
Abstract
Study design:
Functional outcome was evaluated following experimental compression-type spinal cord injury (SCI) in wild-type mice and knockout mice, lacking the inducible nitric oxide synthase (iNOS) gene.
Objectives:
To evaluate the role of the nitric oxide generating enzyme iNOS in SCI.
Methods:
The experimental animals were subjected to an extradural compression of the thoracic spinal cord. Functional outcome was studied during the first 2 weeks post-injury using a scoring system for assessment of hind limb motor function.
Results:
Injury resulted in initial paraplegia followed by gradual improvement of motor function in most cases. Mice lacking the iNOS gene (iNOS−/−) clearly tended to have a better functional outcome than wild-type mice. The difference was significant on day 14 after injury.
Conclusion:
In accordance with a few earlier experimental studies, showing beneficial effects of pharmacological iNOS inhibition, the present report would indicate a destructive influence of iNOS following spinal cord trauma.
Similar content being viewed by others


Introduction
In recent years nitric oxide (NO), one of the smallest endogenous biological mediators, has been shown to be involved in several physiological and pathological events in the central nervous system (CNS) as well as in other types of tissue. NO is synthesised by three known isoforms of nitric oxide synthase (NOS).1 There are two constitutive types of NOS, namely neuronal NOS (nNOS) and endothelial NOS (eNOS). A third isoform, inducible NOS (iNOS), is induced by inflammatory and other stimuli.
After experimental ischaemic and traumatic brain damage, there is a rapid and transient increase in the catalytic activity of constitutive NOS,2, 3 followed by induction of iNOS with some delay.4, 5 Based on the findings obtained with pharmacological inhibition of NOS or comparisons between NOS-deficient and wild-type mice, both protective3, 6 and harmful3, 4, 5 effects of NO in experimental CNS injury have been demonstrated.
Similar to other types of CNS injury, tissue levels of NO are rapidly elevated after spinal cord injury (SCI) in the rat, indicating early activation of constitutive NOS.7 In a later phase, iNOS is induced with the most robust increase 1 day after injury.7, 8 Immunohistochemical studies in rat models of SCI have shown postinjury iNOS immunoreactivity in several cell types, including neutrophils, macrophages, ependymal, endothelial and glial cells.8, 9 Administration of inhibitors of NOS to experimentally spinal cord-injured animals has been reported to improve,7, 8 worsen7 or have no effect on outcome measures.10 The seemingly conflicting effects of different NOS inhibitors implicate a complex role of NO in postinjury tissue reactions. We are interested in the pathophysiology of traumatic SCI. To elucidate the role of iNOS, we have evaluated the functional outcome following SCI in knockout mice, lacking the iNOS gene (iNOS−/−), and wild-type (iNOS+/+) animals.
Methods
A total number of 39 female mice between 13 and 15 weeks of age, weighing 19.3–24.1 g (mean 21.9±0.33) were used in this study. Of them, 20 were homozygously deficient in iNOS (C57BL/6-Nos2tm1Lau)11 and obtained from Jackson Laboratory, Bar Harbour, Maine, USA. In all, 19 age-matched C57BL/6J animals served as wild-type controls. At 1 day before injury, the animals were coded to avoid bias during surgery and functional evaluation. Food and water were provided ad libitum before and after the experiments. The mice were kept at a temperature of 20°C and exposed to alternate light/dark periods of 12 h. The study was approved by the Uppsala ethical committee for animal research.
Spinal cord compression trauma
We used a mouse model of spinal cord compression injury as described previously.12 Briefly, the animals were anaesthetised by a 0.6 ml intraperitoneal injection of a mixture of fluanisone (0.5 mg/ml) and midazolam (0.25 mg/ml) in distilled water. Laminectomy of Th7-8 vertebrae was performed, leaving the dura intact. Two adjustable forceps, connected to a stereotactic apparatus were then applied to the spinous processes of the vertebrae proximal and distal to the site of laminectomy to keep the vertebral column fixed. Injury was induced by gently applying a weight to the spinal cord through a plastic rod with a 2 × 1 mm flat end. In this study, a 20 g weight (10 g/mm2) was used. After 5 min of compression, the weight was removed and the wound was closed. The typical resulting histopathological signs of damage in this model of spinal cord injury are demonstrated in Figure 1.

