
Abstract
Tocolysis with nonsteroidal anti-inflammatory drugs (NSAIDs) has been widely accepted for several years. Recently, the use of the cyclooxygenase-2 (COX2) preferential NSAID nimesulide has been proposed. However, data reporting neonatal acute renal failure or irreversible end-stage renal failure after maternal ingestion of nimesulide question the safety of this drug for the fetus and the neonate. Therefore, this study was designed to define the renal effects of nimesulide in newborn rabbits. Experiments were performed in 28 newborn rabbits. Renal function and hemodynamic parameters were measured using inulin and para-aminohippuric acid clearances as markers of GFR and renal blood flow, respectively. After a control period, nimesulide 2, 20, or 200 μg/kg was given as an i.v. bolus, followed by a 0.05, 0.5, or 5 μg · kg−1 · min−1 infusion. Nimesulide administration induced a significant dose-dependent increase in renal vascular resistance (29, 37, and 92%, respectively), with a concomitant decrease in diuresis (−5, −23, and −44%), GFR (−12, −23, and −47%), and renal blood flow (−23, −23, and −48%). These results are in contrast with recent reports claiming that selective COX2 inhibition could be safer for the kidney than nonselective NSAIDs. These experiments confirm that prostaglandins, by maintaining renal vasodilation, play a key role in the delicate balance regulating neonatal GFR. We conclude that COX2-selective/preferential inhibitors thus should be prescribed with the same caution as nonselective NSAIDs during pregnancy and in the neonatal period.
Similar content being viewed by others

Main
Because of the role of prostaglandins (PGs) in the genesis of labor (term or preterm), nonselective nonsteroidal anti-inflammatory drugs (NSAIDs) have been used as tocolytic drugs for several decades. Meanwhile, the use of NSAIDs during pregnancy to treat toxemia, polyhydramnios, or preterm labor and in the immediate postnatal period to induce closure of a symptomatic patent ductus arteriosus is increasing (1–4). However, side effects that affect mainly the cerebral, mesenteric, and renal microcirculations have been reported in fetuses and neonates (5–10), and NSAID-associated pulmonary hypoperfusion and persistence of fetal circulation may also compromise the newborn renal function (4, 11).
It has been claimed that selective cyclooxygenase-2 (COX2) inhibitors could have the same curative effects as nonselective NSAIDs without the deleterious side effects attributed to COX1 inhibition. Therefore, the use of the COX2-preferential NSAID nimesulide (12, 13) has been proposed for tocolysis in humans (14). In a case report, Sawdy et al.(14) found no effect of nimesulide administered from the 16th to the 34th week of gestation on the renal and ductal functions of the fetus. Doppler flow indices for the ductus arteriosus and amniotic fluid index remained normal, and the infant was born with no congenital abnormalities and an uncomplicated neonatal course (14). However, recent data reporting severe oligohydramnios (15), reversible oliguric, or even irreversible end-stage neonatal renal failure (16–18) after maternal ingestion of nimesulide question the safety of COX2-selective NSAIDs for the fetus and the neonate.
We previously demonstrated that the nonselective NSAIDs aspirin, indomethacin, and the more recently introduced ibuprofen have similar renal side effects in the neonatal period, including significant reductions of diuresis, GFR, and renal blood flow (RBF), associated with a rise in renal vascular resistance (RVR) (19–22). The present study thus was designed to assess the renal hemodynamic effects of the preferential COX2 inhibitor nimesulide in the newborn rabbit, an animal model that shows great similarities to the developing kidney of the human premature infant (23).
METHODS
Animal experiments.
The animal studies were performed according to the guidelines of the Swiss National Research Foundation. Twenty-eight normoxemic, 5.6 ± 0.2-day-old (mean ± SEM) New Zealand White rabbits that weighed 105.6 ± 3.0 g were studied. All animals were born in our own animal facilities by spontaneous vaginal delivery and breast-fed until the time of study. Animals were issued from 11 different litters studied over a period of 12 mo. Therefore, to avoid possible inaccuracies as a result of the interanimal and interlitter variability of the data, the experimental absolute data were compared only within the same group of animals over time.
All methods have been described previously (20). Briefly, the rabbits were anesthetized with 25 mg/kg body weight of sodium pentobarbital i.p. and artificially ventilated via tracheostomy with an oxygen-enriched gas mixture. The respiratory rate was kept constant at 40 breaths/min, and tidal volume was adjusted for age and weight. Internal body temperature was maintained in the range of physiologic values for rabbits (39°C). The femoral vessels had catheters implanted for solute infusion, arterial blood sampling, and continuous monitoring of mean arterial blood pressure (MAP) and heart rate (HR). Urine was sampled by bladder catheterization.
