
Abstract
Mounting evidence supports a potent inhibitory role of interleukin-10 (IL-10) in tumor carcinogenesis, angiogenesis and metastasis. This meta-analysis was designed to examine the association of three promoter polymorphisms (−592C > A, −819C > T and −1082G > A) in IL-10 gene with the risk for colorectal cancer and hepatocellular carcinoma. Qualification assessment and data collection were completed by two authors independently. The random-effects model using the DerSimonian and Laird method was fitted by the STATA software. Twenty-five articles involving 5933 cases and 9724 controls were meta-analyzed. Overall comparisons of the mutant alleles (−592A, −819T and −1082A) of three promoter polymorphisms with alternative wild alleles failed to reveal any statistical significance for both colorectal cancer and hepatocellular carcinoma (P > 0.05), and the likelihood of heterogeneity was low (I2 < 50%). For −592C > A polymorphism, a significant risk for colorectal cancer was identified when analysis was restricted to East Asians (odds ratio or OR = 1.41, 95% confidence interval or CI: 1.18–1.68, P < 0.001) and retrospective studies (OR = 1.23, 95% CI: 1.09–1.39, P = 0.001). As weighed by the Egger’s test and the fill-and-trim method, there was a low probability of publication bias for all studied polymorphisms. Our findings collectively suggest that the −592C > A polymorphism in IL-10 gene might be a susceptibility locus for colorectal cancer in East Asians.
Similar content being viewed by others


Introduction
Interleukin-10 (IL-10) is an anti-inflammatory and immune-suppressive cytokine1,2. Mounting evidence supports a potent inhibitory role of IL-10 in tumor carcinogenesis, angiogenesis and metastasis3. Lack of IL-10 in turn can trigger the production of pro-inflammatory cytokines, prevent anti-tumor immunity and promote tumor growth4. In humans, IL-10 is encoded by IL-10 gene on chromosome 1q31-q32 (gene ID: 3586), which comprises 5 exons and 4 introns. So far, there are 354 validated single nucleotide polymorphisms identified in IL-10 gene (http://www.ncbi.nlm.nih.gov/gene/3586). Human IL-10 in vivo is produced mainly by T-cells, B-cells, monocytes and macrophages, and its changes are under strong genetic control, with an estimated heritability of as high as 75%5. In view of above evidence, it would be tempting to speculate that IL-10 genetic alterations may contribute not only to circulating IL-10 variation but also to cancer susceptibility.
Of validated polymorphisms in IL-10 gene, three promoter polymorphisms including −592C > A (rs1800872), −819C > T (rs1800871) and −1082G > A (rs1800896) are well-defined and have been widely evaluated in predisposition to cancer at some sites6,7,8,9,10. Many studies that tested whether the polymorphisms in the promoter region of IL-10 gene are associated with hepatocellular carcinoma or colorectal cancer have shown controversial and inconclusive results8,11,12,13, at least in part because these studies are individually underpowered and involve different ethnic groups. Two previous meta-analyses have separately examined the association of these promoter polymorphisms with colorectal cancer and hepatocellular carcinoma14,15. Given accumulating data afterwards, we decided to conduct an updated meta-analysis on the association of three promoter polymorphisms in IL-10 gene with the risk of having colorectal cancer and hepatocellular carcinoma among 5933 cases and 9724 controls from 25 articles published in English.
Methods
Checklist
To improve the quality of a systematic review, this meta-analysis was conducted according to the statement put forward by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)16.
Search strategies
Potentially relevant articles were retrieved by searching Medline (PubMed), EMBASE (Excerpta Medica Database) and Web of Science using the following subject words: (interleukin-10 OR IL-10 OR IL 10) AND (colorectal cancer OR colon cancer OR rectal cancer OR hepatocellular carcinoma OR liver cancer) AND (allele OR genotype OR polymorphism OR variant OR mutation) as of January 1, 2016. All retrieved articles were managed by the EndNote X5 software (available at the website www.endnote.com, Thomson Reuters).