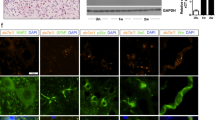
Microphotographs of spinal cords from intact controls (left panels) and experimental animals 14 days following spinal cord compression (right panels) showing the typical post-traumatic morphological changes. (a, b) Haematoxylin–eosin staining reveals extensive postinjury tissue damage, vacuolisation and gliosis. (c, d) Luxol fast blue-stained sections. Normally stained longitudinal, myelinated tracts can be seen in the control animal whereas most of the luxol-stained fibres are lost after the compression. (e, f) Neuronal damage demonstrated by MAP2 immunostaining (neuronal and dendritic marker). In normal grey matter numerous neurons and dendrites are immunostained. Note the extensive loss of immunostaining after injury. Only a few immunopositive profiles remain
As a majority of the animals develop transient urinary retention following this type of spinal cord trauma, bladder function was observed. In animals with palpable, distended bladder urine was expressed once a day by gentle compression of the abdomen.
Assessment of hind limb motor function
Hind limb motor function was evaluated before injury and on days 1, 2, 4, 7, 10 and 14 after injury, using a hind limb motor function scoring system (Table 1). First, animals were allowed to move freely on a paper covered mattress and were rated 0–8 according to the criteria presented in Table 1. Animals that had near normal or normal walking were tested further on steel bars (50 cm long and 3 mm thick) with decreasing widths: 2 cm, 1.5 cm, 1 cm, 7 mm and 5 mm. The mice were allowed to walk on the bars and the narrowest bar they could walk on without slipping in at least two trials was recorded.
Statistics
A nonparametric Mann–Whitney U-test was performed to compare functional outcome in the two experimental groups. Differences with a P-value <0.05 were considered statistically significant. Values in figures and text are presented as are presented as mean±SEM. Any statistically significant difference is denoted by (*).
Results
Immediately after injury there was an easily visible haemorrhagic lesion at the site of the compression. If not, injury was considered improper and the animal was excluded from the study. Seven mice had to be excluded due to improper injury or surgical mistakes. One animal died after induction of anaesthesia. Thus, 16 iNOS−/− and 15 wild-type mice were finally included in the functional evaluation.
Hind limb motor function
Before injury, all the animals had normal walking and could walk without slips on a 5 mm wide bar (hind limb motor function score 13). At day 1 after injury, most animals were paraplegic but during the subsequent 2 weeks there was normally a partial recovery of hind limb motor function.
As compared to wild-type mice, iNOS−/− animals clearly tended to have a better functional outcome after trauma (Figure 2). The difference was statistically significant on day 14 after injury (P=0.02).

Results of the functional evaluation. Hind limb motor function was evaluated on days 1, 2, 4, 7, 10 and 14 after SCI.* indicates significant difference between wild-type and iNOS−/− mice
Discussion
This study shows that mice lacking the iNOS gene have a better functional outcome than wild-types after spinal cord compression. As suggested by a few earlier studies, showing benefical effects of pharmacological inhibition of iNOS, the present report would indicate a mainly neurotoxic potential of iNOS-derived NO after SCI. To our knowledge, this is the first study evaluating the role of iNOS in spinal cord trauma using knockout mice.
Previously, Hamada and collaborators have demonstrated that repeated post-injury injections of the nonspecific NOS inhibitor L-NAME reduce motor disturbances after SCI in the rat, most likely due to inhibition of iNOS.7 In another rat study, administration of the relatively specific iNOS inhibitor aminoguanidine improved long-term functional outcome and reduced the size of the post-traumatic cavity.8 The present finding is consistent with these studies and also with the body of work describing a destructive role of iNOS in cerebral ischaemia and traumatic brain injury.
NO derived from iNOS catalytic activity may react with the superoxide anion to form peroxynitrite,9 a molecule that is associated with oxidative tissue damage13 and apoptotic neuronal death.14 In contrast to this, other investigators have shown that functional end points after controlled cortical impact brain trauma were significantly worsened if iNOS was pharmacologically inhibited or genetically deficient in experimental rats and mice, respectively.6 Based upon this finding, it was hypothesised that iNOS is a postinjury endogenous neuroprotectant. Neither the present, nor previous studies support a beneficial role of iNOS following spinal cord trauma.
There are several possible explanations for the conflicting reports of the role of NO and NO secreting enzymes in CNS injury. First, studies have suggested that changes in ambient redox milieu may switch the influence of NO from neurotoxicity to neuroprotection.15 Secondly, the role of NO seems to depend on the time of NO release and the cellular location of the NO-generating enzyme. Whereas previous studies on knockout mice in our laboratory indicate an involvement of nNOS in secondary damage after SCI,16 less is known about the influence of eNOS. In ischaemic CNS injury, however, eNOS is considered to be neuroprotective, based on the observation that eNOS−/− mice develop larger infarcts than wild types after experimental cerebral ischaemia.17 The finding that pretreatment with L-NAME before experimental SCI inhibits recovery of motor function, may therefore be attributed to inhibition of eNOS.7
Taken together, the role of NO in the secondary mechanisms after SCI seems to be complex but the present report supports ideas of a mainly destructive influence of iNOS-derived NO.
