
Abstract
Background:
Obesity is associated with increased risk of chronic kidney disease and albuminuria is a predictor of renal impairment. Bariatric surgery reduces body weight in obese subjects, but it is not known whether surgery can prevent development of albuminuria. This study aims to determine the long-term effect of bariatric surgery on the incidence of albuminuria.
Subjects:
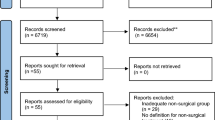
The Swedish Obese Subjects study is a non-randomized, prospective, controlled study conducted at 25 public surgical departments and 480 primary health care centers in Sweden. Between 1 September 1987 and 31 January 2001, 2010 participants who underwent bariatric surgery and 2037 controls were recruited. Inclusion criteria were age 37–60 years and BMI⩾34 in men and BMI⩾38 in women. In this analysis, we included 1498 patients in the surgery group and 1610 controls without albuminuria at baseline. Patients in the bariatric surgery group underwent banding (18%), vertical banded gastroplasty (69%) or gastric bypass (13%); controls received usual obesity care. Date of analysis was 1 January 2011. Median follow-up was 10 years, and the rates of follow-up were 87%, 74 and 52% at 2, 10 and 15 years, respectively. The main outcome of this report is incidence of albuminuria (defined as urinary albumin excretion >30 mg per 24 h) over up to 15 years.
Results:
During the follow-up, albuminuria developed in 246 participants in the control group and in 126 in the bariatric surgery group, corresponding to incidence rates of 20.4 and 9.4 per 1000 person years, respectively (adjusted hazard ratio, 0.37; 95% confidence interval, 0.30–0.47; P<0.001). The expected number of surgeries needed to prevent the development of albuminuria in one patient at 10 years was nine.
Conclusions:
Bariatric surgery is associated with reduced incidence of albuminuria compared with usual obesity care.
Similar content being viewed by others


Introduction
The prevalence of obesity has increased dramatically over recent decades and approximately one-third of the adult population of the United States today are obese.1 It is well established that obesity is associated with an increased risk of type 2 diabetes, hypertension and cardiovascular disease,2, 3, 4, 5 all of which may be involved in the etiology of chronic kidney disease. In addition, there is increasing evidence that obesity is an independent risk factor for chronic kidney disease.6,7
Albuminuria is a well-accepted predictor of chronic kidney disease8,9 and the prevalence of albuminuria is increased in obese individuals.10,11 One suggested link between obesity and albuminuria is increased intraabdominal pressure caused by increased amounts of visceral adipose tissue, resulting in venous stasis of the kidneys.12, 13, 14 Lifestyle changes that reduce body weight are known to reduce albuminuria.15 Bariatric surgery is the most effective treatment to achieve and maintain weight loss in severely obese patients,16 and previous studies indicate that weight-loss surgery also reduces the prevalence of albuminuria.17, 18, 19, 20, 21, 22 In a small study by Iaconelli et al.,17 seven patients with microalbuminuria at baseline had recovered from albuminuria and 15 patients remained free from albuminuria 10 years after biliopancreatic diversion, whereas the prevalence of albuminuria had increased in the non-surgical control group. However, there are no reports that specifically examine the long-term effect of bariatric surgery on the prevention of albuminuria in obese individuals without albuminuria at baseline.
The SOS study is a non-randomized, prospective, controlled, intervention trial that compares the long-term effects of bariatric surgery and usual care in obese subjects. We have previously reported positive effects of bariatric surgery on overall mortality (the predefined primary endpoint of the SOS study), cardiovascular disease and diabetes (predefined secondary endpoints).16,23, 24, 25 Although albuminuria was not a predefined endpoint in SOS, all data were collected prospectively, and we here report the long-term effects of bariatric surgery on albuminuria incidence.
Subjects and methods
Study design
The SOS study is a prospective, controlled intervention study conducted at 25 public surgical departments and 480 primary health care centers in Sweden. The design has been previously described.16,26 In brief, 2010 participants who underwent bariatric surgery and 2037 controls, were recruited between 1 September 1987 and 31 January 2001. Inclusion criteria were age between 37 and 60 years and body mass index (BMI) of 34 kg m2 or more for men and 38 kg m2 or more for women. The exclusion criteria were the same in both groups and designed to obtain an operable surgery group.
