
Abstract
Since the start of the COVID-19 pandemic, pertinent conspiracy theories have proliferated online, raising the question: How might believing in those conspiracy theories be linked with engagement in disease-preventive behaviours? To answer this, we conducted a repeated cross-sectional survey of around 1500 respondents to examine the link between conspiracy-theory beliefs and disease-preventive behaviours across six time-points in the United States from early February to late March 2020. The findings reveal that believing in risk-acceptance conspiracy theories (RA-CTs; e.g., “COVID-19 is a man-made bioweapon”) was linked to more preventive behaviours. However, believing in risk-rejection conspiracy theories (RR-CTs; e.g., “COVID-19 is like influenza and was purposefully exaggerated”) was associated with fewer preventive behaviours. These differential links were mediated by risk perception and negative emotions and modulated by the stage of the outbreak—RA-CTs predicted higher risk perception in the mild stage, whereas RR-CTs predicted lower risk perception in the severe stage.
Similar content being viewed by others


Introduction
Since early days of the COVID-19 outbreak in January 2020, conspiracy theories pertaining to the novel coronavirus (SARS-CoV-2) and the disease it causes (COVID-19) have been circulating on social media and mainstream media platforms around the world (e.g., Islam et al., 2020). A common assumption is that people believing in the pandemic-related conspiracy theories would be less likely to take actions to prevent the virus’ spread (cf. Law, 2020 September 21). Likewise, medical professionals have expressed similar concerns that endorsing conspiracy theories could dampen trust in the medical institution, resulting in non-compliance with disease-prevention practices (e.g., Earnshaw et al., 2019; Sell et al., 2020; see Gonçalves-Sá, 2020). The current research examines how true this perceived link is, as well as the circumstances under which this link may be reversed—i.e., if/when believing in certain types of pandemic-related conspiracy theories is associated with higher rather than lower engagement in disease-preventive behaviours. Findings would be useful for combating public health crises. In the following, we will first elucidate two major types of COVID-19-related conspiracy theories and review how they were linked with disease-preventive behaviours. We will then delineate the knowledge gap and provide empirical findings to address the gap.
Conspiracy theories typically refer to as “an explanation of historical, ongoing, or future events that cites as a main causal factor a group of powerful persons, the conspirators, acting in secret for their own benefit against the common good” (Uscinski, 2018, p. 235; cf. van Prooijen and Van Vugt, 2018). A conspiracy theory is different from a conspiracy, in which the former is a perceived accusation of unknown validity and the latter is a true causal chain of events (see Douglas et al., 2019). Given its sudden emergence and its immense global impact, people sought explanations for the COVID-19 pandemic. However, there is a lack of authoritative scientific consensus on the source of the virus, its spread and containment, and the long-term social and economic ramifications of the pandemic. As a result, researchers (e.g., Shahsavari et al., 2020) have argued that people create and share conspiracy-theory narratives, such that “a single unifying corpus of special or secret knowledge does not yet exist—there are no ‘smoking guns’ to which the conspiracy theorists can point” (p. 16). Instead, conspiracy narratives are partial stories that activate some small group of actants and relationships available in the broader discourse. By analysing tens of thousands of social media posts and news stories on conspiracy theories related to the COVID-19 pandemic, Shahsavari et al. (2020) uncovered several major conspiracy-theory narratives, including: the COVID-19 virus escaped from a Chinese biological weapons laboratory, most likely in Wuhan, either as part of a deliberate release or accidentally; the 5G cellular network is the root cause of the virus; Bill Gates is using the virus as a cover for his desire to create a worldwide surveillance state through the enforcement of a global vaccination programme; the pandemic is a plot of QAnon; the pandemic is a hoax, if anything, no more than a common flu. Importantly, the researchers noted that participants in an online conversation rarely recount the entire scope of a story, choosing instead to tell only parts of it.
Among the conspiracy-theory narratives identified, some seemingly accepted the pandemic as a severe threat (e.g., the novel coronavirus is a human-made virus leaking from a bioweapon laboratory), whereas others seemingly dismissed the threat (e.g., the pandemic is a hoax). Belief in these two types of conspiracy theories or related rumours have been found to link to different behavioural patterns (Imhoff and Lamberty, 2020; Oleksy et al., 2021; Sternisko et al., 2020). In particular, in a study conducted during late March with participants from the United States, the United Kingdom, and Germany, Imhoff and Lamberty (2020) found that holding the conspiracy belief of COVID-19 as a human-made crisis was related to more self-centred prepping behaviour (e.g., stocking up on supplies), whereas holding the conspiracy belief of COVID-19 as a hoax was related to less disease-preventive behaviour (e.g., maintaining personal hygiene, practicing physical distancing) and more self-centred prepping behaviours, though the effect was weaker compared with the belief in COVID-19 as a human-made crisis. In another study conducted during late April with a sample of British participants, Sternisko et al. (2020; Study 2) found that believing in the conspiracy view of COVID-19 as a hoax was related to less social distancing and policy support, while believing in the conspiracy theory of COVID-19 as a human-made crisis was related to more handwashing but also less social distancing and policy support. Taken together, these studies link the two types of conspiracy-theory beliefs—a risk-acceptance type of conspiracy-theory belief (e.g., COVD-19 is a human-made crisis) versus a risk-rejection type of conspiracy-theory belief (e.g., COVID-19 is a hoax)—to different behavioural patterns.
