
Abstract
Objective:
To determine vitamin D and bone status in adolescent girls, pre-menopausal women and men of Pakistani origin, to single out determinants of vitamin D status and to determine the association between vitamin D status, bone metabolism and bone status.
Subjects/Methods:
Cross-sectional study, Copenhagen (55°N), January-November. Serum 25-hydroxyvitamin D (S-25OHD), serum intact parathyroid hormone (S-iPTH), bone turnover markers and whole body and lumbar spine bone mineral density were measured. Sun, smoking and clothing habits, age, body mass index (BMI), and vitamin D and calcium from food and from supplements were recorded. Thirty-seven girls (median age, range: 12.2 years, 10.1–14.7), 115 women (36.2 years, 18.1–52.7) and 95 men (38.3 years, 17.9–63.5) of Pakistani origin (immigrants or descendants with Pakistani parents) took part in the study.
Results:
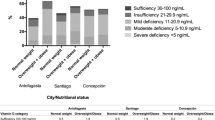
Median concentration of S-25OHD was 10.9, 12.0 and 20.7 nmol/l for girls, women and men, respectively. Forty-seven per cent of the girls, 37% of the women and 24% of the men had elevated S-iPTH, and there was a negative relationship between S-iPTH and S-25OHD. Use of vitamin D-containing supplements had a positive association with S-25OHD for men (P=0.04) and women (P=0.0008). Twenty-one per cent of the women and 34% of the men had osteopenia. Neither S-25OHD nor S-iPTH was associated with lumbar spine or whole body bone mineral content.
Conclusions:
Severely low vitamin D status and elevated S-iPTH is common among Pakistani immigrants in Denmark. The low vitamin D status is not associated with bone markers or bone mass among relatively young Pakistanis.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others

References
Alekel DL, Mortillaro E, Hussain EA, West B, Ahmed N, Peterson CT et al. (1999). Lifestyle and biologic contributors to proximal femur bone mineral density and hip axis length in two distinct ethnic groups of premenopausal women. Osteoporos Int 9, 327–338.
Alver K, Meyer HE, Falch JA, Sogaard AJ (2004). Bone mineral density in ethnic Norwegians and Pakistani immigrants. J Bone Miner Res 19, S159 (Abstract).
Andersen NL, Fagt S, Groth MV (1996). Danskernes kostvaner 1995 (Dietary habits of Danes 1995). Publication No. 235, Levnedsmiddelstyrelsen: Søborg, Denmark.
Andersen R, Mølgaard C, Skovgaard LT, Brot C, Cashman KD, Chabros E et al. (2005). Teenage girls and elderly women living in northern Europe have low winter vitamin D status. Eur J Clin Nutr 59, 533–541.
Arya V, Bhambri R, Godbole MM, Mithal A (2004). Vitamin D status and its relationship with bone mineral density in healthy Asian Indians. Osteoporos Int 15, 56–61.
Awumey EMK, Mitra DA, Hollis BW, Kumar R, Bell NH (1998). Vitamin D metabolism is altered in Asian Indians in the southern United States: a clinical research center study. J Clin Endocrin Metab 83, 169–173.
Binkley N, Krueger D, Cowgill CS, Plum L, Lake E, Hansen KE et al. (2004). Assay variation confounds the diagnosis of hypovitaminosis D: a call for standardization. J Clin Endocrin Metab 89, 3152–3157.
Brunvand L, Haug E (1993). Vitamin D deficiency amongst Pakistani women in Oslo. Acta Obestet Gynecol Scand 72, 264–268.
Carter GD, Carter R, Jones J, Berry J (2004). How accurate are assays for 25-hydroxyvitamin D? Data from the international vitamin D external quality assessment scheme. Clin Chem 50, 2195–2197.
Chapuy M-C, Preziosi P, Maamer M, Arnaud S, Galan P, Herberg S et al. (1997). Prevalence of vitamin D insufficiency in an adult normal population. Osteoporos Int 7, 439–443.
Christensen T (2001) Outline of GIES: General Intake Estimation System. Fourth International Food Data Conference: New Trends in the Management and Uses of Food Databases. 24–26 August 2001. Bratislava, Slovakia (poster).
Dawson-Hughes B (2004). Racial/ethnic considerations in making recommendations for vitamin D for adult and elderly men and women. Am J Clin Nutr 80S, 1763S–1766S.
Dawson-Hughes B, Heaney RP, Holick MF, Lips P, Meunier PJ, Vieth R (2005). Estimates of optimal vitamin D status. Osteoporos Int 16, 713–716.
Diamond TH, Levy S, Smith A, Day P (2002). High bone turnover in Muslim women with vitamin D deficiency. Med J Aust 177, 139–141.
Dunnigan MG, Paton JPJ, Haase S, McNicol GW, Gardner MD, Smith CM (1962). Late rickets and osteomalacia in the Pakistani community in Glasgow. Scot Med J 7, 159–167.
Falch JA, Steihaug S (2000). Vitamin D deficiency in Pakistani premenopausal women living in Norway is not associated with evidence of reduced skeletal strength. Scand J Clin Lab Invest 60, 103–110.