After completion of the surgical procedure (approximately 1 h), inulin and para-aminohippuric acid (PAH) clearances were measured throughout the experiment. From this point onward, all animals received a constant infusion of a modified rabbit Ringer solution at a rate of 1 mL · h−1 · 100 g−1 birth weight (20).
Experimental protocol.
A 90-min equilibration period was allowed, followed by a 60-min control period consisting of two 30-min urine collections with 0.4 mL of blood withdrawn at the midpoint of each collection. Eighty microliters were used for immediate measurements of blood gases, hematocrit, and plasma protein levels. The red blood cells were reconstituted in diluted human albumin and re-infused. The remainder of the plasma was frozen for later determination of renal function tests.
The animals were then randomly divided into three groups comparable for age and weight. They received increasing doses of nimesulide (provided by Helsinn Healthcare SA, Lugano, Switzerland) administered within 2 min as an i.v. bolus diluted in isotonic saline (500 μL/100 g/BW), flushed with heparinized saline for an additional 3 min, and followed by a continuous infusion (diluted in the modified rabbit Ringer solution) throughout the experiment.
Nimesulide dosage was derived from studies performed on dogs using a bolus of 750 μg/kg + 5 μg · kg−1 · min−1(24). We consequently determined the optimal dose that was effective on renal function without affecting MAP in a preliminary study (data not shown) and designed a dose-range study as follows:
-
Group NIM 2: nimesulide 2 μg/kg + 0.05 μg · kg−1 · min−1 (n = 8; age 5.5 ± 0.4 d; weight 105.5 ± 3.2 g)
-
Group NIM 20: nimesulide 20 μg/kg + 0.5 μg · kg−1 · min−1 (n = 10; age 5.3 ± 0.3 d; weight 114.3 ± 4.9 g)
-
Group NIM 200: nimesulide 200 μg/kg + 5 μg · kg−1 · min−1 (n = 10; age 6.0 ± 0.4 d; weight 97.1 ± 5.4 g)
Renal function was measured again for two additional 30-min experimental urine collections (E1 and E2), with 0.4 mL of blood withdrawn at the midpoint of each collection; the red blood cells were again reconstituted and reinfused. Additional sham-surgery experiments were performed in five rabbits (age 6.4 ± 0.5 day old, weight 114.8 ± 4.6 g) infused with isotonic saline, as in the three NIM groups (500 μL/100 g). The experimental protocol was the same as for the rabbits treated with nimesulide.
Analytical procedures.
Urine flow rate (UV) was assessed gravimetrically. Blood gas determinations were performed using a pH/blood gas analyzer (Blood gas system 248; Bayer Schweiz AG, Zürich, Switzerland). The automatic anthrone method of Wright and Gann (25) and the Bratton and Marshall method (26) were used for the determination of inulin and PAH concentrations, respectively (AutoAnalyzer II; Bran & Luebbe, Nordestedt, Germany). The plasma protein concentration was estimated by refractometry (AOTS meter; American Optical, Buffalo, NY, U.S.A.). Osmolality was measured with a vapor pressure osmometer (Wescor 5520, Logan, UT, U.S.A.).
Inulin and PAH clearances were calculated from standard equations representing GFR and renal plasma flow, respectively. RBF, filtration fraction (FF), and RVR were derived from standard equations as previously reported (20).
A PAH extraction ratio of 0.55 ± 0.04 was used to calculate RBF. This is the usual value found for normoxemic neonatal rabbits in our laboratory (23). No significant difference was found (0.48 ± 0.02; p = 0.06) in the 20 animals in which the extraction was completed at the end of the experiment. Free-water clearance (CH2O) was calculated as the difference between UV and the osmolar clearance: CH2O (mL/kg per min) = UV − (urine osmolality × UV)/plasma osmolality.
Statistical analysis.
All results are given as mean ± SEM. Intragroup comparisons between the control period and periods E1 and E2 were performed on the absolute individual data with the nonparametric Friedman and Wilcoxon signed-rank tests. To avoid inaccuracies as a result of the interindividual variability of the data from the control period, intergroup comparison was performed only on the percentage changes (Fig. 1) with the nonparametric Kruskal-Wallis rank-sum test, and ANOVA followed by Fisher's paired least-significant difference test was used for repeated measurements. Each animal acted as its own control. A p < 0.05 was considered as statistically significant.