To the extent that conspiracy theories represent a causal explanation for the occurrence of social crises (e.g., Jolley and Douglas, 2014; van Prooijen and Van Vugt, 2018), believing in different types of conspiracy theories may reflect the endorsers’ implicit appraisals of COVID-19, i.e., how people evaluate the level of danger that they and other people face, as well as negative emotions they feel about the crisis (e.g., worry, anxiety) (Klofstad et al., 2019). We therefore hypothesise that belief in the risk-acceptance type of conspiracy theory is associated positively with risk perception and negative emotions toward COVID-19 (Hypothesis 1a), which in turn is positively related to disease-preventive behaviours (Hypothesis 1b). We predict this association because much research has shown that disease-related risk perception and threat feelings play a prominent role in driving disease-preventive behaviours (for reviews, see Noar and Zimmerman, 2005; Sheeran et al., 2014). We also hypothesise that belief in the risk-rejection type of COVID-19 conspiracy theory is associated negatively with risk perception and negative emotions toward COVID-19 (Hypothesis 2a), which is in turn negatively related to disease-preventive behaviours (Hypothesis 2b). Testing these hypotheses allowed us to contribute to the literature by first validating previous findings (Imhoff and Lamberty, 2020; Sternisko et al., 2020), and then shedding light on the knowledge gap regarding the psychological mechanism underlying the differential links between conspiracy theories and disease-preventive behaviours.
Finally, extending beyond previous findings, we also tested how the two types of conspiracy-theory beliefs may matter differently at different stages of the COVID-19 pandemic. Specifically, we speculated that the associations between the two types of COVID-19 conspiracy-theory beliefs and disease-preventive behaviours could change according to the severity of the outbreak/pandemic. Previous studies have shown that people tend to underestimate the risk of a threat when it provides a high level of psychological distance (Chandran and Menon, 2004; Johnson, 2018; Zwickle and Wilson, 2014). As such, people’s risk perception and disease-preventive behaviours could be lower at an earlier stage of the pandemic than at a later stage. However, because the risk-acceptance type of conspiracy theory portrays COVID-19 as a real threat, endorsers of this type of conspiracy theory would perceive higher risk and experience more negative emotions than would non-endorsers, even at an early stage of the outbreak. By contrast, at a later stage when the pandemic is more severe, the risk-rejection type of conspiracy theory could become impactful because it denies the threat and dampens otherwise strong risk perception and negative emotions. As a result, endorsers of the risk-rejection type of conspiracy theory would show lower risk perception and negative emotions than would non-endorsers at the later stage. Taken as a whole, we predict that the links between believing in risk-acceptance conspiracy theories and risk perception and negative emotions would be stronger at the less-severe stage of the COVID-19 outbreak (Hypothesis 3a), and that the links between believing in the risk-rejection type of conspiracy theory and risk perception and negative emotions would be stronger at the more-severe stage of the COVID-19 outbreak (Hypothesis 3b). These differential links with risk perception and negative emotions would in turn be associated with differential levels of disease-preventive behaviours. As a result, belief in the risk-acceptance conspiracy theories would be associated more strongly with greater disease-preventive behaviours in the early stage than in the later, more-severe stage of the COVID-19 pandemic (Hypothesis 4a). By contrast, belief in risk-rejection conspiracy theories would be associated more strongly with less disease-preventive behaviours in the later stage than in the early stage of the COVID-19 pandemic (Hypothesis 4b).
Methods
Procedures
To test our predictions, we conducted a repeated cross-sectional survey across six-time-points in the United States, covering the period from early February (mild stage of the outbreak: 11 confirmed cases in the U.S.) to late March (severe stage of the outbreak: 68,440 in the U.S.) with a survey conducted every ten days. This time frame was decided a priori to capture variations in the severity of the COVID-19 outbreak in the U.S. as much as possible given our limited funding and resources. We will provide validation of this time frame in the Results section.
Participants
We targeted 250 adult U.S. participants at each time-point. This sample size has 80% statistical power to detect a weak-to-moderate correlational strength with alpha at 0.05 level at each time-point. To ensure that the sample at each time-point was comparable to those at other time-points, we recruited participants from the same participant pool. In total, we recruited 1515 participants for all six time-points via Cloudresearch (Litman et al., 2017), a research-tool platform that recruits participants from Amazon Mechanical Turk. The data collection procedures and research materials were reviewed and approved by the Committee on Research Practices of the university affiliated with the corresponding authors (Reference number: SBRE-19-294). All participants gave their consent first and then completed the online survey, only once each (see also Supplementary Information for the details of the consent form and debriefing note). We included three attention-check items following the recommendation of past studies (e.g., Curran, 2016). Specifically, participants were required to provide exactly the same answer as instructed (e.g., “This is an attention-check item; please click “strongly agree” to pass this attention check.”). Seven participants failed all three attention-check items and were removed from the subsequent analyses. Supplementary Table 1 shows the sample characteristics of the participants at each time-point. Results showed high similarities in the demographic characteristics of the samples across the six time-points, suggesting that it is possible to compare findings across these samples.
Measures
Belief in COVID-19 Conspiracy Theories
To create the risk-acceptance and risk-rejection types of conspiracy-theory items, we collected frequently mentioned conspiracy theory narratives from news reports (e.g., BBC News), social media (e.g., Facebook, Twitter), and fact-checking sites (e.g., Snopes.com, Fackcheck.org) in January 2020. Based on the narratives collected, we generated five items to capture risk-acceptance conspiracy theories: “The outbreak of the novel coronavirus is caused by some organisations and countries on purpose in order to fulfil their secret plans;” “The spread of the novel coronavirus is caused by some people intentionally;” “The novel coronavirus is a bioweapon created by the Chinese government;” “The novel coronavirus was stolen by Chinese spies from a laboratory in Canada;” and “The Chinese government has covered up the true number of people infected by the novel coronavirus.” We generated two items to capture risk-rejection conspiracy theories: “In reality, the novel coronavirus is similar to influenza. It is just that some organisations and people purposefully exaggerate its severity;” and “The novel coronavirus actually does not spread easily among humans; it is being used as an excuse to control the influx of Chinese people by foreign countries.” Participants reported on an 11-point scale (0 = not true at all to 10 = completely true) to indicate the extent to which they believed each statement to be true. These two types of items resemble the COVID-human-made and COVID-hoax items used in Imhoff and Limberty (2020) and Sternisko et al. (2020). To validate these conspiracy-theory items, we conducted a social media-engagement search in a retrospective manner (for details, see Supplementary Information; see also Supplementary Tables 7 and 8), and found that these items have sufficient coverage of popular real-life conspiracy theories that were circulating on social media from January to March 2020. Footnote 1 We computed a mean score for each type of conspiracy theory.Footnote 2 Supplementary Table 2 shows the mean, standard deviation, and reliability of the measures. Footnote 3
Our generation of the items was limited by two major constraints. First, the social discourse regarding the novel coronavirus and its spread was still evolving in January 2020 when we created the items. Some of the conspiracy theories, such as the 5G- and Bill Gates-related conspiracy theories, were not yet widely circulated at that stage, and thus we have not included them in our measure. Second, incidentally, there were many more conspiracy theories portraying COVID-19 as a human-caused crisis than as a hoax during that period. Accordingly, we included more risk-acceptance than risk-rejection items in our measure.
