carbon dioxide production [˙VCO2 (mL/min, STPD)], oxygen uptake [˙VO2 (mL/min, STPD)], minute ventilation[˙VE (L/min, BTPS)], tidal volume (mL), the RR, and the mixed expiratory carbon dioxide concentration (%) were continuously measured on a breath-by-breath basis with the OXYCON Sigma device (AE-3981) and a metabolic measurement cart (Mijnhardt Bunnik, the Netherlands) equipped with an oxygen and carbon dioxide analyzer. Respiratory flow was measured by the turbine volume sensor. To reduce breath-by-breath “noise,” data were processed with a five breath-moving average filter.
˙VA was derived from the followingequation(6): where Vd/Vt is the ratio of the pulmonary dead space to the tidal volume derived from the following modified alveolar gasequation(7),


The PaCO2 was estimated noninvasively by the followingequation derived from regression analysis of the relationships among PaCO2, PETCO2, and Vt during exercise(8), The validity of this equation has been confirmed in the normal adult population(8, 9).

Ventilatory control during exercise was assessed by the slope of the relationship between ˙VE and ˙VCO2(Δ˙VE/Δ˙VCO2) and by the slope of the relationship between ˙VA and ˙VCO2 during incremental exercise(Δ˙VA/Δ˙VCO2). The slopes were determined by linear regression analysis of the relationship between ˙V E and ˙VCO2 or between ˙VA and ˙VCO2 during exercise using data obtained before the occurrence of respiratory compensation(10–12).
The ventilatory anaerobic threshold (VAT) was defined as the level of ˙VO2 at which at least one of the following occurred(13, 14): 1) an increase in the ˙VE/˙VO2 without a simultaneous increase in ˙VE/˙VCO2, 2) an increase in end-tidal oxygen partial pressure without a simultaneous decrease in PETCO2, and 3) the disappearance of the linear relationship between ˙VCO2 and ˙VO2(the V slope method).
The estimated PaCO2 and Vd/Vt at rest were determined by averaging the data obtained for 2 min while the subjects were sitting quietly. The PaCO2 and Vd/Vt during exercise were determined from data obtained during 30 s at the VAT and during the final 30 s of peak exercise. We used the average of the 30 s data for analysis.
Statistical analysis. The relationships between parameters(˙VE/˙VCO2,˙V A/˙VCO2, Vd/Vt, and PaCO2) and age and body weight, were determined by simple linear regression analysis. Coincidence of regression slopes and regression intercepts were tested using the table of t distribution. A level of p < 0.05 was accepted as statistically significant.
RESULTS
At rest, the ˙VE/˙VCO2,˙V A/˙VCO2, Vd/Vt, and PaCO2 were not correlated with age in either boys or girls(Table 1). At peak exercise, these parameters were also not correlated with age in both boys and girls except for the Vd/Vt in boys (Table 1).
At the VAT, PaCO2 was positively (Fig. 1 and Table 1), and the ˙V A/˙VCO2 was negatively correlated with age in both sexes (Table 1), whereas the Vd/Vt was not related to age (Fig. 1 and Table 1). The ˙V E/˙VCO2 was inversely correlated with age in girls, but not in boys (Table 1).

Changes in PaCO2 and the Vd/Vt at the exercise level of the VAT in relation to age. Closed circles, solid line, boys; open circles, dotted line, girls. est, estimated.
Linear regression analysis demonstrated that theΔ˙VE/Δ˙VCO2 and theΔ˙VA/Δ˙VCO2 decreased with age in boys and girls (Fig. 2 and Table 1). However, there were no gender differences in the regression slopes and the intercepts of these relationships (Figs. 1 and 2 and Table 1).

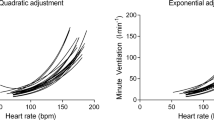
Age-related decrease in the slope of the relation between ˙VE and ˙VCO2, and between ˙V A and ˙VCO2. Closed circles, solid line, boys; open circles, dotted line, girls. BTPS, body temperature, ambient pressure, and saturated with water vapor.
