
Abstract
Introduction
Surgically induced astigmatism is an unwanted variable that can lead to poorer visual and refractive outcomes in patients undergoing vitrectomy even when a technically precise procedure has been performed. This study assesses the difference in surgically induced astigmatism (SIA) between the traditional 20-gauge vitrectomy and the newer 25-gauge sutureless technique by comparing pre- and post-procedure keratometry readings.
Method
The study is a retrospective consecutive case series of vitrectomies performed by a single surgeon. There were a total of 47 patients, eight with bilateral procedures, 24 who underwent the 20 gauge, and 31 who had the 25-gauge procedure. Patients were excluded for corneal altering pathology or scleral buckling procedures. Vector analysis of pre- and post-vitrectomy readings was performed using Alpin's method, facilitated by the ASSORT program version 4.1.
Results
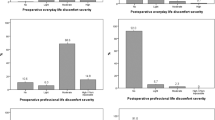
Mean time at which post-operative keratometry readings were taken was 3.9 months (1–36). Mean astigmatism at presentation was 0.63 D and 0.92 D and at post-surgically follow-up 1.14 D and 0.91 D (20 and 25 gauge, respectively). Mean SIA was 0.66 D (SD=0.8 D) for the 20-gauge group and 0.27 D (SD=0.23 D) for the 25 gauge (P=0.037). The calculated figure of SIA variability representing the 95% CI for the maximum amount of SIA for each procedure was 2.26 D and 0.73 D for the 20- and 25-gauge procedure, respectively.
Conclusions
The study shows that the 25-gauge technique involves a statistically significant reduction in the amount of SIA. This can ultimately lead to a better visual and refractive outcome for the patient.
Similar content being viewed by others


Introduction
With the advent of smaller microsurgical instruments, the 25-gauge ‘sutureless’ pars plana vitrectomy has rapidly been adopted as the preferred technique for vitreoretinal surgery. Currently, recognised advantages of the 25-gauge procedure include less postoperative pain and shorter operating times.1 This study aims to investigate the effect of both 20- gauge and 25-gauge vitrectomies on corneal curvature through a comparison of the differences in pre- and post-surgery keratometry readings. Post-vitrectomy astigmatism is a well-recognised consequence of vitrectomy.2, 3, 4, 5 The ability to minimise this surgically induced astigmatism (SIA) assists in achieving optimal refractive and visual outcomes for patients.
Materials and methods
The study is a retrospective, non-randomised consecutive case series of vitrectomies performed by a single surgeon (RDB). The study population consisted of 47 patients, eight of whom had bilateral procedures. The indications for vitrectomy included macular hole repair, epiretinal membrane peeling, and radial optic neurotomy. Twenty-four procedures were performed using the 20-gauge technique and 31 using the 25-gauge procedure. Exclusion criteria included; pathology altering corneal topography such as keratoconus, scleral buckling procedure, and the absence of pre- and post-vitrectomy keratometry.
Both the 20- and 25-gauge procedures were performed using a three-port pars plana technique: one irrigation port in the inferotemporal quadrant, and two instrument ports: superonasal and superotemporal. Twenty gauge procedures used instruments with a diameter of 0.813 mm and a cross-sectional area of 0.519 mm2, the sclerotomy sites were sutured using 8.0 vicryl. The 25-gauge technique used a trochar diameter of 0.519 mm with a cross-sectional area of 0.2026 mm2, the conjunctiva was caressed over the sclerotomy sites to assist in self–sealing; no sutures were used.
At presentation, all patients were phakic in the affected eye. This population was chosen as they all had post-vitrectomy keratometry readings recorded as part of pre-PHACO and IOL insertion investigations. Measurements were made using a manual keratometer, IOL Master, or Humphrey Autorefractor. Refractive values were not used as these include a component of lenticular astigmatism, an indeterminable variable.6, 7
Vector analysis of pre- and post-vitrectomy readings was performed using Alpin's method, facilitated by the ASSORT program version 4.1.8 All investigation was conducted in accordance with the Declaration of Helsinki of 1975.
Results
Postoperative keratometry readings were taken at mean of 3.9 months (1–36), with no statistically significant difference between follow-up for 20- and 25-gauge procedures.
