
Abstract
Retinal vascular events are perceived to be related to various cardiovascular complications. We conducted a systematic review to assess the relationship between retinal artery/vein occlusions (RAO/RVO) and the incidence of mortality, stroke, and myocardial infarction (MI). A comprehensive electronic literature search selected 93 relevant studies between 1992–2015: 16 articles qualified for inclusion (7 for mortality rate and MI, 11 for stroke). No published articles examined associations of RAO to mortality or MI, but only to stroke. Because of the heterogeneity of studies, no meta-analysis was performed. The association with mortality risk was highest at ~34.7% in RVO subgroup; whereas for MI, the risk was comparatively lower at 3.9–5.7% for RVO. There was no significant difference in stroke rate when comparing central and branch RVO subgroups (6.5%), but was significantly higher at 19.6–25% in RAO. There is a positive association of retinal vascular events to mortality, stroke, and MI. RAO is associated with a higher risk of stroke. Given that RAO and RVO patients would generally present to ophthalmologists, their high cardiovascular risk should include a referral for cardiovascular assessment as part of their management protocol.
Similar content being viewed by others

Introduction
Retinal vascular occlusion is the second most common cause of blindness from retinal vascular disease after diabetic retinopathy.1, 2, 3 The terminology broadly includes retinal vein occlusion (RVO) where retinal vascular blockage involves the retinal veins, and retinal artery occlusion (RAO) where the blockage is at the retinal artery tributary. The prevalence of RVO is estimated to be 0.7–1.6% of the general population,1, 2 whereas RAO is much less common.
Whilst RVO is commonly characterised by a localised thrombus formation, often aggravated by external compression on the retinal vein from atherosclerotic retinal artery; RAO is a thromboembolic event lodged by a platelet-fibrinous embolus in the bifurcation of retinal artery, commonly from a remote atherosclerotic arterial disease. Although both RAO and RVO can lead to significant visual disability, RAO is regarded more as an ophthalmic emergency and as the ocular analogue of stroke. In general, retinal vascular event is well known to be associated with common underlying systemic risk factors include hypertension, ischaemic heart disease, diabetes mellitus, and carotid artery disease. As far as we are aware, a systematic review investigating the associations of retinal vascular events to mortality, strokes, and myocardial infarction (MI) has not been previously performed.
Our objective was to conduct a systematic review to assess the relationship between retinal vascular events (RAO and RVO) and the incidence of mortality, stroke, and MI.
Materials and methods
A comprehensive literature search using PubMed/Medline was performed electronically, yielding 93 articles published between 1992 and January 2015. The search terms used in combination were ‘retinal vein occlusion’, ‘retinal artery occlusion,’ ‘mortality’, ‘stroke’, ‘CVA’, ‘cerebrovascular accident’, and ‘myocardial infarction’.
The articles obtained were filtered on the basis of relevancy of abstract and the title. The selection criteria prepared were intended to include studies that concerned the relationship between RAO and RVO with mortality, stroke, or MI incidence. Therefore, articles that were reviews or case reports were excluded. Only articles in the English language were included in this review.
We excluded studies that detailed focus on co-morbidities associated with RAO and RVO such as diabetes and hypertension, as the main purpose of the systematic review is to identify RAO or RVO and its specific relationship to mortality, stroke, and MI occurrence alone. For articles achieving the eligibility criteria stated, the full text was obtained and the reference lists were scanned for further relevant articles. Because of the heterogeneity of studies, no meta-analysis was performed.
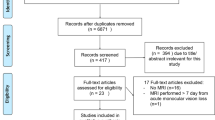
Of the initial 93 articles selected, 27 papers were screened in full, then three were excluded for not focusing on stroke or MI, four studies investigated RVO epidemiology and recurrence, and four studies investigated the pathophysiology of RVO. Finally, 16 studies qualified for inclusion in this review with mortality rate and MI being the focus in seven separate studies, and stroke in 11 studies (Figure 1). Of these studies, only two were based on RAO, 13 on RVO, and one on both RAO and RVO.

Flow chart on studies selection.
In the literature obtained, RAO and RVO are classified according to where the blockage is located. Occlusion of the central retinal vein is referred to as central retinal vein occlusion (CRVO) and obstruction at any distal venules is referred to as branch retinal vein occlusion (BRVO).