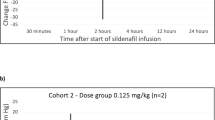
Percentage changes (Δ%) in UV, GFR, RBF, and RVR, in three groups of newborn rabbits after the i.v. administration of increasing doses of nimesulide. Values are means ± SEM of the Δ% of each individual for each group, from the control period to the experimental period E2. *p < 0.05, **p < 0.01 when absolute values of the experimental period are compared with the values of the control period (absolute values presented in Tables 1 and 2); p < 0.05 when Δ% of each group are compared with the two other groups: ‡NIM 200 vs NIM 2, §NIM 200 vs NIM 20.
RESULTS
In the sham-surgery group, the only change seen over time in the hemodynamic and renal function parameters was a slight, albeit significant, increase in GFR, with a resulting increase in FF (GFR: 1.84 ± 0.36 mL · kg−1 · min−1 for control period to 2.01 ± 0.33 mL · kg−1 · min−1 for period E2 (13 ± 6%); FF: 16.0 ± 1.7 to 18.3 ± 1.2%; both p = 0.043). All other parameters were not modified after saline administration (MAP: 36.3 ± 3.2 to 35.6 ± 3.0 mm Hg; UV: 0.060 ± 0.011 to 0.069 ± 0.009 mL · kg−1 · min−1; CH2O: −0.057 ± 0.015 to −0.057 ± 0.014 mL · kg−1 · min−1; RBF: 17.6 ± 2.6 to 16.6 ± 2.4 mL · kg−1 · min−1; RVR: 2.18 ± 0.16 to 2.27 ± 0.16 mm Hg · mL−1 · kg−1 · min−1).
The hemodynamic and renal functional responses to i.v. nimesulide in the three groups are shown in Tables 1 and 2 (absolute data) and Figure 1 (percentage changes). To simplify the presentation, the results for E1 and E2 being similar, percentage changes in Figure 1 are given only for the experimental period E2, compared with the control period.
During the experiments, relatively minor, albeit statistically significant, changes in plasma protein levels and hematocrit were observed. These are recurrent findings in the neonatal animal experiments as a result of repeated blood sampling. However, these changes do not interfere with the physiologic stability of the neonatal model during the time of the experiment.
After the i.v. administration of nimesulide, MAP remained unchanged in the three groups. Diuresis fell significantly in animals that received nimesulide 20 and 200 by −23 and −44% in period E2, respectively (both p < 0.01), but not in those that received the lowest dose (Fig. 1). The same pattern was found for CH2O. The baseline plasma/urine inulin ratio was identical in the three groups (0.039 ± 0.003, 0.036 ± 0.003, and 0.037 ± 0.003, respectively) and remained unchanged whatever the dose of nimesulide. Renal function parameters were significantly modified in all groups with a dose-dependent effect: GFR fell by −12, −23, and −47% in groups NIM 2, NIM 20, and NIM 200, respectively; RBF decreased by −23, −23, and −48%, respectively; meanwhile, RVR increased by 29, 37, and 92%, respectively. FF increased slightly or remained unchanged.
DISCUSSION
The present data clearly demonstrate a dose-dependent increase in RVR in the immature vascular bed after the i.v. administration of nimesulide, with a consequent decrease in urine flow rate, GFR, and RBF. The sham experiments in rabbits that received an infusion of saline confirmed the stability of the model. The slight increase in GFR was probably the result of slight volume expansion, even if the volume injected (500 μL/100 g/BW) was small compared with the rabbit's theoretical blood volume (approximately 8%). These results can obviously not have interfered with the effects of nimesulide as saline administration alone increased GFR, whereas nimesulide decreased it significantly.