For the current analysis, SOS study participants were excluded from if they had albuminuria at baseline (n=811), if baseline information on diabetes or hypertension status (n=12), urine sample (n=31) or urinary albumin concentration (n=8) were not available or if urine collection time was shorter than 20 h (n=77). The current analysis therefore includes 1498 patients who underwent bariatric surgery and 1610 controls (Table 1). Participants in the surgery group underwent nonadjustable or adjustable banding (18%), vertical banded gastroplasty (69%) or gastric bypass (13%). The participants in the control group were given conventional non-surgical treatment for obesity at their primary health care centers. No attempt was made to standardize the non-surgical treatment.
Data collection and definitions
The baseline examination took place approximately 4 weeks before the date of bariatric surgery for both the surgery patients and the controls. Physical examination was undertaken at the baseline examination and after 0.5, 1, 2, 3, 4, 6, 8, 10 and 15 years. Fasting blood samples and 24 h urine collections were obtained and biochemical assays were performed at the baseline visit and after 2, 10 and 15 years at the Central Laboratory, Sahlgrenska University Hospital, Gothenburg, Sweden (accredited according to European Norm 45001). The 24-h urine collection was performed at home according to detailed instructions. Urinary albumin excretion was calculated based on the 24-h urine collection, according to the formula: (urine albumin concentration (mg l−1) × urine volume (l))/urine collection time (min) and expressed as mg per 24 h. Albuminuria was defined as urinary albumin excretion of 30 mg/24 h or more (corresponding to 20 μg/min or more).27 Impaired fasting glucose was defined as fasting blood glucose of at least 90 mg dl−1 and less than 110 mg dl−1 (corresponding to fasting blood glucose of 5.0 mmol l−1 or more and less than 6.1 mmol l−1). Type 2 diabetes was defined as fasting blood glucose of 110 mg dl−1 or more (corresponding to 6.1 mmol l−1 or more) and/or therapy with glucose-lowering medications.28,29 Hypertension was defined as systolic blood pressure of at least 140 mm Hg or diastolic blood pressure of at least 90 mm Hg or treatment with antihypertensive medication.30 The sagittal diameter, measured as the distance between the examination table and a carpenter's level held horizontally across the abdomen at the level of the iliac crest, was used as an index of intraabdominal pressure and visceral adiposity.12
The relevant regional ethics review boards in Sweden approved the study protocol and informed consent was obtained from all participants. The study has been registered at ClinicalTrials.gov (NCT01479452).
Statistical analyses
Mean values, with s.d. and percentages were used to describe the baseline characteristics. Baseline differences between treatment groups were evaluated by using t-tests for continuous variables and Fisher’s exact text for categorical variables. Participants were followed up either until the diagnosis of albuminuria, or until their last follow-up examination, whichever occurred first. Those without albuminuria during follow-up were thus censored at their last follow-up visit.
Time to albuminuria diagnosis was compared between the bariatric surgery and control groups with Kaplan–Meier estimates of cumulative incidence rates. The log-rank test was used to examine differences in the cumulative incidence. The hazard ratio from a Cox proportional-hazards model with a single covariate for treatment group (surgery or control) was calculated. In addition, hazard ratios were calculated adjusted for age, gender, waist hip ratio, sagittal diameter, diabetes, hypertension, triglycerides and albumin excretion at baseline using a multivariate Cox regression model.
In secondary subgroup analyses, the cumulative incidence of albuminuria was calculated separately in subgroups defined according to baseline parameters. The association between risk factors and the effect of bariatric surgery on the development of albuminuria was tested by including the corresponding interaction term in the Cox proportional hazard regression model. In these calculations, dichotomous variables could have one of the two values (for example, male or female sex). For other traits, the interaction tests were conducted using the original continuous variable, dichotomised based on median baseline values. A total of 18 post hoc treatment interaction analyses were performed.