Results
Mortality rate in RVOs
We identified four case–control studies and three case-series assessing the association between RVO and mortality risk (Table 1).2, 4, 5, 6 The largest case–control study had a propensity-matched design.4 There were no studies reporting on the association between RAO and mortality. Table 1a shows the mortality rates ranged from 3.0 to 33.4% in controls and 8.2–33.8% in RVO patients. The larger difference is reported by the smaller sample size studies, but insignificant in the largest study. Some subgroups analyses showed only a slightly higher mortality rate of 30.1–34.7% in CRVO, compared with 22.6–33.3% in BRVO patients.2, 4, 5, 6 The results from case-series studies (Table 1b) show a mortality rate of 16.7–19.2% in CRVO patients and 15.6–43.8% in BRVO patients, compared with a cited figure of 44.2% in the expected background population.7, 8, 9 For example, Tsaloumas et al7 concluded MI as the main cause of death in the RVO patients, being significantly higher (23.1%) compared with the background population (14.4%). The other two studies did not find any difference between presence of RVO and subsequent mortality rates. The mean follow-up duration was much longer than in the case–control studies.
Stroke rate in retinal vascular events
There were eight case–control studies that reported on the association of stroke in retinal vascular events and two of these studies included the RAO category (Table 2). Table 2a shows reports on seven case–control studies: a stroke rate of 6.7–35.1% in RVO patients compared with 2.1–19.9% in controls.4, 5, 10, 11, 12, 13, 14 All except one study indicated a positive association with stroke risk amongst RVO patients.4, 5, 10, 11, 12, 13 Shih et al4 reported no significant difference in stroke rate when comparing the CRVO (6.4%) and BRVO (6.8%) subgroups, but RVO remained a significant predictor for stroke development (after adjustment) among the age group of 60–69 years.14 Two studies also recorded transient ischaemic attack occurrence alongside stroke incidence.11, 13
Table 2b summarises case–control studies reporting associations to stroke risk amongst RAO patients, with rates ranging from 19.6 to 25.0% in RAO patients, and 10.1–14.8% in controls. Christiansen et al13 investigated patients with atrial fibrillation, and their positive association of stroke and transient ischaemic attack rates extended to a smaller subgroup of patients with combined RAO and RVO in one eye of 20%, but not any higher than the groups with lone RAO or RVO. Table 2c summarises findings from three case-series studies, which found no positive association between RVO and stroke, with a low stroke rate of 1.3–1.8%.7, 8 One study reported a 74.2% risk of developing asymptomatic cerebral infarction.16
MI rate in RVOs
Table 3a summarises results from five case–control studies assessing the association between RVO and MI, with a variable rate ranging from 1.3 to 3.9% in RVO patients (3.1–5.0% in CRVO and 1.4–5.7% in BRVO), compared with 0.8–3.4% amongst controls.4, 5, 10, 17, 18 There were no published studies reporting the association of MI in RAO. Table 3b is based on two case-series studies, reporting a low 2.0–6.4% risk of MI in RVO patients with no positive association seen.7, 8
Figure 2 illustrates a forest plot of hazard ratios for the associations of RVO and mortality, stoke, and MI.

Retinal vein occlusion and hazard ratios available from various studies for mortality, stroke, and myocardial infarction.
Discussion
Retinal vascular events would have been expected to relate to mortality, stroke, or MI. This systemic review confirms their positive associations. The association with mortality risk was highest at ~34.7% in RVO subgroup; whereas for MI risk was comparatively lower at 3.9–5.7% for RVO. There was no significant difference in stroke rate when comparing central and branch RVO subgroups (6.5%), but was significantly higher at 19.6–25% in RAO (summarised in Table 4).2, 4, 5, 6, 7, 10, 13, 15, 17
The relationship between retinal vascular events and the various cardiovascular complications perhaps represents the presence of co-morbidities common to all. Conditions such as hypertension, hyperlipidemia, carotid artery disease, and diabetes mellitus are common risk factors associated with cardiovascular morbidity and mortality. Large population-based studies have confirmed significant relationships of various systemic cardiovascular risk factors with RVO, for example, hypertension, hypertriglyceridemia and renal dysfunction.1 This would explain the higher rate of mortality as RVO relates to and includes many ‘high risk’ factors, not just specific to death related to stroke or MI.
