
Abstract
Mitochondrial DNA (mtDNA) content in ovarian carcinomas was assessed by quantitative PCR. Results show that mtDNA content in tumour cell was significantly higher than that in normal ovary. Change in mtDNA content was not related with patients' age or tumour stages. However, the average mtDNA copy number in pathological low-grade tumours was over two-fold higher than that in high-grade carcinomas (P=0.012). Moreover, type I carcinomas also had a significantly higher mtDNA copy number than in type II carcinomas (P=0.019). Change in mtDNA content might be an important genetic event in the progression of ovarian carcinomas.
Similar content being viewed by others


Main
Mitochondrion has its own genome, the mitochondrial DNA (mtDNA). Unlike nuclear genome, mtDNA exists in each cell with several hundreds to more than 10 000 copies. Generally, mtDNA content is tissue-specific and has a steady-state level in each type of tissue. Its maintenance depends mainly on nuclear-encoded factors which usually confers function through the Tfam pathway (Moraes, 2001). Mitochondrial DNA copy number in cell is not under stringent control; and various internal or external factors associated with ATP demand may influence its level, such as: exercise (Lim et al, 2000), hypoxia (Hoppeler et al, 2003), and steroid hormones stimulation (Weitzel et al, 2003). It is well known that carcinoma cells proliferate fast and survive in strict microenvironment, for example, under hypoxic condition. Either down- or upregulation of mtDNA content has been observed in a number of human malignancies (Jones et al, 2001; Simonnet et al, 2002; Lee et al, 2004; Wong et al, 2004). More importantly, mtDNA content change has also been found to be associated with histological types of gastric carcinoma (Wu et al, 2005).
In our previous studies, we have demonstrated the occurrence of high frequencies of somatic mtDNA mutations in endometrial (Liu et al, 2003) and ovarian carcinomas (Liu et al, 2001). In addition, we have also found that mtDNA copy number was significantly elevated in endometrial adenocarcinoma when compared with normal endometrial glandular epithelium (Wang et al, 2005). To further determine the mtDNA content change and its relationship with cancer, we therefore investigate the mtDNA copy number in primary ovarian carcinomas.
Materials and methods
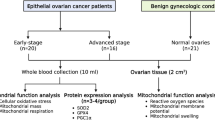
Frozen samples of 38 cases of primary epithelial ovarian carcinomas and four borderline ovarian tumours diagnosed and treated from January 1991 to December 2004 were retrieved without specific selection for this study. The mean age is 52 (ranging from 26 to 83). The clinical and pathologic characteristics of the 42 patients with ovarian carcinomas are shown in Table 1. In addition, frozen samples of 17 normal ovarian tissues were also used for this study. Use of clinical samples in this study was approved by the Ethics Committee of the University of Hong Kong.
In order to obtain pure tumour cell from cancerous tissues, laser capture microdissection (LCM) was employed. The LCM procedure and DNA isolation from LCM procured samples were previously described in detail (Wang et al, 2005). The recipes and conditions of quantitative PCR reaction were also described in our previous study (Wang et al, 2005).
The raw data were processed using the software accompanying the ABI PRISM 7700 Sequencing Detection System. Linear regression was used to analyse the response of Ct (the cycle number at which fluorescence raises above the baseline level during real-time quantitative PCR) vs the logarithm of the DNA concentration. Pearson's correlation was used to test the relationship between patients' age and mtDNA copy numbers in tumour tissues. The copy number comparison between groups was performed by nonparametric test (Mann–Whitney or Kruskal–Wallis test). Statistical significance was set at P<0.05.
Results
Table 1 shows the mtDNA copy number per cell of the 42 ovarian cancer samples and the 17 normal ovarian tissues. Mitochondrial DNA content is significantly higher in ovarian tumours than in normal ovarian tissues (P<0.001) (Figure 1A). The mtDNA copy numbers in tumour tissues have no relationship with patients' ages.

The comparisons of mtDNA copy number in cells among different groups of data. (A) The mean mtDNA copy number in normal ovarian cells (n=17) and ovarian carcinoma cells (n=42) are 929±276 and 3548±3421 copies per cell, respectively. A significant difference was detected (Mann–Whitney test, Z=−3.983, P<0.001). (B) The mtDNA copy number in normal ovarian cells was higher than that in normal endometrial cells (768±573, n=41) (Mann–Whitney test, Z=−2.332, P=0.020). (C) The mean mtDNA copy number in ovarian carcinoma cells (3548±3421, n=42) and endometrial carcinoma cells (2013±2317, n=65) were significantly different (Mann–Whitney test, Z=−3.311, P=0.001). (D) No significant difference of levels of mtDNA copy number between the early-stage tumour (3621±3974, n=20) and advanced stage tumour (3482±2923, n=22) was detected (Mann–Whitney test, Z=−0.327, P=0.743). (E) Significant difference of mtDNA copy number was observed between Grade 3 carcinomas (2361±1799, n=26) and the low-grade tumours (5877±4659, n=14) (Mann–Whitney test, Z=−2.495, P=0.012). (F) The mtDNA content in the type I tumours (4998±4279, n=19) was significantly higher than that in the type II tumours (2318±1930, n=21) (Mann–Whitney test, Z=−2.343, P=0.019).