The decrease in urine flow rate at the two highest doses is probably due mainly to the decrease in GFR, as suggested by the constant plasma/urine inulin ratio. However, at the lowest dose, GFR significantly decreased with no significant decrease in diuresis or CH2O. Therefore, we cannot rule out that the decrease in diuresis and CH2O could also partly result from a PG-mediated dose-dependent direct effect of nimesulide on free-water reabsorption. Indeed, in fetal lambs, the COX2 inhibitor celecoxib decreased UV and CH2O directly, with no alteration of RBF or creatinine clearance (27). In the adult kidney cortex, constitutive expression of COX2 is found mainly in the thick ascending limb of the loop of Henle (28), which is one of the main sites of water reabsorption. Schumacher et al.(29) recently demonstrated on cryosections of neonatal rabbit kidneys that both COX1 and COX2 are constitutively expressed in the medullary collecting duct, without labeling the cortical collecting duct. This suggests a direct role of COX2 inhibition in the medullary collecting duct. In the renal medulla, PGs decrease medullary hypertonicity and reduce the tubular sensitivity to AVP, thereby promoting free-water excretion. Furthermore, PGE2 has a direct effect on aquaporin 2 (AQP2) distribution in rat inner medulla (30). A decrease in PGE2 production by COX2 inhibitors therefore would lead to a reduction of AQP2 endocytosis and to an increased abundance of AQP2 in the plasma membrane. PGE2 has also been reported to modulate AVP-induced water permeability of the cortical collecting tubule (31). In addition, the prostacyclin (PGI2) analogue iloprost can trigger the urinary excretion of AQP2 in healthy humans, suggesting an increase in AQP2 expression in the collecting duct (32). Altogether, COX2-mediated PG synthesis inhibition with nimesulide could stimulate free-water reabsorption at various sites of water transport in the kidney.
Finally,the COX2/COX1 selectivity ratio of nimesulide can vary greatly depending on the system used for its determination. In vitro, COX2/COX1 IC50 ratios have been reported to range from 0.76 to <0.0001, i.e. from a 1.3- to a 10,000-fold higher COX2 versus COX1 selectivity of nimesulide [see (13) for review (33–35)]. Ex vivo, plasma from volunteers who were given nimesulide produced a marked inhibition of COX2 activity with little effect on COX1 (36). In vivo, nimesulide suppressed endotoxin-induced PGE2 formation, which represents an index for COX2 activity, by 93%, whereas the levels of thromboxane B2, an index of COX1 activity, were nearly unchanged (13%) (37). Likewise, in vivo, nimesulide did not affect COX1-mediated PG synthesis in the bronchial tree and in the gastric mucosa. In contrast, this agent markedly affected COX2-mediated PG production in inflammatory exudate (38). These discrepancies do not allow us to conclude definitely on the selectivity of nimesulide in our model. We therefore cannot totally exclude the possibility that the reduction of CH2O by nimesulide might also result from partial COX1 inhibition, as COX1 is widely expressed in the collecting duct (29).
At all doses, nimesulide administration had a deleterious effect on renal function without affecting MAP, thus ruling out a systemic arterial pressure–related effect. The absence of major changes in FF indicates vasoconstriction of afferent as well as efferent glomerular vessels. Renal vasoconstriction occurred even with the lowest dose of nimesulide, suggesting a great sensitivity of the newborn kidney to COX2 inhibition. It seems that the primary event with low-dose nimesulide would be on the renal microvasculature (RVR is increased), thus decreasing GFR and RBF. An additional decrease in GFR combined with a direct effect of nimesulide on free-water reabsorption would then lead to the decrease in urine flow rate seen at the two higher doses.
The present data reinforce those previously observed in our laboratory with the infusion of nonselective NSAIDs (19–22) (Table 3). A similar pattern of response was observed with indomethacin, aspirin, and ibuprofen, which have been demonstrated to be more potent inhibitors of COX1 than COX2 in all models used (39). Interesting enough, the response of adult rabbits to aspirin administration was attenuated compared with the newborns (21). The overall data therefore suggest a major role of both COX1 and COX2 isoforms-derived PGs in protecting the newborn kidney, which is perfused at low renal arterial pressure. Indeed, it has been demonstrated that the low renal expression of COX2 at birth increases rapidly in the first two postnatal weeks, before gradually declining to low levels in normal adult rats and rabbits (29, 40). Likewise, newborn infants have high plasma levels of vasodilating PGs that modulate the highly activated vasoconstrictor state of the neonatal renal circulation (41). COX2 is widely expressed in the macula densa, cortical thick ascending limb, juxtamedullary glomeruli, and medullary interstitial cells. Expression has also been documented in the cortical vasculature (endothelial and smooth muscle cells of arteries and veins, arterioles, vasa recta) and podocytes, suggesting an additional role in the regulation of glomerular hemodynamics through their contraction (42, 43). Thus, COX2 inhibition would impair the renal autoregulation, resulting in an increase in RVR with a marked reduction in GFR and RBF, as seen in the present study. These changes can be explained by the direct inhibition of COX2-mediated PG synthesis. Indeed, in a purified enzyme assay in vitro, nimesulide caused a concentration-related inhibition of PGE2 formation by COX2 (IC50 90.3 μM), with no inhibition of PGE production by COX1, suggesting that nimesulide was specific for COX2 (44). Nimesulide infusion to pregnant ewes also decreased fetal plasma PGE2 concentrations significantly (45), even at low maternal doses consistent with the ones we used in the present study (46). Nimesulide 0.01, 0.1, and 1 mg/kg induced a 35, 82, and 94% reduction, respectively, of PGE2 fetal carotid artery concentrations, indicating effective suppression of COX2 activity (46). In addition, nimesulide may have a dual inhibitory effect on PG levels, not only by decreasing the activity of COX2 but also its formation by suppressing COX2 mRNA expression and protein synthesis (45). Accordingly, the GFR of COX2-deficient mice was reduced by approximately 50%, as compared with normal wild-type controls (47).