Specifically, we found no published studies linking RAO with mortality or MI. The only two studies providing RAO data were focused on stroke, from Denmark and Taiwan, as both countries have well established national database tracking systems for diagnosis. The risk of stroke in RAO patients was significantly higher compared with RVO (Table 4).4, 5, 10, 13, 15 This is perhaps consistent with expectations, based on their pathophysiological associations. The Danish study also found that in patients with established atrial fibrillation and coexisting RAO or RVO could accentuate the risk of incident stroke.13 As some of the increased risks associated with RVO were attributed to other adverse cardiovascular co-morbidities in these patients, it is more likely that RAO and RVO remain important independent predictors of future stroke in patients suffering from atrial fibrillation.
Limitations
Our systematic review was able to obtain useful data for the RVO group, but relatively few published papers were available for RAO group. A possible explanation is that RAO patients often acutely present to ophthalmologists and are immediately referred to the ‘stroke unit’ for a systemic workup, often without further review arrangements in the eye department.
Each published study varied in length of follow-up ranging from 3 to 13 years, making valid comparisons and meta-analysis difficult tasks. There was also a wide range in study sample sizes in the published case-series and case–control studies, ranging from as low as 31 patients to many thousands of studied subjects. Most of the larger case–control population studies do confirm the positive association of retinal vascular events to cardiovascular events.4, 5, 10, 12, 17 Certain studies involved different ethnic groups, age ranges, and lifestyle-related risk factors, and their results may not be necessarily applicable for direct comparisons. Older age was associated with a higher prevalence of RVO and age-stratified mortality (men and women 60–69 years of age) in almost all studies, and one non-controlled study from Taiwan reported a higher morbidity and mortality amongst younger (age <40 years) CRVO patients.5, 19
In addition, not all patients with retinal vascular events would be routinely referred to physicians for cardiovascular assessments. Some studies conducted by physicians rather than by eye specialists may only include data from patients with retinal vascular events who were specifically referred to their unit. Finally, less precise diagnosis or coexisting disease(s) such as diabetic retinopathy plus RVO, may have led to misclassification.
Conclusion
There is a positive association of retinal vascular events to mortality, stroke, and MI. RAO is associated with a higher risk of stroke, but few studies have examined its relationship to mortality and MI. Given the high overall risks compared with the normal general population, further studies are needed to define this relationship, the impact of cardiovascular prevention strategies, and the impact of early treatments in the eye department when these patients first present. As RAO and RVO patients would generally present to ophthalmologists, their high cardiovascular risk would imply that a cardiologist’s assessment would be necessary as part of their management protocol.
References
Cheung N, Klein R, Wang JJ, Cotch MF, Islam AF, Klein BE et al. Traditional and novel cardiovascular risk factors for retinal vein occlusion: the multiethnic study of atherosclerosis. Invest Ophthalmol Vis Sci 2008; 49 (10): 4297–4302.
Klein R, Klein BE, Moss SE, Meuer SM . The epidemiology of retinal vein occlusion: the Beaver Dam Eye Study. Trans Am Ophthalmol Soc 2000; 98: 133–141.
Rogers SL, McIntosh RL, Lim L, Mitchell P, Cheung N, Kowalski JW et al. Natural history of branch retinal vein occlusion: an evidence-based systematic review. Ophthalmology 2010; 117 (6): 1094–1101.
Shih C-H, Ou S-Y, Shih C-J, Chen Y-T, Ou S-M, Lee Y-J . Bidirectional association between the risk of comorbidities and the diagnosis of retinal vein occlusion in an elderly population: A nationwide population-based study. Int J Cardiol 2015; 178: 256–261.
Bertelsen M, Linneberg A, Christoffersen N, Vorum H, Gade E, Larsen M . Mortality in patients with central retinal vein occlusion. Ophthalmology 2014; 121 (3): 637–642.
Xu L, Liu WW, Wang YX, Yang H, Jonas JB . Retinal vein occlusions and mortality: the Beijing Eye Study. Am J Ophthalmol 2007; 144 (6): 972–973.
Tsaloumas MD, Kirwan J, Vinall H, O’Leary MB, Prior P, Kritzinger EE et al. Nine year follow-up study of morbidity and mortality in retinal vein occlusion. Eye (Lond) 2000; 14 (Pt 6): 821–827.