References
Nathan C, Xie Q . Nitric oxide synthases: roles, tolls and controls. Cell 1994; 78: 915–918.
Kader A, Frazzini V, Solomon R, Trifiletti R . Nitric oxide production during focal cerebral ischemia in rats. Stroke 1993; 24: 1709–1716.
Wada K, Chatzipanteli K, Busto R, Dietrich WD . Role of nitric oxide in traumatic brain injury in the rat. J Neurosurg 1998; 89: 807–818.
Iadecola C et al. Inducible nitric oxide synthase gene expression in vascular cells after transient focal cerebral ischemia. Stroke 1996; 27: 1373–1380.
Wada K et al. Inducible nitric oxide synthase expression after traumatic brain injury and neuroprotection with aminoguanidine treatment in rats. Neurosurgery 1998; 43: 1427–1436.
Sinz E et al. Inducible nitric oxide synthase is an endogenous neuroprotectant after traumatic brain injury in rats and mice. J Clin Invest 1999; 104: 647–656.
Hamada Y et al. Roles of nitric oxide in compression injury of rat spinal cord. Free Radic Biol Med 1996; 20: 1–9.
Chatzipanteli K et al. Temporal and segmental distribution of constitutive and inducible nitric oxide synthases after traumatic spinal cord injury: effect of aminoguanidine treatment. J Neurotrauma 2002; 19: 639–651.
Xu J et al. iNOS and nitrotyrosine expression after spinal cord injury. J Neurotrauma 2001; 18: 523–532.
Cohen T, Weinberg R, Blight A . Intrathecal infusion of the nitric oxide synthase inhibitor N-methyl L-arginine after experimental spinal cord injury in guinea pigs. J Neurotrauma 1996; 13: 361–369.
Laubach V, Shesely E, Smithies O, Sherman P . Mice lacking inducible nitric oxide synthase are not resistant to lipopolysaccharide-induced death. Proc Natl Acad Sci 1995; 92: 10688–10692.
Farooque M . Spinal cord compression injury in the mouse: presentation of a model including assessment of motor dysfunction. Acta Neuropathol 2000; 100: 13–22.
Beckman J et al. Apparent hydroxyl radical production by peroxinitrite: implications for endothelial injury from nitric oxide and superoxide. Proc Natl Acad Sci 1990; 87: 1620–1624.
Bonfoco E et al. Apoptosis and necrosis: two distinct events induced, respectively, by mild and intense insults with N-methyl-D-aspartate or nitric oxide/superoxide in cortical cell cultures. Proc Natl Acad Sci 1995; 92: 7162–7166.
Lipton S et al. A redox-based mechanism for the neuroprotective and neurodestructive effects of nitric oxide and related nitroso-compounds. Nature 1993; 364: 626–632.
Farooque M, Isaksson J, Olsson Y . Improved recovery after spinal cord injury in neuronal nitric oxide synthase-deficient mice but not in TNF-α-deficient mice. J Neurotrauma 2001; 18: 105–114.
Huang Z et al. Enlarged infarcts in endothelial nitric oxide synthase knockout mice are attenuated by nitro-L-arginine. J Cereb Blood Flow Metab 1996; 16: 981–987.
Acknowledgements
This work was supported by grants from the Swedish Association of Neurologically Disabled, Fredrik and Ingrid Thurings stiftelse, Tore Nilsons stiftelse, Åhléns stiftelse and Svenska Läkaresällskapet.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Isaksson, J., Farooque, M. & Olsson, Y. Improved functional outcome after spinal cord injury in iNOS-deficient mice. Spinal Cord 43, 167–170 (2005). https://doi.org/10.1038/sj.sc.3101672
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101672
Keywords
This article is cited by
-
α-Gal Nanoparticles in CNS Trauma: II. Immunomodulation Following Spinal Cord Injury (SCI) Improves Functional Outcomes
Tissue Engineering and Regenerative Medicine (2024)
-
Targeted siRNA delivery reduces nitric oxide mediated cell death after spinal cord injury
Journal of Nanobiotechnology (2017)
-
Genetic ablation of receptor for advanced glycation end products promotes functional recovery in mouse model of spinal cord injury
Molecular and Cellular Biochemistry (2014)
-
Distinct regulation of nNOS and iNOS by CB2 receptor in remote delayed neurodegeneration
Journal of Molecular Medicine (2012)
-
Significant correlation between cerebrospinal fluid nitric oxide concentrations and neurologic prognosis in incomplete cervical cord injury
European Spine Journal (2008)