COX2 inhibition with nimesulide may also have unveiled the constrictor effect of angiotensin II. The kidneys of fetal and newborn experimental animals are known to synthesize and secrete renin in abundance (48). In the newborn rabbit, total renin concentration increases with postnatal age and relatively more than kidney weight between 1 and 2 wk of age (49). We previously showed, using the angiotensin-converting enzyme inhibitor perindoprilat, that the renin-angiotensin system plays an important role in regulating renal function in the newborn rabbit (50). Renal PGs are thought to modulate renin expression and secretion in response to changes in renal perfusion. Conflicting results showed that selective inhibition of COX2 attenuated urinary prostanoid excretion without affecting renal renin expression but also blunted the stimulation of renin secretion and renin gene expression in response to renal hypoperfusion (51, 52). Likewise, Qi et al.(51) demonstrated that COX2 deletion or inhibition amplifies the pressor response to exogenous angiotensin II and reveals a depressive effect of endogenous angiotensin II on medullary blood flow. Finally, a partial inhibition by nimesulide of COX1 in the glomerulus cannot be totally excluded from the present results, as discussed earlier for the collecting duct.
Tocolysis with nonselective NSAIDs has been widely accepted for many years, owing to their capacity to inhibit PG-induced initiation and maintenance of labor. In 1978, Novy (5) documented the occurrence of irreversible renal failure in indomethacin-exposed rhesus monkey fetuses. Since then, reports of the use of nonselective NSAIDs in experimental animals and humans have showed an increased incidence of oligohydramnios as a result of a decrease of fetal renal function (9, 11, 53, 54). In addition to the hemodynamic side effects, renal dysgenesis was reported (9, 54). In the embryonic kidney, both isoforms COX1 and COX2 are constitutively expressed, notably in cells undergoing induction and/or morphogenesis (52). Not surprising, tocolysis with the COX2-preferential inhibitor nimesulide was associated with fetal side effects similar to those described with indomethacin, i.e. severe reversible oligohydramnios or neonatal renal failure (15–18, 55). Morphology was suggestive of delayed glomerular development and interstitial fibrosis, or partial abnormal tubular differentiation with subacute tubulointerstitial nephritis and interstitial inflammation (17, 18). Renal dysgenesis was also reported in mice that had targeted disruption of the COX2 gene (56) or that were treated with the specific COX2 inhibitor SC58236 (57).
CONCLUSION
The present results do not support the claim that preferential COX2 inhibition may be safer for the kidney than nonselective COX inhibition. They confirm that the COX2-mediated synthesis of PGs, by maintaining afferent and efferent vasodilatory tones, plays a major role in the physiologic preservation of glomerular filtration and RBF in the neonatal period. On the basis of the present data and experimental work by others on the role of COX2 in fetal development, all NSAIDs, nonselective and COX2 selective/preferential, should be used with great caution during pregnancy and in the neonatal period.