Risk perception
We identified three items to capture individuals’ perceived risk of getting infected with COVID-19 from past studies on the perceived risk of infectious disease (e.g., Piltch‐Loeb et al., 2019). Participants indicated the likelihood with which they believed someone in their local community, their family, or themselves to be to contract COVID-19 on a 7-point scale (1 = not at all likely to 7 = extremely likely). We computed a mean score based on the three items. Supplementary Table 2 shows the mean, standard deviation, and reliability of the measure.
Negative emotions toward COVID-19
We identified eight emotional-state items to capture people’s feelings toward COVID-19. Five of the items were negative emotions: afraid, threatened, anxious, tense, and disgusted. Three of the items were positive emotions: optimistic, calm, and hopeful. Participants reported on a 7-point scale (1 = not at all to 7 = extremely) to indicate their feelings toward the COVID-19 outbreak. Confirmatory factor analysis showed a good fit for a two-factor solution (CFI = 0.990, TLI = 0.983, RMSEA = 0.060). We computed a mean score for negative emotions and positive emotions, respectively. Supplementary Table 2 shows the mean, standard deviation, and reliability of the measures.
We did not include positive emotions toward COVID-19 in our main analysis because we did not theorise a causal impact of such positive emotions on disease-preventive behaviours. On the one hand, it is plausible that positive emotions empower people to engage more in disease-preventive behaviours. On the other hand, positive emotions may reassure people that COVID-19 does not represent a real threat. Consequently, positive emotions could possibly impede people from engaging in disease-preventive behaviours. We explored this issue empirically and found that positive emotions toward COVID-19 had a slight negative correlation with disease-preventive behaviours (r = −0.05, N = 1508). We also performed a supplementary analysis to probe the relationship between belief in COVID-19 conspiracy theories and positive emotions toward COVID-19 (see Supplementary Table 6). Belief in the risk-acceptance type of COVID-19 conspiracy theory was unrelated to positive emotions toward COVID-19, whereas belief in the risk-rejection type of COVID-19 conspiracy theory was positively related to positive emotions toward COVID-19. Furthermore, our results remained consistent when we included positive emotions toward COVID-19 as a covariate in the parallel mediation analysis. Positive emotions toward COVID-19 were non-significant in predicting disease-preventive behaviours in the mediation analysis (b = 0.02, SE = 0.01, p = 0.189, 95% CI = [−0.01, 0.05]).
Disease-preventive behaviours
We identified 10 disease-preventive behaviours based on the recommendations from the U.S. Centers for Disease Control and Prevention (CDC) and those recommended in countries that had earlier outbreaks (e.g., the Chinese Center for Disease Control and Prevention). Specifically, participants reported on a five-point scale (1 = never to 5 = always) to indicate how frequently they performed the following behaviours in the past week: “Wear a mask in public places,” “Wash hands with soap and water for at least 20 s or use an alcohol-based hand sanitiser,” “Wash hands before touching eyes, nose, and mouth,” “Avoid leaving home,” “Change clothes and wash hands when coming back from outside immediately upon returning home,” “Avoid crowded areas,” “Pay close attention to household and personal hygiene,” “Avoid travelling to areas where the novel coronavirus is prevalent,” “Avoid taking public transport,” and “Keep monitoring one’s own body temperature.” We computed a mean score to indicate people’s overall engagement in disease-preventive behaviours. Supplementary Table 2 shows the mean, standard deviation, and reliability of the measure.
Covariates
Institutional trust
Conceptually, conspiracy theories may also lead to reduced trust in scientists, governments, and medical institutions, and thus may make people less likely to adopt recommendations from these agents (Earnshaw et al., 2019; Sell et al., 2020). Therefore, we also controlled for the effect of institutional trust to rule out this alterative mechanism. To this end, we created a four-item measure of trust in U.S. institutions based on past studies (e.g., Piltch‐Loeb et al., 2019). Participants reported on a 7-point scale (1 = not at all to 7 = extremely) to indicate the extent to which they were confident in scientists’, medical experts’, the U.S. government’s, and the CDC’s ability to control the spread of COVID-19. Supplementary Table 2 shows the mean, standard deviation, and reliability of the measure.
Political ideology
Previous research (e.g., Calvillo et al., 2020; Georgious et al., 2020; Uscinski et al., 2020) suggested that political ideology may be related to COVID-19 conspiracy beliefs, risk perception, and disease-preventive behaviours. Although it would be interesting to study the effects of political ideology systematically, it is beyond the scope of the current research. We thus controlled for the effects of political ideology. Participants were asked to report the extent to which they endorse liberal and conservative ideologies, respectively. As these two items were strongly correlated (r = −0.78, N = 1508), we computed an average score to represent political ideology, with higher scores indicating higher levels of endorsement of conservative ideology.