Qualification assessment
As a prerequisite, all potential articles must be published in English. In addition, articles were qualified if they simultaneously satisfied the following criteria: (1) clinical endpoint: colorectal cancer or hepatocellular carcinoma; (2) study design: retrospective or nested case-control design; (3) studied polymorphisms: at least one of the three promoter polymorphisms, −592C > A, −819C > T and −1082G > A, in IL-10 gene under investigation; (4) genetic data: the genotype or allele distributions of studied polymorphism(s) between cases and controls or the associated odds ratio (OR) and 95% confidence interval (CI). In case of duplicated publications from the same study group, article with a larger sample size was retained. Qualification assessment was completed independently by two investigators (Yan-Hui Shi and Chang-Zhu Lu), and if necessary a discussion was made over any uncertainties encountered.
Information collection
From each qualified article, the same two investigators (Yan-Hui Shi and Chang-Zhu Lu) collected and typed relevant information into a standardized Excel template, including the first author’s surname, publication year, the country where study subjects resided, race, cancer type, matched condition, source of controls, study design, sample size, age, gender, smoking, drinking and family history of cancer, hepatitis B virus (HBV) and hepatitis C virus (HCV), as well as the genotype or allele distributions of studied polymorphisms between cases and controls. Two independently-completed templates were cross-checked with inconsistencies solved by consensus. The detailed characteristics of all qualified articles are summarized in Table 1.
Statistical analysis
All statistical analyses are carried out with the STATA software for the Windows version 12.0 (StataCorp, College Station, Texas, USA). For all studied polymorphisms, deviation from the Hardy-Weinberg equilibrium for each polymorphism was assessed by the Chi-squared test or the Fisher’s exact test where appropriate in control groups at a significance level of 5%.
To statistically quantify the between-study heterogeneity, the inconsistency index (I2) is calculated, and it denotes the percent of observed diversity that is explained by heterogeneity rather than by chance. If the I2 is over 50% - a generally accepted cutoff value, it is indicative of significant heterogeneity. Individual effect-size estimates, ORs and its 95% CIs, were calculated under the fixed-effects model adopting the Mantel-Haenszel method17 when no significant heterogeneity was observed. Otherwise, the random-effects model adopting the DerSimonian and Laird method18 was used. In addition, to seek the clinical sources of heterogeneity, a set of stratified analyses by cancer type, race, matched condition, source of controls, study design and sample size were separately implemented. To avoid chance results, only subgroups involving 2 or more studies were analyzed. Moreover, a meta-regression analysis modeling age, gender, smoking, drinking and family history of cancer, HBV and HCV (HBV and HCV for hepatocellular carcinoma only) was conducted.
Influential analysis was conducted to see whether individual studies contribute significantly to pooled estimates by omitting each study one at a time sequentially.
Publication bias is a type of bias originating from the fact that studies with positive findings are more likely to be published than studies with negative findings, and its probability is weighted by the Egger’s linear regression test19 and the trim-and-fill method20. The trim-and-fill method is used to estimate the number of potential missing studies that might exist in a meta-analysis as presented by a filled funnel plot and the effect that these studies might have had on its effect-size estimate.
Results
Qualified articles
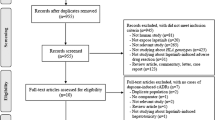
The selection process of qualified articles is charted in Fig. 1. The initial retrieval identified a total of 129 potentially relevant articles using ex-ante subject words. Finally, only 25 articles passed pre-defined qualification assessment,8,11,12,13,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41 and of them 15 used colorectal cancer (15 studies: 3938 cases and 6192 controls)8,11,23,26,27,29,30,31,32,33,35,36,37,40,41 and 10 used hepatocellular carcinoma (10 studies: 1995 cases and 3532 controls)10,11,18,19,21,22,25,31,35,36 as the clinical endpoint. For −592C > A, −819C > T and −1082G > A polymorphisms, there were respectively 11 and 7 studies, 3 and 5 studies, 11 and 6 studies for colorectal cancer and hepatocellular carcinoma.

The selection process of all qualified articles in this meta-analysis.
Baseline characteristics
Of 25 qualified studies, 12 were conducted in Caucasians, 10 in East Asians and 3 in mixed ethnicities. There were 14 studies having matched cases and controls, 3 studies unmatched and 8 studies unknown. Sixteen out of 25 studies enrolled controls from general populations and 9 from hospitals. Nineteen of 25 studies were retrospective case-control studies and 6 were nested case-control studies. TaqMan technique was the most widely adopted genotyping method (15 out of 25 studies). There were 17 studies with total sample size of 300 or more, and 8 studies of less than 300.