Table 1 shows that the 25-gauge vitrectomy produces less astigmatism than the 20-gauge technique. The mean SIA for the 25-gauge procedure (0.27 D) was significantly less (P=0.037) than that for the 20-gauge procedure (0.66 D). The SD in SIA variation in the 25-gauge group was less than one-third of that in the 20-gauge group (0.73 vs 2.28).
Discussion
The magnitude of the difference in SIA between the 20- and 25-gauge groups is both statistically and may also be clinically significant considering the pathological indications for which the vitrectomies were undertaken. Through modern surgical techniques, visual outcomes in patients suffering from macular holes and epiretinal membranes are now exceptional. Kumagai et al,9 performed a long-term follow-up of 190 eyes who underwent macular hole repair (stage 2–4 macular holes) and found an average visual acuity of 0.12 logMAR, with 44% of patients achieving visual acuity ⩾6/6 and 86% achieving ⩾6/12. Epiretinal membrane peeling shows similarly successful visual outcomes, with reported mean visual improvement of 0.3 logMAR and mean post-operative visual acuity of 6/12.10 At these high levels of visual acuity, noticeable blur limits are much smaller11 and consequently a SIA of 0.27 D is expected to go unnoticed by the patient whereas 0.66 D may be visually detectable,12 possibly requiring a new spectacle prescription.
The precision of the refractive outcome is another important factor to consider when interpreting the findings of this study. The SD and 95% CI for the SIA in the 20- and 25-gauge groups were 0.8 and 2.28 D and 0.23 and 0.73 D, respectively. The 25-gauge group showed a far more precise and thus predictable amount of SIA than the 20-gauge group. This highlights yet another advantage of the 25-gauge procedure, as the surgeon can be assured that they are far less likely to induce large, unfavourable amounts of astigmatism.
Surgically induced astigmatism detracts from the visual acuity outcome of pseudophakic patients more than that of phakic patients. Given that almost all phakic patients undergoing vitrectomy will subsequently develop a cataract as procedural complication,13, 14 the resultant IOL implantation procedure provides an opportunity for correction of any SIA. Unfortunately, for the pseudophakic patient, any subsequent intervention to correct SIA will be an additional surgical procedure for that purpose only. Thus, in the absence of a corrective procedure, pseudophakic patients undergoing vitrectomy must bear any resultant astigmatism as an unfortunate consequence. Hence, a vitrectomy technique that minimises SIA provides a superior visual and refractive outcome, particularly for pseudophakic patients.
Although the sample size used in this study is commensurate with, and in most cases significantly greater than, the very few other studies in the area, this series does have some limitations. These relate to the inexact axis of port sites, absence of sequential keratometry readings, variable timing of keratometry readings, and the use of multiple varieties of keratometers.
The variable timing of post-vitrectomy keratometry measurements bears significance predominantly for the 20-gauge group, where vicryl sutures were used. These sutures take 6 weeks to dissolve and may affect corneal topography during this period. The average timing of post-vitrectomy keratometry measurements was 3.9 months, however, in the 20-gauge group only one patient had their keratometry readings recorded within 6 weeks of vitrectomy. The impact of this single reading on the data and conclusions drawn would be negligible.
The use of multiple keratometers to measure the corneal curvatures between preoperative and post-operative visits is a shortcoming of this study and is unfortunately an unavoidable consequence of conducting retrospective research. The impact of this confounder on the significance of the results presented here is debatable. Older studies have shown no significant difference between automated (portable and fixed) and manual keratometers,15, 16 whereas more recent authors have suggested the instruments may not be interchangeable.17
Conclusions
This retrospective study shows another advantage of the 25-gauge vitrectomy procedure over the 20-gauge procedure. The 25-gauge vitrectomy produces significantly less SIA and gives a more predictable and precise refractive result. If vitrectomy induced astigmatism can be minimised, additional refractive corrections are redundant. This difference is especially pertinent in patients who are likely to achieve a good visual outcome after the vitrectomy and those who are pseudophakic preoperatively.
References
Ibarra M, Hermel M, Prenner J, Hassan T . Longer-term outcomes of transconjunctival sutureless 25-gauge vitrectomy. Am J Ophthalmol 2005; 139: 831–836.