Demographic information
We also included demographic variables (gender, age, education level, and annual household income) as covariates; participants reported their gender (1 = male and 0 = female), age, education level (1 = some elementary school or below, 2 = elementary school, 3 = middle school, 4 = high school or equivalent, 5 = some college/associate degree, 6 = bachelor’s degree, 7 = master’s degree, and 8 = professional or Ph.D), and annual household income (1 = less than $10,000; 2 = $10,000 to $39,999; 3 = $40,000 to $69,999; 4 = $70,000 to $99,999; and 5 = $100,000 or more). Participants also indicated their subjective socio-economic-status on a ladder of social-economic status (1 = lowest status to 10 = highest status), ethnicity and political party affiliation; these variables were used to gauge the background characteristics of the six samples.
Supplementary Table 1 shows the sampling characteristics. As shown, the sample characteristics of the participants at each time-point were highly similar, suggesting that it is possible to compare findings across the six samples.
Statistical analysis
To test our hypotheses, we conducted three sets of analysis with SPSS 25.0. First, we conducted a zero-order correlation analysis to test the bivariate relationships among the key variables in the pooled sample (all six time-points) and for each time-point separately. We used the “ggplot” package of R to visualise these bivariate associations for each time-point (see Figs. 1 and 2).

Note. The scatterplot illustrates the bivariate relationship between belief in the risk-acceptance type of COVID-19 conspiracy theories (x-axis; ranged from 0 to 10) and disease-preventive behaviours (y-axis; ranged from 1 to 5) across the six-time points of data collection. The red line illustrates the linear trend of the bivariate relationship.

Note. The scatterplot illustrates the bivariate relationship between belief in the risk-rejection type of COVID-19 conspiracy theories (x-axis; ranged from 0 to 10) and disease-preventive behaviours (y-axis; ranged from 1 to 5) across the six-time points of data collection. The red line illustrates the linear trend of the bivariate relationship.
Next, we conducted a parallel mediation analysis using the SPSS Macro application PROCESS (Hayes, 2013), since we hypothesised both risk perception and negative emotions to be simultaneously mediating the relationship between conspiracy-theory beliefs and disease-preventive behaviour. The PROCESS application enabled researchers to estimate the indirect effects of independent variables via multiple mediator variables simultaneously and generated bootstrap estimates for these indirect effects (Hayes, 2013). In this analysis, we included the extent of believing in the two types of conspiracy beliefs (risk acceptance and risk rejection) as the independent variables, risk perception and negative emotions toward COVID-19 as the mediator variables, and disease-preventive behaviours as the outcome variable. This proposed mediation chain rests on the theoretical assumptions that (1) conspiracy theories have an implication for people’s evaluation of risk associated with an entity (in this case, COVID-19/SARS-CoV-2), and (2) such evaluation influences people’s engagement in health-related behaviour. Past studies have offered initial support to these assumptions with experimental design (e.g., Jolley and Douglas, 2014; Sheeran et al., 2014). Additionally, it would be crucial to rule out alternative mechanisms and to control for potential confounding variables in the proposed mediation analysis. Therefore, we controlled for the covariates noted above, including institutional trust, political orientation, and demographic variables.
Last, we explored how the hypothesised relationship may vary across different stages of the COVID-19 outbreak. We compared the strength of the relationship by treating the stage of the outbreak as the moderator variable and testing its effect using multiple regression analysis. We coded the stage of the COVID-19 outbreak as a continuous variable (1 = Time 1 to 6 = Time 6). To facilitate the interpretation of the moderation effect, we standardised both the independent variables (i.e., the two types of conspiracy beliefs) and the moderator variable (i.e., stage) when computing the interaction terms (i.e., conspiracy beliefs × stage). We conducted two multiple regression analyses with risk perception and negative emotions as the respective outcome variables. We used the “ggplot” package of R to illustrate the bivariate relationship between the two types of conspiracy-theory beliefs and risk perception or negative emotions (see Supplementary Figs. 1 to 4). We further explored whether or not the indirect effects of conspiracy-theory beliefs via risk perception and negative emotions on disease-preventive behaviours would vary across stages by conducting a moderated mediation analysis with PROCESS (Hayes, 2013; see also Preacher et al., 2007).
Results
We summarise descriptive and reliability statistics of the key variables in Supplementary Table 2 and present the zero-order correlations among the key variables in Supplementary Table 3. Figures 1 and 2 illustrate the zero-order correlation between belief in the two types of COVID-19 conspiracy theories (risk acceptance and risk rejection) and disease-preventive behaviours across the six time-points. The correlation between belief in the risk-acceptance type of COVID-19 conspiracy theory and disease-preventive behaviours was 0.19 (N = 1508, p < 0.001) in the pooled sample and ranged between −0.09 (N = 251, p = 0.165; Time 6) and 0.28 (N = 253, p < 0.001; Time 3) across the six time-points. By contrast, the correlation between belief in the risk-rejection type of COVID-19 conspiracy theory and disease-preventive behaviours was −0.01 (N = 1508, p = 0.752) in the pooled sample and ranged between −0.15 (N = 251, p = 0.018; Time 6) and 0.12 (N = 254, p = 0.064; Time 2) across the six time-points, showing an opposite pattern from that of the risk-acceptance type.
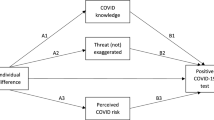
Next, we conducted a parallel mediation analysis to examine the indirect effects of the two independent variables (the two types of conspiracy-theory beliefs) via the two mediator variables (risk perception and negative emotions toward COVID-19) using PROCESS (Hayes, 2013). Figure 3 shows the key findings (see Supplementary Table 4 for the full results). As predicted, belief in the risk-acceptance type of COVID-19 conspiracy theory was positively related to risk perception and negative emotions toward COVID-19. The indirect effects of belief in the risk-acceptance type of COVID-19 conspiracy theory on disease-preventive behaviours via the two mediator variables were significant, as the bootstrapped 95% confidence interval did not contain zero (see the note of Fig. 3). These findings support Hypotheses 1a and 1b. By contrast, belief in the risk-rejection type of COVID-19 conspiracy theory was negatively related to risk perception and negative emotions toward COVID-19. The indirect effects of belief in the risk-rejection type of COVID-19 conspiracy theories were significant, as the bootstrapped 95% confidence interval did not contain zero (see the note in Fig. 3). These findings support Hypotheses 2a and 2b. Interestingly, we also found that institutional trust was unrelated to belief in the two types of COVID-19 conspiracy theories, although positively related to disease-preventive behaviour (see Supplementary Table 6).