For both colorectal cancer and hepatocellular carcinoma, cases tended to be older (P = 0.022 and 0.028, respectively), male gender (P = 0.078 and 0.081, respectively) and smokers (P = 0.035 and 0.059) relative to controls. Moreover for hepatocellular carcinoma, the percentage of cases with HVB was exceedingly higher than that of controls (81.94% vs. 39.16%, P = 0.007).
Overall estimates
Given the small number of mutant homozygous genotypes of three studied polymorphisms, individual effect-size estimates were pooled only on the basis of both allelic and dominant models. Overall comparisons of the mutant alleles (−592A, −819T and −1082A) with the alternative wild alleles failed to reveal any statistical significance (P > 0.05) for both colorectal cancer and hepatocellular carcinoma under both allelic and dominant models (Figs 2, 3, 4), and there was no indication of between-study heterogeneity as measured by the I2 (<50%), except for the association of −592C > A polymorphism with colorectal cancer under the allelic model (I2 = 52.3%) and with hepatocellular carcinoma under the dominant model (I2 = 59.3%), as well as for the association of −891C > T polymorphism with colorectal cancer under both allelic (I2 = 72.0%) and dominant (I2 = 56.1%) models.

Forest plots of IL-10 gene −592C > A polymorphism with colorectal cancer and hepatocellular carcinoma under both allelic and dominant models.

Forest plots of IL-10 gene −819C > T polymorphism with colorectal cancer and hepatocellular carcinoma under both allelic and dominant models.

Forest plots of IL-10 gene −1082G > A polymorphism with colorectal cancer and hepatocellular carcinoma under both allelic and dominant models.
Stratified estimates
Considering the limited number of qualified studies for −819C > T polymorphism, the exploration of clinical heterogeneity by stratified analyses was only presented for −592C > A and −1082G > A polymorphisms under both allelic and dominant models (Tables 2 and 3). For −592C > A polymorphism, a significant increased risk for colorectal cancer was identified when analysis was restricted to East Asians under the allelic model (OR = 1.41, 95% CI: 1.18–1.68, P < 0.001) and to retrospective studies under both allelic (OR = 1.23, 95% CI: 1.09–1.39, P = 0.001) and dominant (OR = 1.21, 95% CI: 1.00–1.45, P = 0.047) models, and there was no evidence of significant heterogeneity. In contrast to hepatocellular carcinoma, there was no observable significance, except for a marginally significant association between −592C > A polymorphism and hepatocellular carcinoma in retrospective studies under the allelic model (OR = 0.90, 95% CI: 0.81–1.00, P = 0.051) and in studied with matched cases and controls under the dominant model (OR = 1.40, 95% CI: 1.00–1.97; P = 0.048). In addition, no statistical significance was noted in the other subgroups for −592C > A polymorphism and in all subgroups for −1082G > A polymorphism (P > 0.05).
Influential analysis
For three studied polymorphisms in IL-10 gene associated with colorectal cancer and hepatocellular carcinoma, influential analyses confirmed the overall changes in direction and magnitude under both allelic and dominant models.
Meta-regression analysis
By modeling age, gender, smoking, drinking and family history of cancer, HBV and HCV (HBV and HCV for hepatocellular carcinoma only), the meta-regression analyses failed to detect any positive signals for three studied polymorphisms in association with both colorectal cancer and hepatocellular carcinoma under both allelic and dominant models (Supplementary Table S1).
Publication bias
As weighed by the Egger’s test, there was a low probability of publication bias for three studied polymorphisms, except for −1082G > A polymorphism in association with hepatocellular carcinoma under the allelic model (Egger’s test: P = 0.042). As estimated by the trim-and-fill method, no missing studies were required to make the filled funnel plots symmetrical for three studied polymorphisms under both allelic (Fig. 5) and dominant (Fig. 6) models.

Filled funnel plots of the −592C > A, −819C > T and −1082G > A polymorphisms in IL-10 gene with colorectal cancer and hepatocellular carcinoma under the allelic model.

Filled funnel plots of the −592C > A, −819C > T and −1082G > A polymorphisms in IL-10 gene with colorectal cancer and hepatocellular carcinoma under the dominant model.
Discussion
Through a comprehensive meta-analysis of three promoter polymorphisms in IL-10 gene with colorectal cancer and hepatocellular carcinoma, we found that the −592C > A polymorphism might be a susceptibility locus for colorectal cancer in East Asians. Besides ethnic heterogeneity, study design might be another potential source of clinical heterogeneity for the association between −592C > A polymorphism and colorectal cancer. To our knowledge, this is so far the largest meta-analysis that has evaluated IL-10 gene multiple promoter polymorphisms with colorectal cancer and hepatocellular carcinoma risk.