The levels of mtDNA in normal ovary was higher than that in endometrium (Wang et al, 2005) (P=0.020) (Figure 1B). In ovarian tumours, an average of 3548±3421 copies of mtDNA was present in tumour cells. The highest and lowest copy numbers of mtDNA in cell were 16 772 and 444, respectively (Table 1). Compared with endometrial carcinomas (average mtDNA copy number=2012±2317 copies) (Wang et al, 2005), a significantly higher level of mtDNA copy number was found in ovarian carcinomas (P=0.001) (Figure 1C).
From the 42 patients, 20 were diagnosed as early-stage tumours, stage I or stage II; whereas 22 patients suffered from advanced carcinomas, stage III or stage IV. There is no significant difference of mtDNA copy numbers between the early-stage tumours (average at 3621±3974 copies per cell) and advanced stage carcinomas (average at 3482±2923 copies per cell) (Figure 1D).
As two patients were uninformative on the grading, the analysis was carried out in 40 patients. No significant difference was observed between the four borderline tumours and other invasive carcinomas (Mann–Whitney test, Z=−1.328, P=0.199). In the 26 cases of Grade 3 carcinomas, the mean value of mtDNA content in tumour cells was 2361±1799 copies. In the other 14 patients with lower-grade tumours (including the four borderline tumours), the mean copy of mtDNA molecules in each cell were 5877±4659 copies, it is over two-folds and significantly higher (P=0.012) than that in the higher-grade carcinomas (Figure 1E).
The mtDNA copy numbers among different histological subtypes of carcinomas was not significantly different (Kruskal–Wallis test, χ2=8.397, P=0.136, and df=5). Nevertheless, the mucinous tumours seem to have relatively higher level of mtDNA content than other subtypes. In the 42 cases, except two subjects of serous carcinoma uninformative on grading, 19 cases were classified as type I tumours and the other 21 cases were classified as type II tumour (for tumour classification, please see footnotes of Table 1). An average of 4998±4279 copies of mtDNA was detected in type I tumours; whereas, the mean copy number of mtDNA in type II tumours is 2318±1930. It is remarkable lower than that in the type I tumours (P=0.019) (Figure 1F).
Discussion
In this study, mtDNA content in ovarian carcinoma cells was found significantly higher than that in normal ovary. Except for a few reports, the change in mtDNA content does not associate with clinicopathological characteristics. Interestingly, in present study, we found that the mtDNA copy number in high-grade tumours is significantly lower than that in low-grade tumour. As the grade of tumour is a crucial prognostic factor, therefore, mtDNA content change might be an important genetic event in the progression of ovarian carcinoma.
Mitochondrial DNA copy number change was also found related with other human diseases. A significantly lower level of mtDNA content was observed in oocytes from women with ovarian insufficiency (May-Panloup et al, 2004). In addition, increased sperm mtDNA content was observed in male infertility (May-Panloup et al, 2003). The findings suggested that the change of mtDNA copy number was related with the impairment of cellular physiologic function. A probable explanation is that the change in mtDNA content would likely cause or be caused by the deficiencies in oxidative phosphorylation activity. Reactive oxygen species generation in mitochondria, which lead to DNA oxidative damage in cells, could thus impair cell function.
The significantly different levels of mtDNA content in different grades of tumour may be accounted for either by the downregulation in mtDNA replication in the high-grade tumours, or upregulation in mtDNA replication in low-grade tumours. Detection of many mtDNA alterations in the premalignant or preinvasive lesions indicated that mtDNA alterations could be an early genetic event in tumorigenesis (Chen et al, 2002; Ha et al, 2002; Durham et al, 2003). Mitochondrial DNA copy number was suggested to be increased by a feedback mechanism that compensates for the defective respiratory system owing to mutated mtDNA (Lee et al, 2000). So, it is possible that mtDNA copy number increased in early- and lower-grade malignancies.
