
Abstract
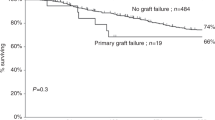
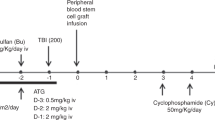
Twenty allogeneic bone marrow transplant patients were treated with an additional dose of donor cells (boost dose) for graft failure (n = 7), partial graft failure (n = 11) or extensive hemolysis caused by remaining recipient cells producing anti-erythrocyte antibodies (n = 2). Donors were in 12 cases HLA-identical siblings, three mismatched related donors and five unrelated donors. Cell source was in 13 cases bone marrow and in seven peripheral blood progenitor cells. Median time from BMT to booster dose was 3.4 months (range 0.7–59.3). Median infused cell dose was 2.4 × 108/kg patient (range 0.5–19.0). As GVHD prophylaxis most patients were already receiving different combinations of cyclosporine, prednisolone and methotrexate. No preparative treatment was given prior to boost in 16 patients; four received ATG. After boost, 11 patients developed acute GVHD, six grade I, four grade II and one grade III. Except for one patient, acute GVHD after boost was less, or the same grade as after BMT. Six patients developed chronic GVHD, three limited and three extensive. Five patients died within 30 days of the boost. Nine of 15 (60%) evaluable patients became transfusion independent within 30 days and three more within 60 days. Causes of death were: infections six (IP four, pneumonia two), relapse three; and GVHD three. Three out of five patients transplanted with unrelated marrow suffered from severe immunological reactions and died 2–3 months after the boost dose. Patient survival 1 and 3 years after boost was 55% and 43%, respectively. Among patients with hematological malignancies, leukemia-free survival at 3 years was 41%.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Remberger, M., Ringdén, O., Ljungman, P. et al. Booster marrow or blood cells for graft failure after allogeneic bone marrow transplantation. Bone Marrow Transplant 22, 73–78 (1998). https://doi.org/10.1038/sj.bmt.1701290
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1701290
Keywords
This article is cited by
-
Optimizing peripheral blood stem cells transplantation outcome through amend relapse and graft failure: a review of current literature
Experimental Hematology & Oncology (2017)
-
Successful early unmanipulated haploidentical transplantation with reduced-intensity conditioning for primary graft failure after cord blood transplantation in hematologic malignancy patients
Bone Marrow Transplantation (2015)
-
Poor graft function can be durably and safely improved by CD34+-selected stem cell boosts after allogeneic unrelated matched or mismatched hematopoietic cell transplantation
Journal of Cancer Research and Clinical Oncology (2015)
-
Treatment of poor graft function after allogeneic hematopoietic cell transplantation with a booster of CD34-selected cells infused without conditioning
Bone Marrow Transplantation (2014)
-
Salvage allogeneic hematopoietic SCT for primary graft failure in children
Bone Marrow Transplantation (2013)