Differing from the findings of previous meta-analysis by Zhang et al. who enrolled subjects of only Caucasian descent14, we observed a significant association of −592C > A polymorphism with colorectal cancer in East Asians rather than in Caucasians. One possible reason for this failed confirmation in Caucasians might be the enlarged sample size, as the contrast of 3938 cases and 6192 controls in the current meta-analysis with 1469 cases and 2566 controls in the meta-analysis by Zhang et al.14. Another possible reason might be the confounding impact of source of controls since after restricting analysis to population-based studies, significance was detected in the meta-analysis by Zhang et al.14 but not in the current meta-analysis. However, a note of caution should be sounded for the significant association of −592C > A polymorphism with colorectal cancer in East Asians in this study since only two studies are available for analysis11,41 and a possible chance of publication bias cannot be excluded, albeit no evidence of between-study heterogeneity observed. A large-scale study in East Asian populations is thereby required to confirm this preliminary finding.
Through exhaustive data explorations, there is no hint of significance for the association of three studied polymorphisms in IL-10 gene with hepatocellular carcinoma in this meta-analysis, inconsistent with the findings of the previous meta-analysis by Wei et al.15, as they observed a susceptible role of −592C > A polymorphism in hepatocellular carcinogenesis by pooling individual effect-size estimates of four Asian populations. In contrast to the 7 East Asian populations12,21,22,24,25,28,38,39 in this meta-analysis, our findings didn’t lend any credence to this susceptible role. Besides the enhanced statistical power in this meta-analysis, it might be the confounding impact of unaccounted heterogeneity in East Asians (I2 = 37.2% in contrast to 0.0% in Wei et al’s meta-analysis15). Moreover, as a corroboration of our negative findings, the association magnitude between −592C > A polymorphism and hepatocellular carcinoma risk was identical between the small and the large studies in our stratified analysis. Nevertheless, in spite of the negative findings in this study, it does not mean that the three studied polymorphisms in IL-10 gene are not biologically functional, and it is possible that the relative risk attributable to a single allele is small42. To yield statistically reliable evidence, further studies incorporating a wide range of candidate genes responsible for the development of hepatocellular carcinoma are required to get a clear picture of its underlying genetic architecture.
Finally, some possible limitations need to be acknowledged when interpreting and extrapolating our meta-analytical findings. First, our literature retrieval was only limited to articles published in English, and doing so might introduce a selection bias43. However, the Egger’s test and the filled funnel plots for three studied polymorphisms indicated no evidence of publication bias in this meta-analysis. Second, pooled analysis was only restricted to three promoter polymorphisms in IL-10 gene, and the other polymorphisms were not considered due to insufficient available data. Third, the only significant finding in this meta-analysis was based only on two eligible studies, leaving some room for further criticism. Fourth, all enrolled studies are case-control in design, which precluded the causality exploration. Fifth, only the risk of having colorectal cancer or hepatocellular carcinoma was treated as the clinical endpoint, and it is of interest to investigate whether the studied polymorphisms are associated with the recurrence and survival during subsequent medical therapies.
Taken together, we in an updated meta-analysis of three promoter polymorphisms in IL-10 gene found that the -592C > A polymorphism might be a susceptibility locus for colorectal cancer in East Asians. Considering the ubiquity of genetic heterogeneity and in view of small sample sizes involved, our findings should be considered to be preliminary until being replicated or confirmed in other larger, well-designed studies in future investigations.
Additional Information
How to cite this article: Shi, Y.-H. et al. The association of three promoter polymorphisms in interleukin-10 genewith the risk for colorectal cancer and hepatocellular carcinoma: A meta-analysis. Sci. Rep. 6, 30809; doi: 10.1038/srep30809 (2016).
References
Holland, G. & Zlotnik, A. Interleukin-10 and cancer. Cancer Invest 11, 751–758 (1993).
Barry, J. C. et al. Hyporesponsiveness to the anti-inflammatory action of interleukin-10 in type 2 diabetes. Sci Rep 6, 21244 (2016).
Tanikawa, T. et al. Interleukin-10 ablation promotes tumor development, growth, and metastasis. Cancer Res 72, 420–429 (2012).
