
Abstract
Renal pathophysiology is elicited by activation of angiotensin II type 1 (AT1) receptors at all stages of renovascular disease. Angiotensin receptor blockers (ARBs) that specifically block the AT1 receptor offer the potential to prevent or delay progression to end-stage renal disease independently of reductions in blood pressure. Proteinuria—an early and sensitive marker for progressive renal dysfunction—is reduced by ARB use in patients with type 2 diabetic nephropathy and microalbuminuria or macroalbuminuria. Retrospective analysis of data available from early trials has confirmed this finding and has shown that albuminuria reduction is associated with lessening of cardiovascular risk. The ARB telmisartan is equivalent to enalapril in preventing glomerular filtration rate decline, and equivalent to valsartan in reducing proteinuria. Telmisartan is more effective than conventional therapy in lowering the risk of transition to overt nephropathy in hypertensive and normotensive patients. An additive effect has been seen in smaller studies when telmisartan has been added to lisinopril therapy, and high-dose telmisartan reduces albuminuria better than low-dose telmisartan. Similar data were obtained with other ARBs such as candesartan, losartan, valsartan, or irbesartan. These data support the proposition that blockade of the renin–angiotensin system beyond that required for maximum blood pressure reduction provides optimum renal protection.
Key Points
-
Injury to the vascular endothelium and glomerulus can be promoted by an activated renin–angiotensin system and, therefore, inhibition of this system provides renoprotection
-
RAS inhibition reduces proteinuria, which is a key factor in the progression of renal disease
-
Blood pressure control is essential to prevent progression to end-stage renal disease, but because the mechanisms of angiotensin receptor blockers and angiotensin-converting-enzyme inhibitors differ, the effectiveness of the latter might decline over time
-
Combination therapy with angiotensin receptor blockers and angiotensin-converting-enzyme inhibitors seems to produce additional blood-pressure-lowering effects to monotherapy
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
Ruggenenti P et al. (1998). Urinary protein excretion rate is the best independent predictor of ESRF in non-diabetic proteinuric chronic nephropathies. “Gruppo Italiano di Studi Epidemiologici in Nefrologia” (GISEN). Kidney Int 53: 1209–1216
Brewster UC and Perazella MA (2004) The renin-angiotensin-aldosterone system and the kidney: effects on kidney disease. Am J Med 116: 263–272
European Society of Hypertension-European Society of Cardiology Guidelines Committee (2003) 2003 European Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertension. J Hypertens 21: 1011–1053
Whitworth JA (2003) 2003 World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. J Hypertens 21: 1983–1992
Zidek W et al. (2003) New recommendations of the German Hypertension League for the drug treatment of hypertension. Dtsch Med Wochenschr 128: 2468–2469
Dzau V and Braunwald E (1991) Resolved and unresolved issues in the prevention and treatment of coronary artery disease: a workshop consensus statement. Am Heart J 121: 1244–1263
Hurairah H and Ferro A (2004) The role of the endothelium in the control of vascular function. Int J Clin Pract 58: 173–183
Hollenberg NK et al. (1998) Pathways for angiotensin II generation in intact human tissue: evidence from comparative pharmacological interruption of the renin system. Hypertension 32: 387–392
Sica DA (2003) Combination angiotensin-converting enzyme inhibitor and angiotensin receptor blocker therapy: its role in clinical practice. J Clin Hypertens (Greenwich) 5: 414–420
Brenner BM (2003) AMGEN International Prize: The history and future of renoprotection. Kidney Int 64: 1163–1168
Heart Outcomes Prevention Evaluation (HOPE) Study Investigators (2000) Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Lancet 355: 253–259
Lewis EJ et al. (1993) The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. N Engl J Med 329: 1456–1462
The GISEN Group (Gruppo Italiano di Studi Epidemiologici in Nefrologia) (1997) Randomised placebo-controlled trial of effect of ramipril on decline in glomerular filtration rate and risk of terminal renal failure in proteinuric, non-diabetic nephropathy. Lancet 349: 1857–1863
Maschio G et al. (1996) Effect of the angiotensin-converting-enzyme inhibitor benazepril on the progression of chronic renal insufficiency. The Angiotensin-Converting-Enzyme Inhibition in Progressive Renal Insufficiency Study Group. N Engl J Med 334: 939–945
Kidney Disease Outcomes Quality Initiative (K/DOQI) (2004) K/DOQI clinical practice guidelines on hypertension and antihypertensive agents in chronic kidney disease. Am J Kidney Dis 43 (Suppl 1): S1–S290
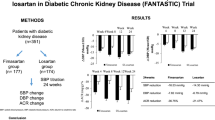
Brenner BM et al. (2001) Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 345: 861–869
Remuzzi G et al. (2004) Continuum of renoprotection with losartan at all stages of type 2 diabetic nephropathy: a post hoc analysis of the RENAAL trial results. J Am Soc Nephrol 15: 3117–3125
Lewis EJ et al. (2001) Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med 345: 851–860
American Diabetes Association (2002) Standards of medical care for patients with diabetes mellitus. Diabetes Care 25: 213–229
American Diabetes Association (2006) Standards of medical care in diabetes-2006. Diabetes Care 29 (Suppl 1): S4–S42