The Vd/Vt at rest were 0.29 ± 0.06 in boys and 0.26 ± 0.10 in girls; the Vd/Vt at the V AT were 0.13 ± 0.04 in boys and 0.14 ± 0.07 in girls; and the Vd/Vt at peak exercise were 0.13 ± 0.07 in boys and 0.11 ± 0.04 in girls.
DISCUSSION
The ˙VA required to eliminate a given amount of CO2 during exercise was greater in younger children than in older children. This difference was accounted for by the slightly but significantly lower PaCO2 set-point during exercise in younger children, although no differences were observed at rest. The Vd/Vt, another factor that may influence ventilation, was not a function of age or body weight. These results essentially confirm the results of the study by Cooper et al.(3).
These age-related differences may be explained by the higher metabolic rate in younger children. However, if this is the sole mechanism of their increased ventilation, their PaCO2 set point andΔ˙VA/Δ˙VCO2 must not be influenced, because the increased metabolic rate, the increased ˙V CO2, will result in proportional change in ˙V A and the same values ofΔ˙VA/Δ˙VCO2. Rather, our results suggest that the age dependence of respiratory control during exercise is due to the maturational changes in the sensitivity of the central and peripheral chemoreceptor. Springer et al.(2) reported that the contribution of peripheral chemoreceptor to respiratory control during exercise is greater in normal young children than in adults. Their results support the hypothesis that there is a maturational change in the control of ventilation.
The Δ˙VE/Δ˙VCO2 is widely used to estimate the ventilatory drive(3, 11, 12, 15, 16). However, as the modified alveolar gas equation shows, ˙VE is regulated by the Vd/Vt as well as by the PaCO2 set point. Therefore, this index is affected by the pulmonary dead space (anatomical dead space and physiologic dead space) and thus is not a valid index of neurohumoral ventilatory control. We used theΔ˙VA/Δ˙VCO2, which is not affected by pulmonary dead space, as an index of neurohumoral respiratory control during exercise. In this study, the Vd/Vt was not influenced by age or body weight during exercise, but the correlation coefficient between PaCO2 and ˙V A/˙VCO2 was higher than that between PaCO2 and ˙VE/˙VCO2 at rest(r = 0.912, versus r = 0.416), at the VAT(r = 0.881, versus r = 0.513) and at peak exercise(r = 0.989, versus r = 0.879). That is why we advocate the use of alveolar ventilation instead of minute ventilation to improve accuracy by taking into account the effect of pulmonary dead space.
Invasive measurement of PaCO2 is ethically problematic, especially for normal children. Therefore Cooper et al.(2) used PETCO2 to estimate the PaCO2(2). However, PETCO2 does not take into account the difference between end-tidal and arterial PCO2 values during exercise, which is known to increase with ˙VCO2(8). Therefore, we noninvasively estimated the PaCO2 using the method of Jones et al.(8), which was derived from data obtained from healthy men aged 24-34 y. The validity of this method was confirmed in a subsequent study in normal subjects aged 18-25 y(9). In this equation, tidal volume was dependent on anatomical measurements and may be different in children.
Parameters of ventilatory control at peak exercise were not correlated with age in boys or girls in the present study. This finding may be related to the development of hypocapnic hyperventilation or to the respiratory compensation at the end stage of exercise testing.
In summary, the Δ˙VE/Δ˙VCO2 and the Δ˙VA/Δ˙VCO2 during exercise were greater in younger children than in older children, whereas the Vd/Vt was not influenced by age or body weight. These age-related differences were explained by the slightly but significantly lower PaCO2 set point during exercise in younger children, although no differences were observed at rest.
Abbreviations
- ˙V,E:
-
minute ventilation
- ˙VA:
-
effective alveolar ventilation
- V t :
-
tidal volume
- V d :
-
pulmonary dead space
- Vd/V t:
-
ratio of pulmonary dead space to tidal volume
- ˙VCO2:
-
carbon dioxide production
- PaCO2:
-
arterial PCO2
- PETCO2:
-
end-tidal PCO2
- Δ˙VE/Δ˙VCO2:
-
slope of the relationship between ˙Ve and ˙V CO2
- Δ˙VA/Δ˙VCO2:
-
slope of the relationship between ˙VA and ˙V CO2
- VAT:
-
ventilatory anaerobic threshold
- RR:
-
respiratory rate
- STPD:
-
standard pressure (and) pressure, dry
References
Brischetto MJ, Millman RP, Peterson DD, Silage DA, Pack AI 1984 Effect of aging on ventilatory response to exercise and CO2 . J Appl Physiol 56: 1143–1150.