Note. All pathways were significant at p < 0.001 level. Indirect effects of belief in the risk-acceptance type of COVID-19 conspiracy theory via risk perception (partial standardised indirect effect = 0.02, bootstrapped SE = 0.00, 95% CI = [0.02, 0.03]) and negative emotions toward COVID-19 (partial standardised indirect effect = 0.02, bootstrapped SE = 0.00, 95% CI = [0.02, 0.04]) were significant. Indirect effects of belief in the risk-rejection type of COVID-19 conspiracy theory via risk perception (partial standardised indirect effect = −0.02, bootstrapped SE = 0.00, 95% CI = [−0.02, −0.01]) and negative emotions toward COVID-19 (partial standardised indirect effect = −0.01, bootstrapped SE = 0.00, 95% CI = [−0.02, −0.01]) were significant. See Supplementary Table 4 for the detail of the results.
Next, we conducted a series of moderating analyses with the stage of the COVID-19 outbreak coded as a continuous variable (1 = Time 1 to 6 = Time 6). Supplementary Table 5 shows the full results. Supporting our classification, the stage of the COVID-19 outbreak was a positive and significant predictor of risk perception (b = 0.85, SE = 0.03, p < 0.001, 95% CI = [0.78, 0.91]) and negative emotions toward COVID-19 (b = 0.32, SE = 0.04, p < 0.001, 95% CI = [0.25, 0.39]). This indicates that people perceived the risk of COVID-19 to be more severe and felt more negative toward the virus/disease at the later time-points. This result is also consistent with the surge in the number of confirmed cases of COVID-19 since Time 4 (see Supplementary Table 1) and the official categorisation of COVID-19 as a pandemic by the World Health Organisation (WHO) on March 11, 2020 (one day before Time 5 data collection). In line with this, a public opinion poll conducted during March also revealed an increasing trend in Americans’ risk perception (YouGov, 2020a), reporting that the percentage of people who reported fear of being infected with COVID-19 had increased from 34% on March 2 to 60% on March 30. Furthermore, there was also an increasing trend in the adoption of disease-preventive behaviours in this period (e.g., improving personal hygiene, avoiding crowded places) (YouGov, 2020b). For example, the percentage of American respondents who reported that they had avoided crowded public places increased from 24% on March 2 to 77% on March 30. We also observed a similar trend in our data, in which outbreak stage was positively related to disease-preventive behaviour (r = 0.36, p < 0.001; see Supplementary Table 1). Overall, the consistency between our findings and the public opinion survey provides support that the differences observed between time-points did reflect the changes in people’s response to the COVID-19 outbreak.
We found that belief in the risk-acceptance type of COVID-19 conspiracy theory × stage of the outbreak interaction was negative and marginally significant in predicting risk perception (b = −0.07, SE = 0.04, p = 0.089, 95% CI = [−0.14, 0.01]) and negative and significant in predicting negative emotions toward COVID-19 (b = −0.12, SE = 0.04, p = 0.004, 95% CI = [−0.21, −0.04]). These findings suggest that the relationship between belief in risk-acceptance COVID-19 conspiracy theories and risk perception/negative emotions was stronger in the less-severe stage of the outbreak (though only marginally for risk perception), thereby supporting Hypothesis 3a. Also, belief in the risk-rejection type of COVID-19 conspiracy theories × stage of the COVID-19 outbreak interaction was negative and significant in predicting risk perception (b = −0.15, SE = 0.04, p < 0.001, 95% CI = [−0.22, −0.07]) but was negative and non-significant in predicting negative emotions toward COVID-19 (b = −0.01, SE = 0.04, p = 0.870, 95% CI = [−0.09, 0.08]). These findings suggest that the relationship between belief in risk-rejection COVID-19 conspiracy theories and risk perception—but not that between belief in risk-rejection conspiracy theories and negative emotions—was stronger in the more-severe stage of the outbreak, thereby partially supporting Hypothesis 3b.
Taken as a whole, these findings suggest that the two types of conspiracy theories may play a differential role in risk perception at mild versus severe stages of the outbreak. Figures 4 and 5 illustrate the strength of the associations between belief in the two types of COVID-19 conspiracy theories and the two mediator variables across the six time-points, respectively. As shown in these figures, and consistent with our predictions, the strength of the positive associations for the risk-acceptance type became weaker over time, whereas the strength of the negative associations for the risk-rejection type became more prominent at the later time-points. Supplementary Figs. 1 through 4 illustrate the scatterplots of the relationship between belief in the two types of COVID-19 conspiracy theories and the two mediators, respectively.

Note. Each bar shows the strength of partial correlation (r) with 95% confidence interval (CI).

Note. Each bar shows the strength of partial correlation (r) with 95% confidence interval (CI).
Finally, we explored whether or not the stage of the COVID-19 outbreak moderated the indirect effects of belief in the two types of conspiracy theories via risk perception and negative emotions toward COVID-19 on disease-preventive behaviours (Hypotheses 4a and 4b). We tested the indirect effects only for the significant moderation effect revealed above. As predicted, the indirect effects of belief in the risk-acceptance type of COVID-19 conspiracy theory via negative emotions toward COVID-19 was significantly higher in the less-severe than more-severe phases of the outbreak (moderated mediation index = −0.01, bootstrapped SE = 0.00, bootstrapped 95% CI = [−0.02, −0.00]). Also, as predicted, the indirect effect of belief in the risk-rejection type of COVID-19 conspiracy theory via risk perception was significantly lower in the less-severe than more-severe phases of the outbreak (moderated mediation index = −0.01, bootstrapped SE = 0.00, bootstrapped 95% CI = [−0.02, −0.00]).