Randleman J, Hewitt S, Stulting R . Refractive changes after posterior segment surgery. Ophthalmol Clin North Am 2004; 17: 521-vi.
Sinha R, Sharma N, Verma L . Corneal topographic changes following retinal surgery. BMC Ophthalmol 2004; 4: 10.
Weinberger D, Lichter H, Loya N, Axer-Siegel R, Muzmacher L, Gabbay U et al. Corneal topographic changes after retinal and vitreous surgery. Ophthalmology 1990; 106 (8): 1521–1524.
Wirbelauer C, Hoerauf H, Roider J, Laqua H . Corneal shape changes after pars plana vitrectomy. Graefes Arch Clin Exp Ophthalmol 1998; 236: 822–828.
Dashevskii A, Kuzina E . Clinical aspects of vector analysis of lenticular astigmatism. Oftamol Zh 1987; 11: 70–72.
Liang D, Guan Z, Lin J . The relations of corneal, lenticular and total astigmatism. Yan Ke Xue Bao 1995; 11: 70–72.
Jaffe N, Jaffe G, Jaffe M . Postoperative Corneal Astigmatism. Mosby: St Louis, 1997.
Kumagai K, Furukawa M, Ogino N, Uemura A, Larson E . Long-term outcomes of internal limiting membrane peeling with and without indocyanine green in macular hole surgery. Retina 2006; 26: 613–617.
Wong J, Sachdev N, Beaumont P, Chang A . Visual outcomes following vitrectomy and peeling of epiretinal membrane. Clin Experiment Ophthalmol 2005; 33: 373–378.
Atchinson D, Fisher S, Pederson C, Ridall P . Noticable, troublesome and objectionable limits of blur. Vision Res 2005; 45: 1967–1974.
Miller A, Kris M, Griffiths A . Effect of small focal errors on vision. Optom Vis Sci 1997; 74 (7): 521–526.
Blodi B, Paluska S . Cataract after vitrectomy in young patients. Ophthalmology 1997; 104: 1092–1095.
Thompson J . The role of patient age and intraocular gas use in cataract progression after vitrectomy for macular holes and epiretinal membranes. Am J Ophthalmol 2004; 137: 250–257.
Knorz M, Kohl M, Trinkmann R . Automatic biometry and keratometry in comparison with the manual technic. Fortschr Ophthalmol 1989; 86 (2): 157–158.
Manning C, Kloess P . Comparison of portable automated keratometry and manual keratometry for IOL calculation. J Cataract Refract Surg 1997; 23 (8): 1213–1216.
Elbaz U, Barkana Y, Gerber Y, Avni I, Zadok D . Comparison of different techniques of anterior chamber depth and keratometric measurements. Am J Ophthalmol 2007; 143 (1): 48–53.
Author information
Authors and Affiliations
Corresponding author
Additional information
Proprietary interests: None
Presented at the ASCRS Symposium on Cataract, IOL and Refractive Surgery 2005 Washington
Rights and permissions
About this article
Cite this article
Galway, G., Drury, B., Cronin, B. et al. A comparison of induced astigmatism in 20- vs 25-gauge vitrectomy procedures. Eye 24, 315–317 (2010). https://doi.org/10.1038/eye.2009.81
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2009.81
Keywords
This article is cited by
-
Clinical factors contributing to postoperative aqueous flare intensity after 27-gauge pars plana vitrectomy for the primary rhegmatogenous retinal detachment
Japanese Journal of Ophthalmology (2019)
-
Evaluation of corneal topographic changes and surgically induced astigmatism after transconjunctival 27-gauge microincision vitrectomy surgery
International Ophthalmology (2018)
-
Long-term outcomes of sutureless 25-G+ pars-plana vitrectomy for the management of diabetic tractional retinal detachment
Graefe's Archive for Clinical and Experimental Ophthalmology (2017)
-
Comparative study of 27-gauge vs 25-gauge vitrectomy for epiretinal membrane
Eye (2016)
-
25-Gauge pars plana vitrectomy for ciliary block (malignant) glaucoma
International Ophthalmology (2015)