The number needed to treat to prevent the development of albuminuria in one patient at 10 years was calculated in different subgroups as the reciprocal of the absolute risk difference between the bariatric surgery and control groups.
All P-values are two-tailed and P<0.05 was considered to be statistically significant. In all calculations, the intention-to-treat principle was applied. The Stata statistical package, version 10.1 (StataCorp, College Station, TX, USA), was used.
Results
Baseline characteristics, follow-up rates and weight changes during follow-up
Characteristics of the SOS participants included in this report are shown in Table 1. For most of the baseline characteristics, participants in the surgery group were more metabolically deranged than the controls. At baseline, mean BMI was higher in the bariatric surgery group compared with the control group, and the surgery group had a higher proportion of individuals with risk factors for albuminuria (type 2 diabetes, hypertension and smokers) compared with the control group.
The median follow-up time in this analysis was 10 years (interquartile range 2 to 10 years, maximum 15 years). After adjustment for mortality, the rates of follow-up were 87% at 2 years and 74% at 10 years. After adjustment, also for those patients who had not yet been followed for 15 years at the time of analysis, the follow-up rate was 52% at 15 years.
No significant weight loss was observed in the control group during 15 years of follow-up (Figure 1). In contrast, the average weight loss in the bariatric surgery group was 25% after 1 year. After partial weight regain, the average weight loss at 15 years was 16% (Figure 1; P<0.001 vs controls). At all the time points we examined, the weight loss was greater after gastric bypass than after banding or vertical banded gastroplasty (Supplementary Figure 1).

Mean body weight changes (%) and 95% confidence intervals (bars) over 15 years in the control and surgery groups of the SOS study.
Incidence of albuminuria
During the follow-up period, albuminuria developed in 246 patients in the control group and 126 patients in the bariatric surgery group (Figure 2a), corresponding to incidence rates of 20.4 cases (95% confidence interva (CI), 18.0 to 23.2) and 9.4 cases (95% CI, 7.9 to 11.2) per 1000 person years, respectively (log-rank P<0.001; unadjusted hazard ratio=0.46, 95% CI, 0.37–0.57). After adjustment for confounding baseline factors (age, gender, BMI, sagittal diameter, diabetes, hypertension, triglycerides and urinary albumin excretion), the hazard ratio was 0.37 (Table 2).

Kaplan–Meier estimates of cumulative incidence of albuminuria in the control group compared with the entire surgery group (a) and to the surgery group plotted according to the method of bariatric surgery (b). Albuminuria was defined as urinary albumin excretion equal to or above 30 mg per 24 h or more. The unadjusted hazard ratio and the 95% CI are shown in the figure using the control group as reference.
Subgroup analysis
All three types of bariatric surgery were associated with a reduced incidence of albuminuria compared with usual care (P⩽0.001; Figure 2b). Within the surgery group, the hazard ratios for albuminuria in the banding and vertical banded gastroplasty groups as compared with the GBP group were 1.62 (95% CI 0.78–3.34, P=0.19) and 1.54 (95% CI 0.80–2.94, P=0.20), respectively (Figure 2b). The non-significant P-values remained after exclusion of patients in the banding and vertical banded gastroplasty groups who were converted to GBP during follow-up. However, it should be noted that the number of events in these analyses were low, affecting the power of the tests.
The incidence of albuminuria in subgroups defined according to baseline parameters and interactions between baseline risk factors and treatment are shown in Table 3. In the control group, many high-risk subgroups (for example, male sex, diabetes, hypertension, high sagittal diameter, high insulin, high glucose, high urine albumin excretion) had a higher incidence of albuminuria than the corresponding low-risk subgroups (Panel A in Table 3).
The association between bariatric surgery and reduced incidence of albuminuria was significant in all subgroups with hazard ratios ranging from 0.35 to 0.55 (Panel B in Table 3). However, the relative treatment effects of bariatric surgery were not significantly different between any of the subgroups (Panel B in Table 3).