Pohl MA et al. (2005) Independent and additive impact of blood pressure control and angiotensin II receptor blockade on renal outcomes in the irbesartan diabetic nephropathy trial: clinical implications and limitations. J Am Soc Nephrol 16: 3027–3037
Gall MA et al. (1997) Risk factors for development of incipient and overt diabetic nephropathy in patients with non-insulin dependent diabetes mellitus: prospective, observational study. BMJ 314: 783–788
Ibrahim HA et al. (2004) Relations between von Willebrand factor, markers of oxidative stress and microalbuminuria in patients with type 2 diabetes mellitus. Med Sci Monit 10: CR85–CR89
Leoncini G et al. (2002) Microalbuminuria is an integrated marker of subclinical organ damage in primary hypertension. J Hum Hypertens 16: 399–404
Wachtell K et al. (2003) Albuminuria and cardiovascular risk in hypertensive patients with left ventricular hypertrophy: the LIFE study. Ann Intern Med 139: 901–906
Parving HH et al. (2001) The effect of irbesartan on the development of diabetic nephropathy in patients with type 2 diabetes. N Engl J Med 345: 870–878
Viberti G and Wheeldon NM (2002) Microalbuminuria reduction with valsartan in patients with type 2 diabetes mellitus: a blood pressure-independent effect. Circulation 106: 672–678
Ibsen H et al. (2005) Reduction in albuminuria translates to reduction in cardiovascular events in hypertensive patients: losartan intervention for endpoint reduction in hypertension study. Hypertension 45: 198–202
Dahlöf B et al. (2002) Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet 359: 995–1003
Battershill AJ and Scott LJ (2006) Telmisartan: a review of its use in the management of hypertension. Drugs 66: 51–83
Makino H et al. (2005) The telmisartan renoprotective study from incipient nephropathy to overt nephropathy—rationale, study design, treatment plan and baseline characteristics of the incipient to overt: angiotensin II receptor blocker, telmisartan, Investigation on Type 2 Diabetic Nephropathy (INNOVATION) Study. J Int Med Res 33: 677–686
Barnett AH et al. (2004) Angiotensin-receptor blockade versus converting-enzyme inhibition in type 2 diabetes and nephropathy. N Engl J Med 351: 1952–1961
Schmieder RE et al. (2005) Effects of telmisartan versus ramipril on endothelium function of the renal vasculature in type 2 diabetes. J Hypertens 23 (Suppl): S147
Ravid M et al. (1998) Use of enalapril to attenuate decline in renal function in normotensive, normoalbuminuric patients with type 2 diabetes mellitus. A randomized, controlled trial. Ann Intern Med 128: 982–988
Parving HH et al. (2004) Angiotensin receptor blockers in diabetic nephropathy: renal and cardiovascular end points. Semin Nephrol 24: 147–157
National Kidney Foundation (2002) K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 39 (Suppl 1): S1–S266
Valmadrid CT et al. (2000) The risk of cardiovascular disease mortality associated with microalbuminuria and gross proteinuria in persons with older-onset diabetes mellitus. Arch Intern Med 160: 1093–1100
Barnett AH (2005) Preventing renal complications in diabetic patients: the Diabetics Exposed to Telmisartan And enalaprIL (DETAIL) study. Acta Diabetol 42 (Suppl 1): S42–S49
Weber M (2003) The telmisartan Programme of Research tO show Telmisartan End-organ proteCTION (PROTECTION) programme. J Hypertens 21 (Suppl): S37–S46
Aranda P et al. (2005) Long-term renoprotective effects of standard versus high doses of telmisartan in hypertensive nondiabetic nephropathies. Am J Kidney Dis 46: 1074–1079
Wolf G and Ritz E (2005) Combination therapy with ACE inhibitors and angiotensin II receptor blockers to halt progression of chronic renal disease: pathophysiology and indications. Kidney Int 67: 799–812
MacKinnon M et al. (2006) Combination therapy with an angiotensin receptor blocker and an ACE inhibitor in proteinuric renal disease: a systematic review of the efficacy and safety data. Am J Kidney Dis 48: 8–20
Sengul AM et al. (2006) Beneficial effect of lisinopril plus telmisartan in patients with type 2 diabetes, microalbuminuria and hypertension. Diabetes Res Clin Pract 71: 210–219
Acknowledgements
PAREXEL MMS provided writing assistance, comprising preparation of a draft from slides and audio transcript, preparation of figures and obtaining copyright permissions, proofreading, and reference checking.
Author information
Authors and Affiliations
Ethics declarations
Competing interests
The author declares no competing financial interests.
Rights and permissions
About this article
Cite this article
Galle, J. Reduction of proteinuria with angiotensin receptor blockers. Nat Rev Cardiol 5 (Suppl 1), S36–S43 (2008). https://doi.org/10.1038/ncpcardio0806
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1038/ncpcardio0806
This article is cited by
-
Continuous hypergammaglobulinemia and proteinuria after the recovery of the visceral Leishmaniasis: a case report
BMC Infectious Diseases (2021)
-
Exercise-induced albuminuria increases over time in individuals with impaired glucose metabolism
Cardiovascular Diabetology (2020)
-
Proteomic urinary biomarker approach in renal disease: from discovery to implementation
Pediatric Nephrology (2015)
-
Impaired endocytosis in proximal tubule from subchronic exposure to cadmium involves angiotensin II type 1 and cubilin receptors
BMC Nephrology (2013)
-
The angiotensin II type 1 receptor blocker olmesartan preferentially improves nocturnal hypertension and proteinuria in chronic kidney disease
Hypertension Research (2013)