On the other hand, long-term exposure to severe environmental insult such as hypoxia decreases the mitochondrial content of muscle fibres (Hoppeler et al, 2003). Undoubtedly, mitochondria are oxygen sensitive and the mtDNA content decrease might account for hypoxia. So, an alternative explanation of the decrease of mtDNA copy number in high-grade tumour is due to the fact that such tumour has rapid proliferation rate, and thus, survives in more severe hypoxia microenvironment leading to the downregulation of the mtDNA replication.
The most important finding in this study is the association between decreased mtDNA copy number with high grade and histological subtype of ovarian carcinoma. The histopathological phenotypes of ovarian carcinoma are complex. The epithelial-derived tumours including serous, mucinous, endometrioid, clear cell, transitional, squamous, mixed, and undifferentiated types comprise the majority of malignant tumours. Each of these histological subtypes is associated with distinct molecular genetic alterations (Shih Ie and Kurman, 2004; Bell, 2005). Based on recent clinicopathological and molecular studies, it has been proposed that surface epithelial tumours could be divided into two broad categories, type I and type II tumours. Mutations in KRAS and BRAF have been found to be common in low-grade serous and mucinous ovarian carcinomas (Gemignani et al, 2003; Sieben et al, 2004). KRAS belongs to RAS families which coding proto-oncogene that functions as a relay switch that transduces various growth signals in the cell surface to the nucleus through activation of the RAS–RAF–MEK–ERK–MAP kinase signalling pathway. Till now, no report connected the regulation of mtDNA replication with the genetic alterations in RAS–RAF pathway. As shown above, type I tumour had a significantly higher mtDNA copy number than that in type II tumour. So, whether or not a potential relationship between the genetic alterations in RAS–RAF pathway and mtDNA content change would be an interesting field to be explored.
On the other hand, mutations in the tumour suppressor molecule p53 were detected in type II tumours frequently (Shih Ie and Kurman, 2004). Recent studies provided the potential mechanistic explanation. p53 binding sequence was identified in mtDNA suggested that p53 might be involved in the regulation of mitochondrial transcription and replication (Heyne et al, 2004). In addition, p53 might also enhance the DNA replication function of mtDNA polymerase γ through their interaction. So, the loss of p53 owing to the mutations in the type II tumours could result in the decrease of mtDNA replication (Achanta et al, 2005).
Taken together, the finding of grade and histological associated change in mtDNA copy number provide a novel insight of the role of mtDNA alterations in cancer progression. Mitochondrial DNA content in cell may be potentially used as a tool to predict prognosis. Mechanisms of mtDNA maintenance in carcinoma cells warrant further investigation.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Achanta G, Sasaki R, Feng L, Carew JS, Lu W, Pelicano H, Keating MJ, Huang P. (2005) Novel role of p53 in maintaining mitochondrial genetic stability through interaction with DNA Pol gamma. EMBO J 24: 3482–3492
Bell DA (2005) Origins and molecular pathology of ovarian cancer. Mod Pathol 18(Suppl 2): S19–32
Chen JZ, Gokden N, Greene GF, Mukunyadzi P, Kadlubar FF (2002) Extensive somatic mitochondrial mutations in primary prostate cancer using laser capture microdissection. Cancer Res 62: 6470–6474
Durham SE, Krishnan KJ, Betts J, Birch-Machin MA (2003) Mitochondrial DNA damage in non-melanoma skin cancer. Br J Cancer 88: 90–95
Gemignani ML, Schlaerth AC, Bogomolniy F, Barakat RR, Lin O, Soslow R, Venkatraman E, Boyd J (2003) Role of KRAS and BRAF gene mutations in mucinous ovarian carcinoma. Gynecol Oncol 90: 378–381
Ha PK, Tong BC, Westra WH, Sanchez-Cespedes M, Parrella P, Zahurak M, Sidransky D, Califano JA (2002) Mitochondrial C-tract alteration in premalignant lesions of the head and neck: a marker for progression and clonal proliferation. Clin Cancer Res 8: 2260–2265
Heyne K, Mannebach S, Wuertz E, Knaup KX, Mahyar-Roemer M, Roemer K (2004) Identification of a putative p53 binding sequence within the human mitochondrial genome. FEBS Lett 578: 198–202