Abbreviations
- AQP2:
-
aquaporin 2
- CH2O:
-
free-water clearance
- COX:
-
cyclooxygenase
- FF:
-
filtration fraction
- HR:
-
heart rate
- MAP:
-
mean arterial blood pressure
- NSAID:
-
nonsteroidal anti-inflammatory drug
- PAH:
-
para-aminohippuric acid
- PG:
-
prostaglandin
- RBF:
-
renal blood flow
- RVR:
-
renal vascular resistance
- UV:
-
urine flow rate
References
Heyborne KD 2000 Preeclampsia prevention: lessons from the low-dose aspirin therapy trials. Am J Obstet Gynecol 183: 523–528
Stika CS, Gross GA, Leguizamon G, Gerber S, Levy R, Mathur A, Bernhard LM, Nelson DM, Sadovsky Y 2002 A prospective randomized safety trial of celecoxib for treatment of preterm labor. Am J Obstet Gynecol 187: 653–660
Macones GA, Marder SJ, Clothier B, Stamilio DM 2001 The controversy surrounding indomethacin for tocolysis. Am J Obstet Gynecol 184: 264–272
Hammerman C, Kaplan M 2001 Comparative tolerability of pharmacological treatments for patent ductus arteriosus. Drug Saf 24: 537–551
Novy MJ 1978 Effects of indomethacin on labor, fetal oxygenation and fetal development in rhesus monkeys. Adv Prostaglandin Thromboxane Res 4: 285–300
Cantor B, Tyler T, Nelson RM, Stein GH 1980 Oligohydramnios and transient neonatal anuria: a possible association with the maternal use of prostaglandin synthetase inhibitors. J Reprod Med 24: 220–223
Vanhaesebrouck P, Thiery M, Leroy JG, Govaert P, de Praeter C, Coppens M, Cuvelier C, Dhont M 1988 Oligohydramnios, renal insufficiency and ileal perforation in preterm infants after intrauterine exposure to indomethacin. J Pediatr 113: 738–743
Simeoni U, Messer J, Weisburd P, Haddad J, Willard D 1989 Neonatal renal dysfunction and intrauterine exposure to prostaglandin synthesis inhibitors. Eur J Pediatr 148: 371–373
van der Heijden BJ, Carlus C, Narcy F, Bavoux F, Delezoide AL, Gubler MC 1994 Persistent anuria, neonatal death, and renal microcystic lesions after prenatal exposure to indomethacin. Am J Obstet Gynecol 171: 617–623
Cuzzolin L, Dal Cerè M, Fanos V 2001 NSAID-induced nephrotoxicity from the fetus to the child. Drug Saf 24: 9–18
Schoenfeld A, Bar Y, Merlob P, Ovadia Y 1992 NSAIDs: maternal and fetal considerations. Am J Reprod Immunol 28: 141–147
Bennett A 2001 Nimesulide: a well-established cyclooxygenase-2 inhibitor with many other pharmacological properties relevant to inflammatory diseases. In: Vane JR, Botting RM (eds) Therapeutic Roles of Selective COX-2 Inhibitors. William Harvey Press, London, 524–540.
Famaey JP 1997 In vitro and in vivo pharmacological evidence of selective cyclooxygenase-2 inhibition by nimesulide: an overview. Inflamm Res 46: 437–446
Sawdy R, Slater D, Fisk N, Edmonds DK, Bennett P 1997 Use of a cyclooxygenase type-2-selective non-steroidal anti-inflammatory agent to prevent preterm delivery. Lancet 350: 265–266
Holmes RP, Stone PR 2000 Severe oligohydramnios induced by cyclooxygenase-2 inhibitor nimesulide. Obstet Gynecol 96: 810–811
Landau D, Shelef I, Polacheck H, Marks K, Holcberg G 1999 Perinatal vasoconstrictive renal insufficiency associated with maternal nimesulide use. Am J Perinatol 16: 441–444
Peruzzi L, Gianoglio B, Porcellini MG, Coppo R 1999 Neonatal end-stage renal failure associated with maternal ingestion of cyclo-oxygenase-type-2 selective inhibitor nimesulide as tocolytic. Lancet 354: 1615
Balasubramaniam J 2000 Nimesulide and neonatal renal failure. Lancet 355: 575
Duarte-Silva M, Gouyon JB, Guignard JP 1986 Renal effects of indomethacin and dopamine in newborn rabbits. Kidney Int 30: 455–456
Chamaa NS, Mosig D, Drukker A, Guignard JP 2000 The renal hemodynamic effects of ibuprofen in the newborn rabbit. Pediatr Res 48: 600–605
Drukker A, Mosig D, Guignard JP 2001 The renal hemodynamic effects of aspirin in newborn and young adult rabbits. Pediatr Nephrol 16: 713–718