The estimated number needed to treat to prevent one case of albuminuria over 10 years in the entire study group was 9 (95% CI 7.1–12.5; Panel C in Table 3). A difference in the number needed to treat between subgroups defined by baseline factors was found when the SOS cohort was subdivided by median baseline urine albumin excretion (9.3 mg per 24 h), serum triglycerides (154 mg dl−1), diabetes and sex. In individuals with baseline urine albumin excretion below or equal to the median, the number needed to treat was fourfold higher than in individuals with albumin excretion rates greater than median at baseline (Panel C in Table 3).
Discussion
In the current report, we examined the long-term effects of bariatric surgery on albumin excretion in patients without albuminuria at study start. Our results show that bariatric surgery is associated with more than 50% lower incidence of albuminuria compared with conventional obesity treatment. Although gastric bypass resulted in greater weight loss, the preventive effect on albuminuria was not different compared with the restrictive procedures but this should be interpreted with caution because the SOS study was not designed to detect such differences. In the whole cohort, surgical treatment of nine patients was needed to prevent the development of albuminuria in one patient at 10 years. However, in some high-risk subgroups (men, diabetics and participants with high triglyceride levels or high urinary albumin excretion at study start), the number of surgeries needed to prevent the development of albuminuria in one patient was lower than in the corresponding low-risk groups. In these high-risk groups, one case of albuminuria was prevented for every four to six surgeries. It should also be noted that, although all participants in this study were free from albuminuria (baseline urinary albumin excretion less than 30 mg per 24 h), baseline urine albumin excretion above the median (9.3 mg per 24 h) was associated with increased progression to albuminuria.
The mechanisms behind the beneficial effects of bariatric surgery on albuminuria are largely unknown. Obesity per se is an independent risk factor for renal disease6,7 and is associated with hemodynamic, structural and functional changes of the kidney as well as increased albuminuria.6,31 In addition, metabolic syndrome, diabetes and hypertension, well established as major causes of chronic kidney disease,32 are closely associated with obesity.2, 3, 4 The effect of bariatric surgery on albuminuria incidence may be mediated by the improvement of several risk factors for this condition (for example, diabetes, hypertension and metabolic syndrome). It has also been shown that western style diet with high content of sodium, fat and protein from red meat increases the risk of chronic kidney disease.33 It is therefore possible that the dramatic reduction in food intake after bariatric surgery protects against kidney damage and contributes to the reduced incidence of albuminuria in our study.
Interestingly, although obesity is associated with increased risk for albuminuria,10,11 the incidence of albuminuria in the control group during the 15-year follow-up was almost identical in subjects with baseline BMI above and below the median in the SOS cohort. In contrast, albuminuria incidence in the control group was higher in individuals with high sagittal diameter, a marker for visceral fat and intraabdominal pressure.12 In addition, higher baseline fasting insulin, glucose and triglycerides and lower HDL cholesterol were associated with increased albuminuria incidence in the control group, indicating that metabolic parameters rather than BMI are predictors of an increased incidence of albuminuria among obese individuals. Obesity is characterized by a varying degree of resistance to the physiological effect of insulin. Recent observations suggest that insulin signaling in podocytes, cells having a pivotal role in kidney filtration, contributes to albuminuria.34, 35, 36 This could potentially explain why albuminuria incidence is associated with metabolic features rather than with BMI per se in the control group in the present study. Our results also show that the effect of bariatric surgery on albuminuria incidence was similar for subgroups with high and low BMI at baseline. This is in line with our earlier observations that baseline BMI does not predict the treatment benefit of bariatric surgery in obese subjects.24,25,37
A limitation of this study is that intervention in the SOS study was not randomized owing to ethical considerations related to the high postoperative mortality associated with bariatric surgery in the 1980s.38 In addition, there were baseline differences between the surgery and control groups in the subgroup of the original SOS cohort used for the current study. However, the risk factors were worse in the surgery group compared with the control group, and, if anything, our data may therefore underestimate the effects of surgery compared with conventional management. Another limitation is that the SOS study was not primarily designed to assess the effect of bariatric surgery on albuminuria incidence; nonetheless all the analyzed variables were collected prospectively. Further longitudinal randomized-controlled trials are therefore warranted to confirm our results. A strength of the study is that albuminuria measurement was based on a 24 h urine collection. This method is a more reliable way to assess albuminuria in morbidly obese individuals compared with other parameters (for example, albumin-to-creatinine ratio).39 As the collection was performed by the patients, there is a risk of over- or under collection of 24 h urine; however, this is likely to affect both treatment groups.