Discussion
Overall, the findings reveal complex (not-so-straightforward) links between belief in COVID-19 conspiracy theories and self-reported disease-preventive behaviours; the links depend on the contents of the conspiracy theory and the context, i.e., the severity of the disease outbreak. Specifically, our findings revealed that belief in the risk-acceptance type of conspiracy theory was associated with higher risk perception and more negative feelings toward the COVID-19 outbreak, which in turn was linked to more engagement in disease-preventive behaviours. By contrast, belief in the risk-rejection type of conspiracy theory was associated with lower risk perception and less-negative emotions toward the outbreak, which in turn related to less engagement in disease-preventive behaviours. Interestingly, these two links appear to play out differently at different stages of the COVID-19 outbreak, such that the former link was stronger during the early, mild stage of the outbreak, whereas the latter link was stronger during the later, severe stage. This is probably because the risk-acceptance type of conspiracy theory reflected people’s awareness of threat and increased their negative feeling above the normative level when the outbreak was mild (early stage), whereas the risk-rejection type of conspiracy theory reflected people’s denial of threat and thus was linked with risk perception below the normative level when the outbreak was severe (later stage). These findings remained consistent after controlling for institutional trust, political orientation, and demographic variables.
Taken as a whole, our findings shed light on some new aspects that have not been well explored in the literature. First, our findings demonstrate that the different contents of conspiracy theories can have different, even opposite implications for people’s perceptions, feelings, and behaviours. In our case, we show that COVID-19 conspiracy theories relate to people’s implicit acceptance or denial of disease risk. As such, conspiracy theories can reflect people’s sense-making, i.e., how they understand the nature of the disease and/or the disease outbreak. This point was consistent with research studies that were conducted at the same time by Imhoff and Lamberty (2020), Oleksy et al. (2021), and Sternisko et al. (2020). Our findings replicate and extend past findings by probing into the mechanism underlying the differential impact of conspiracy-theory beliefs, specifically: The differential impacts of COVID-19 conspiracy-theory beliefs are linked to different levels of risk perception and negative emotion.
Second, we show how context is an integral factor in linking specific types of conspiracy theories and people’s perceptions, feelings, and behaviours. For instance, when the outbreak was not-so-severe (or the threat was still distant), believing in conspiracy theories that acknowledge the threat (risk-acceptance type) would relate to more precautious feeling (e.g., stronger negative emotions) and action (e.g., disease-preventive behaviour). Although this acceptance would relate to more negative emotions as well, it could save lives if the threat turned out to be deadly. By contrast, believing in conspiracy theories that deny the threat (risk-rejection type) could relate to lower risk perception and fewer precautions taken, which could lead to dire consequences in the case of a deadly disease outbreak. For example, denying the severity of the outbreak may fuel frustration toward constraining regulations and motivate protests against stay-at-home orders, mandatory closure of non-essential business, and/or mask-wearing recommendations/mandates.
Third, the impact of context (in this case, the actual severity of the COVID-19 outbreak) on the psychological and behavioural consequences of conspiracy beliefs has not been systematically studied by past research. For example, the aforementioned study by Imhoff and Lamberty (2020) was conducted in late March, at which time the outbreak had already hit the United States severely. Our findings thus add nuance to the literature by suggesting how the links between beliefs in different types of conspiracy-theory and outcome variables may change as a function of the outbreak’s progression. It is crucial for future studies to consider how these links vary across situations and contexts.
It is important to note that we do not mean to say that belief in risk-acceptance conspiracy theories is necessarily adaptive, because such belief may reflect a misattribution of the origin of the threat to outgroup or wrong sources. Accordingly, such conspiracy beliefs may relate to heightened hatred and hostility toward some groups of people. Anecdotes and news reports have suggested an anti-Chinese or even anti-Asian sentiment since the COVID-19 outbreak (for discussions, see Roberto et al., 2020; Shimizu, 2020). Indeed, the relationship between conspiracy beliefs and prejudice toward groups of people is well-documented in the literature (e.g., Imhoff and Bruder, 2014). Accordingly, it is crucial for future studies to not only examine whether belief in COVID-19 conspiracy theories leads to prejudice against certain groups of people, but also to identify ways to improve intergroup harmony in the aftermath of disease outbreaks.
There are several limitations in the current study. First, because the study used a repeated cross-sectional design, our findings are correlational in nature and we cannot discern causal relationships among belief in COVID-19 conspiracy theories and risk perception, negative emotions toward COVID-19, and disease-preventive behaviours. Moreover, because the participants were different at each time-point, we cannot exclude sampling differences as confounds. Nevertheless, the repeated cross-sectional design allowed us to observe how the natural change in the severity of COVID-19 relates to differences in belief of COVID-19 conspiracy theories, risk perception, negative emotions toward COVID-19, and disease-preventive behaviours across the six time-points. Our design offers preliminary support to the notion that changes in the actual severity of an outbreak are associated with changes in risk perception, negative emotions toward the disease, and engagement in disease-preventive behaviours (see Supplementary Table 3). This pattern is consistent with public opinion polls conducted in March (e.g., YouGov, 2020a, 2020b), in which there was an increasing trend in people’s perceived threat of COVID-19 and disease-preventive behaviours. However, we did not observe significant differences in the mean scores of the beliefs in the two types of COVID-19 conspiracy theories across different time-points (except for the risk-acceptance type of conspiracy theories in Time 6; see Supplementary Table 2). This observation is consistent with Romer and Jamieson (2020), in which they found that conspiracy beliefs related to COVID-19 were highly stable over a four-month period from March to July 2020. Future study can test the causal impact of conspiracy beliefs by manipulating conspiracy theories through presenting theories that support versus reject threatening events (like Jolley and Douglas, 2014, Study 2) and observing the consequences on risk perception, threat-related emotions, and disease-preventive behaviours.