Mansour AM, Walsh JB, Henkind P . Mortality and morbidity in patients with central retinal vein occlusion. Ophthalmologica 1992; 204 (4): 199–203.
Christoffersen N, Gade E, Knudsen L, Juel K, Larsen M . Mortality in patients with branch retinal vein occlusion. Ophthalmology 2007; 114 (6): 1186–1189.
Werther W, Chu L, Holekamp N, Do D V, Rubio RG . Myocardial infarction and cerebrovascular accident in patients with retinal vein occlusion. Arch Ophthalmol 2011; 129 (3): 326–331.
Di Capua M, Di Minno MND, Guida A, Loffredo M, Cuccaro C, Coppola A et al. Coronary artery disease, cerebral non-fatal ischemic stroke in retinal vein occlusion: an 8-yr follow-up. Nutr Metab Cardiovasc Dis 2012; 22 (1): 23–27.
Rim TH, Kim DW, Han JS, Chung EJ . Retinal vein occlusion and the risk of stroke development. Ophthalmology 2015; 122 (6): 1187–1194.
Christiansen CB, Lip GYH, Lamberts M, Gislason G, Torp-Pedersen C, Olesen JB . Retinal vein and artery occlusions: a risk factor for stroke in atrial fibrillation. J Thromb Haemost 2013; 11 (8): 1485–1492.
Ho J, Liou S . Retinal vein occlusion and the risk of stroke development: a five-year follow-up study. Am J Ophthalmol 2009; 147 (2): 283–290.
Chang Y-S, Jan R-L, Weng S-F, Wang J-J, Chio C-C, Wei F-T et al. Retinal artery occlusion and the 3-year risk of stroke in Taiwan: a nationwide population-based study. Am J Ophthalmol 2012; 154 (4): 645–652.e1.
Ueda Y, Kanazawa S, Ohira A, Miyamura N, Takaki T, Kitaoka T et al. Retinal vascular obstruction and asymptomatic cerebral infarction. Jpn J Ophthalmol 2002; 46 (2): 209–214.
Bertelsen M, Linneberg A, Rosenberg T, Christoffersen N, Vorum H, Gade E et al. Comorbidity in patients with branch retinal vein occlusion: case-control study. BMJ 2012; 345: e7885.
Hu C-C, Ho J-D, Lin H-C . Retinal vein occlusion and the risk of acute myocardial infarction (correction of infraction): a 3-year follow-up study. Br J Ophthalmol 2009; 93 (6): 717–720.
Kuo JZ, Lai CC, Ong FS, Shih CP, Yeung L, Chen TL et al. Central retinal vein occlusion in a young Chinese population: risk factors and associated morbidity and mortality. Retina 2010; 30 (3): 479–484.
Acknowledgements
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
All authors contributed equally to this work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
GYHL is consultant for Bayer/Jansen J&J, BMS/Pfizer, Biotronik, Medtronic, Portola, Boehringer Ingelheim and Daiichi-Sankyo; speaker for Bayer, BMS/Pfizer, Medtronic, Boehringer Ingelheim, Microlife, Roche and Daiichi-Sankyo. The remaining authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Woo, S., Lip, G. & Lip, P. Associations of retinal artery occlusion and retinal vein occlusion to mortality, stroke, and myocardial infarction: a systematic review. Eye 30, 1031–1038 (2016). https://doi.org/10.1038/eye.2016.111
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2016.111
This article is cited by
-
Retinal vein occlusion is associated with stroke independent of underlying cardiovascular disease
Eye (2023)
-
Combination intravitreal anti-vascular endothelial growth factor inhibitors and macular laser photocoagulation relative to intravitreal injection monotherapy in macular oedema secondary to retinal vein occlusion: a meta-analysis of randomized controlled trials
Eye (2022)
-
The association of stroke with central and branch retinal arterial occlusion
Eye (2022)
-
Similarities and differences in systemic risk factors for retinal artery occlusion and retinal vein occlusion: A nationwide case–control study
International Ophthalmology (2022)
-
Efficacy and safety of non-vitamin K-antagonist oral anticoagulants for retinal vascular diseases in patients with atrial fibrillation: Korean cohort study
Scientific Reports (2020)