Hoppeler H, Vogt M, Weibel ER, Fluck M (2003) Response of skeletal muscle mitochondria to hypoxia. Exp Physiol 88: 109–119
Jones JB, Song JJ, Hempen PM, Parmigiani G, Hruban RH, Kern SE (2001) Detection of mitochondrial DNA mutations in pancreatic cancer offers a “mass”-ive advantage over detection of nuclear DNA mutations. Cancer Res 61: 1299–1304
Lee HC, Li SH, Lin JC, Wu CC, Yeh DC, Wei YH (2004) Somatic mutations in the D-loop and decrease in the copy number of mitochondrial DNA in human hepatocellular carcinoma. Mutat Res 547: 71–78
Lee HC, Yin PH, Lu CY, Chi CW, Wei YH (2000) Increase of mitochondria and mitochondrial DNA in response to oxidative stress in human cells. Biochem J 348(Part 2): 425–432
Lim S, Kim SK, Park KS, Kim SY, Cho BY, Yim MJ, Lee HK (2000) Effect of exercise on the mitochondrial DNA content of peripheral blood in healthy women. Eur J Appl Physiol 82: 407–412
Liu VW, Shi HH, Cheung AN, Chiu PM, Leung TW, Nagley P, Wong LC, Ngan HY (2001) High incidence of somatic mitochondrial DNA mutations in human ovarian carcinomas. Cancer Res 61: 5998–6001
Liu VW, Yang HJ, Wang Y, Tsang PC, Cheung AN, Chiu PM, Ng TY, Wong LC, Nagley P, Ngan HY (2003) High frequency of mitochondrial genome instability in human endometrial carcinomas. Br J Cancer 89: 697–701
May-Panloup P, Chretien MF, Jacques C, Vasseur C, Malthiery Y, Reynier P (2004) Low oocyte mitochondrial DNA content in ovarian insufficiency. Hum Reprod 20: 593–597
May-Panloup P, Chretien MF, Savagner F, Vasseur C, Jean M, Malthiery Y, Reynier P (2003) Increased sperm mitochondrial DNA content in male infertility. Hum Reprod 18: 550–556
Moraes CT (2001) What regulates mitochondrial DNA copy number in animal cells? Trends Genet 17: 199–205
Shih Ie M, Kurman RJ (2004) Ovarian tumorigenesis: a proposed model based on morphological and molecular genetic analysis. Am J Pathol 164: 1511–1518
Sieben NL, Macropoulos P, Roemen GM, Kolkman-Uljee SM, Jan Fleuren G, Houmadi R, Diss T, Warren B, Al Adnani M, De Goeij AP, Krausz T, Flanagan AM (2004) In ovarian neoplasms, BRAF, but not KRAS, mutations are restricted to low-grade serous tumours. J Pathol 202: 336–340
Simonnet H, Alazard N, Pfeiffer K, Gallou C, Beroud C, Demont J, Bouvier R, Schagger H, Godinot C (2002) Low mitochondrial respiratory chain content correlates with tumor aggressiveness in renal cell carcinoma. Carcinogenesis 23: 759–768
Wang Y, Liu VW, Xue WC, Tsang PC, Cheung AN, Ngan HY (2005) The increase of mitochondrial DNA content in endometrial adenocarcinoma cells: A quantitative study using laser-captured microdissected tissues. Gynecol Oncol 98: 104–110
Weitzel JM, Iwen KA, Seitz HJ (2003) Regulation of mitochondrial biogenesis by thyroid hormone. Exp Physiol 88: 121–128
Wong L-JC, Tan D-J, Bai R-K, Yeh K-T, Chang J (2004) Molecular alterations in mitochondrial DNA of hepatocellular carcinomas: is there a correlation with clinicopathological profile? J Med Genet 41: e65
Wu CW, Yin PH, Hung WY, Li AF, Li SH, Chi CW, Wei YH, Lee HC (2005) Mitochondrial DNA mutations and mitochondrial DNA depletion in gastric cancer. Genes Chromosomes Cancer 44: 19–28
Acknowledgements
This work was supported by University of Hong Kong Conference and Research Grant (10205029).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Wang, Y., Liu, V., Xue, W. et al. Association of decreased mitochondrial DNA content with ovarian cancer progression. Br J Cancer 95, 1087–1091 (2006). https://doi.org/10.1038/sj.bjc.6603377
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6603377
Keywords
This article is cited by
-
Ovarian cancer cells regulate their mitochondrial content and high mitochondrial content is associated with a poor prognosis
BMC Cancer (2024)
-
Mitochondrial DNA abnormalities provide mechanistic insight and predict reactive oxygen species-stimulating drug efficacy
BMC Cancer (2021)
-
EGFR-upregulated LIFR promotes SUCLG2-dependent castration resistance and neuroendocrine differentiation of prostate cancer
Oncogene (2020)
-
Mitochondrial DNA alterations may influence the cisplatin responsiveness of oral squamous cell carcinoma
Scientific Reports (2020)
-
Reversing wrinkled skin and hair loss in mice by restoring mitochondrial function
Cell Death & Disease (2018)