The present research measured only self-reported disease-preventive behaviours. Participants may over-report or under-report their behaviours (e.g., due to bad memory or social-impression management). Future studies would benefit from using multiple methods to capture people’s engagement in disease-preventive behaviours (e.g., observer rating, observational study based on a lab experiment). Furthermore, the present research measured only some beliefs derived from the complex narratives pertaining to COVID-19 conspiracy theories. Since we began conducting the study in early February, the various narratives of COVID-19 conspiracy theories were not yet fully fledged (see Shahsavari et al., 2020). Future research can identify a more comprehensive set of conspiracy theories to examine how much people believe in them and how such beliefs influence people’s behaviours.
Data availability
The dataset analysed in the present study and the codes used to conduct the analyses are available in open science framework: https://osf.io/7xf4u
Notes
In our original questionnaire, we have included two additional items. The two items, however, did not contain all parts of a conspiracy theory as it is typically defined. The statement that “the novel coronavirus is a man-made virus that was created in a laboratory” did not explicitly name a conspirator; similarly, “the outbreak of the novel coronavirus is due to an accidental leakage that happened in a virology institute in Wuhan, China,” did not state a secret malicious intent. We thus removed these two items, when we computed the average score of the risk-acceptance conspiracy beliefs. To provide a conservative test, we have tested all hypotheses again by including the two items in question. All of our main findings remained consistent, except that the Stage x belief in risk-acceptance type of COVID-19 conspiracy theory interaction in predicting risk perception became significant (b = −0.08, SE = 0.04, p = 0.031, 95% CI = [−0.16, −0.01]). By including these two items, the construct may capture both belief in risk-acceptance conspiracy theories and COVID-19-related rumours. We thus opted to report the findings without the two items included. Nevertheless, these findings may point to the possibility to extend our hypothesised model into understanding the relationship between COVID-19-related unfounded beliefs and disease-preventive behaviour. Given that we only included two rumour-related items in this study, we refrained from drawing any further conclusion. We suggest future studies to further scrutinise this possibility by incorporating measures that capture a comprehensive set of unfounded beliefs.
We conducted a confirmatory factor analysis to validate the proposed two-factor structure with R. We included the five items of belief in the risk-acceptance type of conspiracy theory and the two items of belief in the risk-rejection type of conspiracy theory into the analysis. The model fit showed better model fit for a two-factor solution (CFI = 0.975, TLI = 0.952, RMSEA = 0.092, SRMR = 0.033, BIC = 46775.575, AIC = 46685.160) than for a one-factor solution (CFI = 0.961, TLI = 0.931, RMSEA = 0.109, SRMR = 0.095, BIC = 46845.953, AIC = 46760.857). This result suggests that it is appropriate to consider the two types of conspiracy beliefs as distinct constructs.
We noted that the internal reliability of the two risk-rejection conspiracy-theory items was relatively low; hence we performed additional analyses using only one core item: “In reality, the novel coronavirus is similar to influenza. It is just that some organisations and people purposefully exaggerate its severity.” All of our findings reported in the main text remained consistent even with this single item.
References
Calvillo DP, Ross BJ, Garcia RJB, Smelter TJ, Rutchick AM (2020) Political ideology predicts perceptions of the threat of COVID-19 (and susceptibility to fake news about it). Soc Psychol Pers Sci 11:1119–1128. https://doi.org/10.1177/1948550620940539
Chandran S, Menon G (2004) When a day means more than a year: effects of temporal framing on judgements of health risk. J Consum Res 31:375–389. https://doi.org/10.1086/422116
Curran PG (2016) Methods for the detection of carelessly invalid responses in survey data. J Exp Soc Psychol 66:4–19. https://doi.org/10.1016/j.jesp/2015.07.006
Douglas KM, Uscinski JE, Sutton RM, Cichocka A, Nefes T, Ang CS, Deravi F(2019) Understanding conspiracy theories Adv Political Psychol 40:3–35. https://doi.org/10.1111/pops.12568
Earnshaw VA, Bogart LM, Klompas M, Katz IT (2019) Medical mistrust in the context of Ebola: implications for intended care-seeking and quarantine policy support in the United States. J Health Psychol 24:219–228. https://doi.org/10.1177/1359105316650507
Georgiou N, Delfabbro P, Balzan R (2020) COVID-19-related conspiracy beliefs and their relationship with perceived stress and pre-existing conspiracy beliefs. Pers Individ Differ 166:110201. https://doi.org/10.1016/j.paid.2020.110201
Gonçalves-Sá J (2020) In the fight against the new coronavirus outbreak, we must also struggle with human bias. Nat Med 26:305–305. https://doi.org/10.1038/s41591-020-0802-y
Hayes AF (2013) Introduction to mediation, moderation, and conditional process analysis. The Guilford Press, New York, NY
Imhoff R, Bruder M (2014) Speaking (un-) truth to power: conspiracy mentality as a generalised political attitude. Eur J Pers 28:25–43. https://doi.org/10.1002/per.1930
Imhoff R, Lamberty P (2020) A bioweapon or a hoax? The link between distinct conspiracy beliefs about the coronavirus disease (COVID-19) outbreak and pandemic behavior. Soc Psychol Pers Sci 11:1110–1118. https://doi.org/10.1177/1948550620934692