Acuner-Ozbabacan, E. S. et al. The structural network of Interleukin-10 and its implications in inflammation and cancer. BMC Genomics 15 Suppl 4, S2 (2014).
Westendorp, R. G. et al. Genetic influence on cytokine production and fatal meningococcal disease. Lancet 349, 170–173 (1997).
Vinod, C. et al. A Common SNP of IL-10 (-1082A/G) is Associated With Increased Risk of Premenopausal Breast Cancer in South Indian Women. Iran J Cancer Prev 8, e3434 (2015).
Zidi, S. et al. IL-10 gene promoter and intron polymorphisms as genetic biomarkers of cervical cancer susceptibility among Tunisians. Cytokine 76, 343–347 (2015).
Miteva, L. D., Stanilov, N. S., Deliysky, T. S. & Stanilova, S. A. Significance of -1082A/G polymorphism of IL10 gene for progression of colorectal cancer and IL-10 expression. Tumour Biol 35, 12655–12664 (2014).
Li, C., Tong, W., Liu, B., Zhang, A. & Li, F. The -1082A>G polymorphism in promoter region of interleukin-10 and risk of digestive cancer: a meta-analysis. Sci Rep 4, 5335 (2014).
Niu, Y. M. et al. Increased risks between Interleukin-10 gene polymorphisms and haplotype and head and neck cancer: a meta-analysis. Sci Rep 5, 17149 (2015).
Yu, Y. et al. Polymorphisms of inflammation-related genes and colorectal cancer risk: a population-based case-control study in China. Int J Immunogenet 41, 289–297 (2014).
Li, Y. et al. Green tea consumption, inflammation and the risk of primary hepatocellular carcinoma in a Chinese population. Cancer Epidemiol 35, 362–368 (2011).
Ognjanovic, S., Yuan, J. M., Chaptman, A. K., Fan, Y. & Yu, M. C. Genetic polymorphisms in the cytokine genes and risk of hepatocellular carcinoma in low-risk non-Asians of USA. Carcinogenesis 30, 758–762 (2009).
Zhang, Y. M., Zhou, X. C., Xu, Z. & Tang, C. J. Meta-analysis of epidemiological studies of association of two polymorphisms in the interleukin-10 gene promoter and colorectal cancer risk. Genet Mol Res 11, 3389–3397 (2012).
Wei, Y. G. et al. Interleukin-10 gene polymorphisms and hepatocellular carcinoma susceptibility: a meta-analysis. World J Gastroenterol 17, 3941–3947 (2011).
Moher, D., Liberati, A., Tetzlaff, J. & Altman, D. G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6, e1000097 (2009).
Mantel, N. & Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 22, 719–748 (1959).
DerSimonian, R. & Laird, N. Meta-analysis in clinical trials. Control Clin Trials 7, 177–188 (1986).
Egger, M., Davey Smith, G., Schneider, M. & Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 315, 629–634 (1997).
Duval, S. & Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 56, 455–463 (2000).
Heneghan, M. A. et al. Frequency and nature of cytokine gene polymorphisms in hepatocellular carcinoma in Hong Kong Chinese. Int J Gastrointest Cancer 34, 19–26 (2003).
Shin, H. D. et al. Interleukin 10 haplotype associated with increased risk of hepatocellular carcinoma. Hum Mol Genet 12, 901–906 (2003).
Macarthur, M., Sharp, L., Hold, G. L., Little, J. & El-Omar, E. M. The role of cytokine gene polymorphisms in colorectal cancer and their interaction with aspirin use in the northeast of Scotland. Cancer Epidemiol Biomarkers Prev 14, 1613–1618 (2005).
Migita, K. et al. Cytokine gene polymorphisms in Japanese patients with hepatitis B virus infection–association between TGF-beta1 polymorphisms and hepatocellular carcinoma. J Hepatol 42, 505–510 (2005).
Nieters, A. et al. Effect of cytokine genotypes on the hepatitis B virus-hepatocellular carcinoma association. Cancer 103, 740–748 (2005).
Crivello, A. et al. Regulatory cytokine gene polymorphisms and risk of colorectal carcinoma. Ann N Y Acad Sci 1089, 98–103 (2006).
Gunter, M. J. et al. Inflammation-related gene polymorphisms and colorectal adenoma. Cancer Epidemiol Biomarkers Prev 15, 1126–1131 (2006).