Springer C, Cooper DM, Wasserman K 1988 Evidence that maturation of the peripheral chemoreceptors is not complete in childhood. Respir Physiol 74: 55–64.
Cooper DM, Kaplan MR, Baumgarten L, Weiler-Ravell D, Whipp BJ, Wasserman K 1987 Coupling of ventilation and CO2 production during exercise in children. Pediatr Res 21: 568–572.
Rigatto H, Brady JP, Verduzco R 1975 Chemoreceptor reflexes in preterm infants. 1. The effect of gestational and postnatal age on the ventilatory response to inhalation of 100% and 15% oxygen. Pediatrics 55: 604–613.
Clark AL, Chua TP, Coats AJS 1995 Anatomical dead space, ventilatory pattern, and exercise capacity in chronic heart failure. Br Heart J 74: 377–380.
Sullivan MJ, Higginbotham MB, Cobb FR 1988 Increased exercise ventilation in patients with chronic heart failure: intact ventilatory control despite hemodynamic and pulmonary abnormalities. Circulation 77: 552–559.
Caiozzo VJ, Davis JA, Berriman DJ, Vandagriff RB, Prietto CA 1987 Effect of high-intensity exercise on the V E-VCO2 relationship. J Appl Physiol 62: 1460–1464.
Jones NL, Robertson DG, Kane JW 1979 Difference between end-tidal and arterial PCO2 in exercise. J Appl Physiol 47: 954–960.
Robbins PA, Conway J, Cunningham DA, Khamnei S, Paterson DJ 1990 A comparison of indirect methods for continuous estimation of arterial PCO2 in men. J Appl Physiol 68: 1727–1731.
Buller NP, Poole-Wilson PA 1990 Mechanism of the increased ventilatory response to exercise in patients with chronic heart failure. Br Heart J 63: 281–283.
Merta M, Cas LDC, Pania G, Visioli O 1992 Exercise hyperventilation chronic congestive heart failure, and its relation to functional capacity and hemodynamics. Am J Cardiol 70: 622–628.
Tantucci C, Bottini M, Dottorini ML, Puxeddu E, Caucci G, Scionti L, Sorbini CA 1996 Ventilatory response to exercise in diabetic subjects with autonomic neuropathy. J Appl Physiol 81: 1978–1986.
Wasserman K, Hansen JE, Sue DY, Whipp BJ, Casaburi R 1994 Principles of Exercise Testing and Interpretation, 2nd Ed. Lea & Febiger, Philadelphia, PP 62–64.
Beaver WL, Wasserman K 1991 Muscle RQ and lactate accumulation from analysis of the VCO2-VO2 relationship during exercise. Clin J Sport Med 1: 27–34.
Banning AP, Lewis NP, Elborn JS, Hall RJ 1995 Exercise ventilation after balloon dilation of the mitral valve. Br Heart J 73: 386–389.
Wada O, Asano H, Miyagi K, Ishizaka S, Kameyama T, Seto H, Sasayama S 1993 Importances of abnormal lung perfusion in excessive exercise ventilation in chronic heart failure. Am Heart J 125: 790–798.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Nagano, Y., Baba, R., Kuraishi, K. et al. Ventilatory Control during Exercise in Normal Children. Pediatr Res 43, 704–707 (1998). https://doi.org/10.1203/00006450-199805000-00021
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199805000-00021
This article is cited by
-
A Systematic Review of Reference Values in Pediatric Cardiopulmonary Exercise Testing
Pediatric Cardiology (2015)
-
Exercise Capacity in Pediatric Heart Transplant Candidates: Is There Any Role for the 14 ml/kg/min Guideline?
Pediatric Cardiology (2006)
-
Exercise-induced breathing patterns of youth are related to age and intensity
European Journal of Applied Physiology (2006)
-
High-intensity intermittent running training improves pulmonary function and alters exercise breathing pattern in children
European Journal of Applied Physiology (2005)