Islam MS, Sarkar T, Khan SH, Mostofa Kamal AH, Hasan SM, Kabir A et al. (2020) COVID-19-related infodemic and its impact on public health: a global social media analysis. Am J Trop Med Hyg 103:1621–1629. https://doi.org/10.4269/ajtmh.20-0812
Johnson BB (2018) Residential location and psychological distance in Americans’ risk views and behavioral intentions regarding Zika virus. Risk Anal 38:2561–2579. https://doi.org/10.1111/risa.13184
Jolley D, Douglas KM (2014) The effects of anti-vaccine conspiracy theories on vaccination intentions. PLoS ONE 9:e89177. https://doi.org/10.1371/jounral.pone.0089177
Klofstad CA, Uscinski JE, Connolly JM, West JP (2019) What drives people to believe in Zika conspiracy theories? Palgrave Commun 5:1–8. https://doi.org/10.1057/s41599-019-0243-8
Law T (2020, September 21) COVID-19 conspiracy theories are spreading rapidly—and they’re a public health risk all their own. TIME. Retrieved from: https://time.com/5891333/covid-19-conspiracy-theories/
Litman L, Robinson J, Abberbock T (2017) TurkPrime.com: a versatile crowdsourcing data acquisition platform for the behavioral sciences. Behav Res Methods 49:433–442. https://doi.org/10.3758/s13428-016-0727-z
Noar SM, Zimmerman RS (2005) Health behavior theory and cumulative knowledge regarding health behaviors: are we moving in the right direction? Health Educ Res 20:275–290. https://doi.org/10.1093/her/cyg113
Oleksy T, Wnuk A, Maison D, Lys A (2021) Content matters. Different predictors and social consequences of general and government-related conspiracy theories on COVID-19. Pers Individ Differ 168:110289. https://doi.org/10.1016/j.paid.2020.110289
Piltch‐Loeb R, Zikmund‐Fisher BJ, Shaffer VA, Scherer LD, Knaus M, Fagerlin A et al. (2019) Cross‐sectional psychological and demographic associations of Zika knowledge and conspiracy beliefs before and after local Zika transmission. Risk Anal 39:2683–2693. https://doi.org/10.1111/risa.13369
Preacher KJ, Rucker DD, Hayes AF (2007) Addressing moderated mediation hypotheses: theory, methods, and prescriptions. Multivar Behav Res 42:185–227. https://doi.org/10.1080/00273170701341316
Roberto K, Johnson AF, Rauhaus BM (2020) Stigmatization and prejudice during the COVID-19 pandemic. Administrat Theory Praxis 43:364–378. https://doi.org/10.1080/10841806.2020.1782128. June
Romer D, Jamieson KH (2020) Conspiracy theories as barriers to controlling the spread of COVID-19 in the U.S. Soc Sci Med 263:113356. https://doi.org/10.1016/j.socscimed.2020.113356
Sell TK, Hosangadi D, Trotochaud M (2020) Misinformation and the U.S. Ebola communication crisis: analyzing the veracity and content of social media messages related to a fear-inducing infectious disease outbreak. BMC Public Health 20:1–10. https://doi.org/10.1186/s12889-020-08697-3
Shahsavari S, Holur P, Tangherlini TR, Roychowdhury V (2020) Conspiracy in the time of corona: automatic detection of COVID-19 conspiracy theories in social media and the news. J Comput Soc Sci. https://doi.org/10.1007/s42001-020-00086-5 1–39
Sheeran P, Harris PR, Epton T (2014) Does heightening risk appraisals change people’s intentions and behavior? A meta-analysis of experimental studies. Psychol Bull 140:511–543. https://doi.org/10.1037/a0033065
Shimizu K (2020) 2019-nCoV, fake news, and racism. Lancet 395:685–686. https://doi.org/10.1016/S0140-6736(20)30357-3
Sternisko A, Cichocka A, Cislak A, & Van Bavel JJ (2020) Collective narcissism predicts the belief and dissemination of conspiracy theories during the COVID-19 pandemic. Preprint at https://doi.org/10.31234/osf.io/4c6av
Uscinski JE (2018) The study of conspiracy theories. Argumenta 3:233–245. https://doi.org/10.23811/53.arg2017.use
Uscinski JE, Enders AM, Klofstad C, Seelig M, Funchion J, Everett C, Wuchty S et al. (2020) Why do people believe COVID-19 conspiracy theories?. The Harvard Kennedy School (HKS) Misinform Rev 1. https://doi.org/10.37016/mr-2020-015
van Prooijen JW, Van Vugt M (2018) Conspiracy theories: evolved functions and psychological mechanisms. Perspect Psychol Sci 13:770–788. https://doi.org/10.1177/1745691618774270
YouGov (2020a) YouGov COVID-19 tracker: fear of catching. Retrieved from: https://yougov.co.uk/topics/international/articles-reports/2020/03/17/fear-catching-covid-19
YouGov (2020b) YouGov COVID-19 tracker: personal measures taken to avoid COVID-19. Retrieved from: https://yougov.co.uk/topics/international/articles-reports/2020/03/17/personal-measures-taken-avoid-covid-19
Zwickle A, Wilson RS (2014) Construing risk: implications for risk communication. In: Arvai J, Rivers L (eds.) Effective risk communication. Routledge, New York, NY, pp. 190–203
Acknowledgements
We would like to thank Christa Schmidt for helping to identify COVID-19-related conspiracy theories and offering useful comments on the earlier version of the manuscript. This research is partially funded by a post-doctoral fellowship conferred to H-W Chan by the Research Committee of the Chinese University of Hong Kong, internal research grants by Beijing Normal University, China, and a General Research Fund (Ref No. 14621920) by Research Grant Council of Hong Kong SAR government awarded to Y Hong.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chan, HW., Chiu, C.PY., Zuo, S. et al. Not-so-straightforward links between believing in COVID-19-related conspiracy theories and engaging in disease-preventive behaviours. Humanit Soc Sci Commun 8, 104 (2021). https://doi.org/10.1057/s41599-021-00781-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1057/s41599-021-00781-2
This article is cited by
-
Conspiracy beliefs and COVID-19 guideline adherence in adolescent psychiatric outpatients: the predictive role of adverse childhood experiences
Child and Adolescent Psychiatry and Mental Health (2023)
-
Development and cross-national investigation of a model explaining participation in WHO-recommended and placebo behaviours to prevent COVID-19 infection
Scientific Reports (2022)