Tseng, L. H. et al. Correlation of interleukin-10 gene haplotype with hepatocellular carcinoma in Taiwan. Tissue Antigens 67, 127–133 (2006).
Cozar, J. M. et al. High incidence of CTLA-4 AA (CT60) polymorphism in renal cell cancer. Hum Immunol 68, 698–704 (2007).
Talseth, B. A. et al. Lack of association between genetic polymorphisms in cytokine genes and disease expression in patients with hereditary non-polyposis colorectal cancer. Scand J Gastroenterol 42, 628–632 (2007).
Vogel, U. et al. Prospective study of interaction between alcohol, NSAID use and polymorphisms in genes involved in the inflammatory response in relation to risk of colorectal cancer. Mutat Res 624, 88–100 (2007).
Cacev, T., Radosevic, S., Krizanac, S. & Kapitanovic, S. Influence of interleukin-8 and interleukin-10 on sporadic colon cancer development and progression. Carcinogenesis 29, 1572–1580 (2008).
Wilkening, S. et al. Interleukin promoter polymorphisms and prognosis in colorectal cancer. Carcinogenesis 29, 1202–1206 (2008).
Bouzgarrou, N. et al. Combined analysis of interferon-gamma and interleukin-10 gene polymorphisms and chronic hepatitis C severity. Hum Immunol 70, 230–236 (2009).
Tsilidis, K. K. et al. Association of common polymorphisms in IL10, and in other genes related to inflammatory response and obesity with colorectal cancer. Cancer Causes Control 20, 1739–1751 (2009).
Andersen, V., Holst, R., Kopp, T. I., Tjonneland, A. & Vogel, U. Interactions between diet, lifestyle and IL10, IL1B, and PTGS2/COX-2 gene polymorphisms in relation to risk of colorectal cancer in a prospective Danish case-cohort study. PLoS One 8, e78366 (2013).
Burada, F. et al. Cytokine promoter polymorphisms and risk of colorectal cancer. Clin Lab 59, 773–779 (2013).
Bei, C. H. et al. Combined Effects of Six Cytokine Gene Polymorphisms and SNP-SNP Interactions on Hepatocellular Carcinoma Risk in Southern Guangxi, China. Asian Pac J Cancer Prev 15, 6961–6967 (2014).
Saxena, R., Chawla, Y. K., Verma, I. & Kaur, J. Association of interleukin-10 with hepatitis B virus (HBV) mediated disease progression in Indian population. Indian J Med Res 139, 737–745 (2014).
Basavaraju, U. et al. Cytokine gene polymorphisms, cytokine levels and the risk of colorectal neoplasia in a screened population of Northeast Scotland. Eur J Cancer Prev 24, 296–304 (2015).
Wang, N. et al. Multiple genetic variants are associated with colorectal cancer risk in the Han Chinese population. Eur J Cancer Prev 24, 1–5 (2015).
Wacholder, S., Rothman, N. & Caporaso, N. Population stratification in epidemiologic studies of common genetic variants and cancer: quantification of bias. J Natl Cancer Inst 92, 1151–1158 (2000).
Pei, Y., Xu, Y. & Niu, W. Causal relevance of circulating adiponectin with cancer: a meta-analysis implementing Mendelian randomization. Tumour Biol 36, 585–594 (2015).
Acknowledgements
This study received the grants from the Heilongjiang Provincial Education Office Scientific & Technologic Research Project (Grant No. 12541914) and the Scientific & Technologic Plan Project of Qiqihar City (Grant No. sfzd-2015109).
Author information
Authors and Affiliations
Contributions
Y.-H.S., C.-Z.L. and B.W. conceived and designed the study; Y.-H.S. and C.-Z.L. performed the study; Y.-H.S., Y.-F.W. and C.-Z.L. analyzed the data; Y.-F.W., B.-P.X., D.-N.J., D.-M.Z., M.-R.J., L.Z. and X.L. contributed materials/analysis tools; Y.-H.S., C.-Z.L. and B.W. wrote and revised the manuscript. All authors reviewed and approved the manuscript prior to submission.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Shi, YH., Zhao, DM., Wang, YF. et al. The association of three promoter polymorphisms in interleukin-10 gene with the risk for colorectal cancer and hepatocellular carcinoma: A meta-analysis. Sci Rep 6, 30809 (2016). https://doi.org/10.1038/srep30809
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep30809
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