In conclusion, our results show for the first time that bariatric surgery is associated with reduced long-term incidence of albuminuria in obese individuals. Baseline BMI did not influence the incidence of albuminuria in the conventionally treated control group or the treatment benefit in the surgery group.
References
Flegal KM, Carroll MD, Ogden CL, Curtin LR . Prevalence and trends in obesity among US adults, 1999-2008. JAMA 2010; 303: 235–241.
Bray GA . Medical consequences of obesity. J Clin Endocrinol Metab 2004; 89: 2583–2589.
Chan JM, Rimm EB, Colditz GA, Stampfer MJ, Willett C . Obesity, fat distribution, and weight gain as risk factors for clinical diabetes in men. Diabetes Care 1994; 17: 961–969.
Mokdad AH, Ford ES, Bowman BA, Dietz WH, Vinicor F, Bales VS et al. Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA 2003; 289: 76–79.
McTigue K, Larson JC, Valoski A, Burke G, Kotchen J, Lewis CE et al. Mortality and cardiac and vascular outcomes in extremely obese women. JAMA 2006; 296: 79–86.
Hunley TE, Ma LJ, Kon V . Scope and mechanisms of obesity-related renal disease. Curr Opin Nephrol Hypertens 2010; 19: 227–234.
Ejerblad E, Fored CM, Lindblad P, Fryzek J, McLaughlin JK, Nyren O . Obesity and risk for chronic renal failure. J Am Soc Nephrol 2006; 17: 1695–1702.
Verhave JC, Gansevoort RT, Hillege HL, Bakker SJ, De Zeeuw D, de Jong PE . An elevated urinary albumin excretion predicts de novo development of renal function impairment in the general population. Kidney Int Suppl 2004; 92: S18–S21.
Viazzi F, Leoncini G, Conti N, Tomolillo C, Giachero G, Vercelli M et al. Microalbuminuria is a predictor of chronic renal insufficiency in patients without diabetes and with hypertension: the MAGIC study. Clin J Am Soc Nephrol 2010; 5: 1099–1106.
Kawar B, Bello AK, El Nahas AM . High prevalence of microalbuminuria in the overweight and obese population: data from a UK population screening programme. Nephron Clin Pract 2009; 112: c205–c212.
Chandie Shaw PK, Berger SP, Mallat M, Frolich M, Dekker FW, Rabelink TJ . Central obesity is an independent risk factor for albuminuria in nondiabetic South Asian subjects. Diabetes Care 2007; 30: 1840–1844.
Sugerman H, Windsor A, Bessos M, Wolfe L . Intra-abdominal pressure, sagittal abdominal diameter and obesity comorbidity. J Intern Med 1997; 241: 71–79.
Sugerman HJ . Effects of increased intra-abdominal pressure in severe obesity. Surg Clin North Am 2001; 81: 1063–1075 vi.
Sugerman HJ . Comment on: Correlations between intra-abdominal pressure and obesity-related co-morbidities. Surg Obes Relat Dis 2009; 5: 528–529.
Straznicky NE, Grima MT, Lambert EA, Eikelis N, Dawood T, Lambert GW et al. Exercise augments weight loss induced improvement in renal function in obese metabolic syndrome individuals. J Hypertens 2011; 29: 553–564.
Sjöström L, Narbro K, Sjöström CD, Karason K, Larsson B, Wedel H et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med 2007; 357: 741–752.
Iaconelli A, Panunzi S, De Gaetano A, Manco M, Guidone C, Leccesi L et al. Effects of bilio-pancreatic diversion on diabetic complications: a 10-year follow-up. Diabetes Care 2011; 34: 561–567.