Guignard JP 2002 The adverse renal effects of prostaglandin synthesis inhibitors in the newborn rabbit. Semin Perinatol 26: 398–405
Gouyon JB, Valloton M, Guignard JP 1987 The newborn rabbit: a model for studying hypoxemia-induced renal changes. Biol Neonate 52: 115–120
Llinas MT, Rodriguez F, Moreno C, Salazar FJ 2000 Role of cyclooxygenase-2-derived metabolites and nitric oxide in regulating renal function. Am J Physiol 279: R1641–R1646
Wright HK, Gann DS 1966 An automatic anthrone method for the determination of inulin in plasma and urine. J Lab Clin Med 67: 689–693
Bratton AC, Marshall EK 1939 A new coupling component for sulfanilamide determination. J Biol Chem 128: 537–550
Kajino H, Roman C, Clyman RI 2002 Renal effects of cyclooxygenase-2 inhibition in fetal lambs. Biol Neonate 82: 257–262
Kammerl MC, Nusing RM, Seyberth HW, Riegger GA, Kurtz A, Kramer BK 2001 Inhibition of cyclooxygenase-2 attenuates urinary prostanoid excretion without affecting renal renin expression. Pflugers Arch 442: 842–847
Schumacher K, Castrop H, Strehl R, de Vries U, Minuth WW 2002 Cyclooxygenases in the collecting duct of neonatal rabbit kidney. Cell Physiol Biochem 12: 63–74
Zelenina M, Christensen BM, Palmer J, Nairn AC, Nielsen S, Aperia A 2000 Prostaglandin E(2) interaction with AVP: effects on AQP2 phosphorylation and distribution. Am J Physiol 278: F388–F394
Stokes JB 1985 Modulation of vasopressin-induced water permeability of the cortical collecting tubule by endogenous and exogenous prostaglandins. Miner Electrolyte Metab 11: 240–248
Buemi M, Di Pasquale G, Ruello A, Floccari F, Aloisi C, Latassa G, Corsonello A, Sturiale A, Corica F, Frisina N 2002 Effect of a prostacyclin analogue, iloprost, on urinary aquaporin-2 excretion in humans. Nephron 91: 197–202
Riendeau D, Percival MD, Brideau C, Charleson S, Dube D, Ethier D, Falgueyret JP, Friesen RW, Gordon R, Greig G, Guay J, Mancini J, Ouellet M, Wong E, Xu L, Boyce S, Visco D, Girard Y, Prasit P, Zamboni R, Rodger IW, Gresser M, Ford-Hutchinson AW, Young RN, Chan CC 2001 Etoricoxib (MK-0663): preclinical profile and comparison with other agents that selectively inhibit cyclooxygenase-2. J Pharmacol Exp Ther 296: 558–566
Toutain PL, Cester CC, Haak T, Metge S 2001 Pharmacokinetic profile and in vitro selective cyclooxygenase-2 inhibition by nimesulide in the dog. J Vet Pharmacol Ther 24: 35–42
Range SP, Pang L, Holland E, Knox AJ 2000 Selectivity of cyclo-oxygenase inhibitors in human pulmonary epithelial and smooth muscle cells. Eur Respir J 15: 751–756
Giuliano F, Ferraz JGP, Pereira R, de Nucci G, Warner TD 2001 Cyclooxygenase selectivity of non-steroid anti-inflammatory drugs in humans: ex vivo evaluation. Eur J Pharmacol 426: 95–103
Nusing RM, Reinalter SC, Peters M, Komhoff M, Seyberth HW 2001 Pathogenetic role of cyclooxygenase-2 in hyperprostaglandin E syndrome/antenatal Bartter syndrome: therapeutic use of the cyclooxygenase-2 inhibitor nimesulide. Clin Pharmacol Ther 70: 384–390
Bernareggi A 1998 Clinical pharmacokinetics of nimesulide. Clin Pharmacokinet 35: 247–274
Mitchell JA, Akarasereenont P, Thiemermann C, Flower RJ, Vane JR 1993 Selectivity of nonsteroidal antiinflammatory drugs as inhibitors of constitutive and inducible cyclooxygenase. Proc Natl Acad Sci U S A 90: 11693–11697
Zhang MZ, Wang JL, Cheng HF, Harris RC, McKanna JA 1997 Cyclooxygenase-2 in rat nephron development. Am J Physiol 273: F994–F1002
Chevalier R 1993 Atrial natriuretic peptide in renal development. Pediatr Nephrol 7: 653–656
Harris RC 2002 Cyclooxygenase-2 inhibition and renal physiology. Am J Cardiol 89: 10D–17D
Kömhoff M, Gröne HJ, Klein T, Seyberth HW, Nüsing RM 1997 Localization of cyclooxygenase-1 and -2 in adult and fetal human kidney: implication for renal function. Am J Physiol 272: F460–F468