Hofso D, Nordstrand N, Johnson LK, Karlsen TI, Hager H, Jenssen T et al. Obesity-related cardiovascular risk factors after weight loss: a clinical trial comparing gastric bypass surgery and intensive lifestyle intervention. Eur J Endocrinol 2010; 163: 735–745.
Navarro-Diaz M, Serra A, Romero R, Bonet J, Bayes B, Homs M et al. Effect of drastic weight loss after bariatric surgery on renal parameters in extremely obese patients: long-term follow-up. J Am Soc Nephrol 2006; 17: S213–S217.
Chagnac A, Weinstein T, Herman M, Hirsh J, Gafter U, Ori Y . The effects of weight loss on renal function in patients with severe obesity. J Am Soc Nephrol 2003; 14: 1480–1486.
Agrawal V, Krause KR, Chengelis DL, Zalesin KC, Rocher LL, McCullough PA . Relation between degree of weight loss after bariatric surgery and reduction in albuminuria and C-reactive protein. Surg Obes Relat Dis 2009; 5: 20–26.
Brethauer SA, Aminian A, Romero-Talamas H, Batayyah E, Mackey J, Kennedy L et al. Can diabetes be surgically cured? Long-term metabolic effects of bariatric surgery in obese patients with type 2 diabetes mellitus. Ann Surg 2013; 258: 628–636 discussion 636-7.
Sjöström L, Lindroos AK, Peltonen M, Torgerson J, Bouchard C, Carlsson B et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med 2004; 351: 2683–2693.
Sjöström L, Peltonen M, Jacobson P, Sjöström CD, Karason K, Wedel H et al. Bariatric surgery and long-term cardiovascular events. JAMA 2012; 307: 56–65.
Carlsson LM, Peltonen M, Ahlin S, Anveden A, Bouchard C, Carlsson B et al. Bariatric surgery and prevention of type 2 diabetes in Swedish obese subjects. N Engl J Med 2012; 367: 695–704.
Sjöström L, Larsson B, Backman L, Bengtsson C, Bouchard C, Dahlgren S et al. Swedish obese subjects (SOS). Recruitment for an intervention study and a selected description of the obese state. Int J Obes Relat Metab Disord 1992; 16: 465–479.
Molitch ME, DeFronzo RA, Franz MJ, Keane WF, Mogensen CE, Parving HH et al. Nephropathy in diabetes. Diabetes Care 2004; 27: S79–S83.
World Health Organization. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications. Report of a WHO Consultation. Part 1: Diagnosis and Classification of Diabetes Mellitus. World Health Org (Rep. no 99.2): Geneva 1999.
American Diabetes Association. Executive summary: standards of medical care in diabetes—2011. Diabetes Care 2011; 34: S4–S10.
Whitworth JA . 2003 World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension J Hypertens, 2003; 21: 1983–1992.
Eknoyan G . Obesity and chronic kidney disease. Nefrologia 2011; 31: 397–403.
Stenvinkel P . Chronic kidney disease: a public health priority and harbinger of premature cardiovascular disease. J Intern Med 2010; 268: 456–467.
Odermatt A . The Western-style diet: a major risk factor for impaired kidney function and chronic kidney disease. Am J Physiol Renal Physiol 2011; 301: F919–F931.
Coward RJ, Saleem MA . Podocytes as a target of insulin. Curr Diabetes Rev 2011; 7: 22–27.
Coward RJ, Welsh GI, Yang J, Tasman C, Lennon R, Koziell A et al. The human glomerular podocyte is a novel target for insulin action. Diabetes 2005; 54: 3095–3102.
Welsh GI, Hale LJ, Eremina V, Jeansson M, Maezawa Y, Lennon R et al. Insulin signaling to the glomerular podocyte is critical for normal kidney function. Cell Metab 2010; 12: 329–340.
Sjöholm K, Anveden A, Peltonen M, Jacobson P, Romeo S, Svensson PA et al. Evaluation of Current Eligibility Criteria for Bariatric Surgery: Diabetes prevention and risk factor changes in the Swedish Obese Subjects (SOS) study. Diabetes Care 2013; 36: 1335–1340.
Brolin RE . Results of obesity surgery. Gastroenterol Clin North Am 1987; 16: 317–338.
Guidone C, Gniuli D, Castagneto-Gissey L, Leccesi L, Arrighi E, Iaconelli A et al. Underestimation of urinary albumin to creatinine ratio in morbidly obese subjects due to high urinary creatinine excretion. Clin Nutr 2012; 31: 212–216.
Acknowledgements
This study was supported by grants from the Swedish Research Council (K2012- 55X-22082-01-3, 2013-99X-22279-01-3, 2013-54X-11285-19-5), the Swedish Foundation for Strategic Research to Sahlgrenska Center for Cardiovascular and Metabolic Research, the Swedish federal government under the LUA/ALF agreement concerning research and education of doctors and the VINNOVA-VINNMER program. The SOS study has previously been supported by grants Hoffmann–La Roche, AstraZeneca, Cederroth, Sanofi-Aventis, and Johnson & Johnson. Sponsors had no role in the design or management of the study or in the collection, analysis or interpretation of the data. Medical writers were not used. We thank the staff members at 480 primary health care centers and 25 surgical departments in Sweden that participated in the study. We also thank Gerd Bergmark, Christina Torefalk and Lisbeth Eriksson for administrative support and Rosie Perkins for editing the manuscript (all employed by the Institute of Medicine, University of Gothenburg).
Author Contributions
Dr Peltonen had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Carlsson, Romeo, Jacobson, Sjöholm, Svensson, Haraldsson, Peltonen and Sjöström were responsible for the study concept and design. Carlsson, Jacobson, Sjöholm, Svensson, Peltonen and Sjöström were responsible for acquisition of data. Carlsson, Romeo, Jacobson, Burza, Maglio, Sjöholm, Svensson, Haraldsson, Peltonen and Sjöström were responsible for analysis and interpretation of data. Carlsson, Romeo, Peltonen and Sjöström drafted the manuscript. Carlsson, Romeo, Jacobson, Burza, Maglio, Sjöholm, Svensson, Haraldsson, Peltonen and Sjöström were responsible for critical revision of the manuscript for important intellectual content. Peltonen performed statistical analysis. Carlsson, Sjöholm, Svensson, Peltonen and Sjöström obtained the funding. Carlsson, Jacobson, Sjöholm, Svensson and Sjöström provided administrative, technical or material support. Carlsson, Peltonen and Sjöström supervised the study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
Lena Carlsson reports receiving consulting fees from AstraZeneca and owning stock in Sahltech; Lars Sjöström reports serving as a member of the board of Lenimen, receiving lecture fees from AstraZeneca and Johnson & Johnson and providing an expert statement on drug effects and weight-loss effects on obesity for AstraZeneca. The remaining authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on International Journal of Obesity website
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution 3.0 Unported License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/3.0/
About this article

Cite this article
Carlsson, L., Romeo, S., Jacobson, P. et al. The incidence of albuminuria after bariatric surgery and usual care in swedish obese subjects (SOS): a prospective controlled intervention trial. Int J Obes 39, 169–175 (2015). https://doi.org/10.1038/ijo.2014.72
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ijo.2014.72
Keywords
This article is cited by
-
Prevalence and Clinical Predictors of Hyperuricemia in Chinese Bariatric Surgery Patients
Obesity Surgery (2022)
-
Remission and progression of pre-existing micro- and macroalbuminuria over 15 years after bariatric surgery in Swedish Obese Subjects study
International Journal of Obesity (2021)
-
Bariatric Surgery Is Protective Against Renal Function Decline in Severely Obese Patients in the Long-Term
Obesity Surgery (2021)
-
Bariatric surgery for the treatment of chronic kidney disease in obesity and type 2 diabetes mellitus
Nature Reviews Nephrology (2020)
-
Analyzing the Impact of Bariatric Surgery in Kidney Function: a 2-Year Observational Study
Obesity Surgery (2019)