Tavares IA, Bishai PM, Bennett A 1995 Activity of nimesulide on constitutive and inducible cyclooxygenases. Arzneimittelforschung 45: 1093–1095
Wu WX, Unno N, Ma XH, Nathanielsz PW 1998 Inhibition of prostaglandin production by nimesulide is accompanied by changes in expression of the cassette of uterine labor-related genes in pregnant sheep. Endocrinology 139: 3096–3103
Poore KR, Young IR, Hirst JJ 1999 Efficacy of the selective prostaglandin synthase type 2 inhibitor nimesulide in blocking basal prostaglandin production and delaying glucocorticoid-induced premature labor in sheep. Am J Obstet Gynecol 180: 1244–1253
Norwood VF, Morham SG, Smithies O 2000 Postnatal development and progression of renal dysplasia in cyclooxygenase-2 null mice. Kidney Int 58: 2291–2300
Drukker A, Goldsmith DI, Spitzer A, Edelmann CM, Blaufox MD 1980 The renin angiotensin system in newborn dogs: developmental patterns and response to acute saline loading. Pediatr Res 14: 304–307
Drukker A, Donoso VS, Linshaw MA, Bailie MD 1983 Intrarenal distribution of renin in the developing rabbit. Pediatr Res 17: 762–765
Huet F, Semama DS, Gouyon JB, Guignard JP 1999 Protective effect of perindoprilat in the hypoxemia-induced renal dysfunction in the neonatal rabbit. Pediatr Res 45: 138–142
Qi Z, Hao CM, Langenbach RI, Breyer RM, Redha R, Morrow JD, Breyer MD 2002 Opposite effects of cyclooxygenase-1 and -2 activity on the pressor response to angiotensin II. J Clin Invest 110: 61–69
Thomas MC, Harris DCH 2002 Renal effects of cyclo-oxygenase-2 inhibition. Nephrology 7: 281–286
Matson JR, Stokes JB, Robillard JE 1981 Effects of inhibition of prostaglandin synthesis on fetal renal function. Kidney Int 20: 621–627
Kaplan BS, Restaino I, Raval DS, Gottlieb RP, Bernstein J 1994 Renal failure in the neonate associated with in utero exposure to non-steroidal anti-inflammatory agents. Pediatr Nephrol 8: 700–704
Locatelli A, Vergani P, Bellini P, Strobelt N, Ghidini A 2001 Can a cyclo-oxygenase type-2 selective tocolytic agent avoid the fetal side effects of indomethacin?. BJOG 108: 325–326
Dinchuk JE, Car BD, Focht RJ, Johnston JJ, Jaffee BD, Covington MB, Contel NR, Eng VM, Collins RJ, Czerniak PM, Gorry SA, Trzaskos JM 1995 Renal abnormalities and an altered inflammatory response in mice lacking cyclooxygenase II. Nature 378: 406–409
Kömhoff M, Wang JL, Cheng HF, Langenbach R, McKanna JA, Harris RC, Breyer MD 2000 Cyclooxygenase-2-selective inhibitors impair glomerulogenesis and renal cortical development. Kidney Int 57: 414–422
Acknowledgements
We thank M. Julita and M. Thonney Viani for skillful technical help and valuable contributions in the laboratory.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by the Swiss National Science Foundation (grant nos. 3200-052463.97/1 and 3200-064041.00).Presented in part at the 7th Congress of the European Society for Developmental, Perinatal & Pediatric Pharmacology, Limassol, Cyprus, November 2001; and at the 36th Annual Meeting of the European Society for Pediatric Nephrology, Bilbao, Spain, September 2002.
Rights and permissions
About this article
Cite this article
Prévot, A., Mosig, D., Martini, S. et al. Nimesulide, a Cyclooxygenase-2 Preferential Inhibitor, Impairs Renal Function in the Newborn Rabbit. Pediatr Res 55, 254–260 (2004). https://doi.org/10.1203/01.PDR.0000100904.17064.47
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/01.PDR.0000100904.17064.47
This article is cited by
-
Use of Nimesulide During Early Pregnancy and the Risk of Congenital Malformations: A Population-Based Study from Italy
Advances in Therapy (2018)
-
Maternal ingestion of diclofenac leading to renal failure in newborns
Pediatric Nephrology (2012)
-
Beneficial effect of insulin-like growth factor-1 on hypoxemic renal dysfunction in the newborn rabbit
Pediatric Nephrology (2009)