Finch PJ, Ang L, Eastwood JB, Maxwell JD (1992). Clinical and histological spectrum of osteomalacia among Asians in south London. Q J Med 83, 439–448.
Glerup H, Mikkelsen K, Poulsen L, Hass E, Overbeck S, Andersen H et al. (2000a). Hypovitaminosis D myopathy without biochemical signs of osteomalacic bone involvement. Calcif Tissue Int 66, 419–424.
Glerup H, Mikkelsen K, Poulsen L, Hass E, Overbeck S, Thomsen J et al. (2000b). Commonly recommended daily intake of vitamin D is not sufficient if sunlight exposure is limited. J Int Med 247, 260–268.
Heaney RP (2000). Vitamin D: how much do we need, and how much is too much? Osteoporos Int 11, 553–555.
Heaney RP (2003). Long-latency deficiency disease: insights from calcium and vitamin D. Am J Clin Nutr 78, 912–919.
Henderson JB, Dunnigan MG, McIntosh WB, Abdul-Motaal AA, Gettinby G, Glekin BM (1987). The importance of limited exposure to ultraviolet radiation and dietary factors in the aetiology of Asian rickets: a risk-factor model. Q J Med 63, 413–425.
Henriksen C, Brunvand L, Stoltenberg C, Trygg K, Haug E, Pedersen JI (1995). Diet and vitamin D status among pregnant Pakistani women in Oslo. Eur J Clin Nutr 49, 211–218.
Holick MF (2004). Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Am J Clin Nutr 80S, 1678S–1688S.
Hollis BW (2004). The determination of circulating 25-hydroxyvitamin D: no easy task. J Clin Endocrin Metab 89, 3149–3151.
Holvik K, Meyer HE, Falch JA, Søgaard AJ, Haug E (2004). The Oslo Health Study: biochemical markers of bone turnover and their relation to parathyroid hormone levels in persons of Pakistani and Norwegian origin living in Oslo. J Bone Min Res 19, S167 (Abstract).
Holvik K, Meyer HE, Haug E, Brunvand L (2005). Prevalence and predictors of vitamin D deficiency in five immigrant groups living in Oslo, Norway: the Oslo Immigrant Health Study. Eur J Clin Nutr 59, 57–63.
Hunt SP, O’Riordan JLH, Windo J, Truswell AS (1976). Vitamin D status in different subgroups of British Asians. BMJ 2, 1351–1354.
Jesudason D, Need AG, Horowitz M, O’Loughlin PD, Morris HA, Nordin BEC (2002). Relationship between serum 25-hydroxyvitamin D and bone resorption markers in vitamin D insufficiency. Bone 31, 626–630.
Lips P, Chapuy M-C, Dawson-Huges B, Pols HAP, Holick MF (1999). An international comparison of serum 25-hydroxyvitamin D measurements. Osteoporos Int 9, 394–397.
Meyer HE, Falch JA, Søgaard AJ, Haug E (2004). Vitamin D deficiency and secondary hyperparathyroidism and the association with bone mineral density in persons with Pakistani and Norwegian background living in Oslo, Norway, The Oslo Health Study. Bone 35, 412–417.
Nisbet J, Eastwood JB, Colston KW, Ang L, Flanagan AM, Chambers TJ et al. (1990). Detection of osteomalacia in British Asians: a comparison of clinical score with biochemical measurements. Clin Sci 78, 383–389.
Ovesen L, Andersen R, Jakobsen J (2003). Geographical differences in vitamin D status, with particular reference to European countries. Proc Nutr Soc 62, 813–821.
Prentice A, Parsons TJ, Cole TJ (1994). Uncritical use of bone mineral density in absorptiometry may lead to size-related artefacts in the identification of bone mineral determinants. Am J Clin Nutr 60, 837–843.
Rassouli A, Milanian I, Moslemi-Zaden M (2001). Determination of serum 25-hydroxyvitamin D3 levels in early postmenopausal Iranian women: relationship with bone mineral density. Bone 29, 428–430.
Roy DK, Berry JL, Pye SR, Adams JE, Swarbrich CM, King Y et al. (2007). Vitamin D status and bone mass in UK South Asian women. Bone 40, 200–204.
Sahota O, Masud T, San P, Hosking DJ (1999). Vitamin D insufficiency increases bone turnover markers and enhances bone loss at the hip in patients with established vertebral osteoporosis. Clin Endocrin 51, 217–221.
Serhan E, Holland M (2002). Relationship of hypovitaminosis D and secondary hyperparathyroidism with bone mineral density among UK resident Indo-Asians. Ann Rheum Dis 61, 456–458.
Solanki T, Hyatt RH, Kemm JR, Hughes EA, Cowan RA (1995). Are elderly Asians in Britain at a high risk of vitamin D deficiency and osteomalacia? Age Ageing 24, 103–107.
Statistics Denmark, Statbank (2005): http://www.dst.dkBEF3: Population by area, age, sex, country of origin and citizenship (1980–2005).
Zittermann A (2003). Vitamin D in preventive medicine: are we ignoring the evidence? Br J Nutr 89, 552–572.
Acknowledgements
We acknowledge Karin Hess Ygil, Dorte Strange and Nighat Kwajada for interviewing the participants. Nighat Kwajada is acknowledged for the blood sampling and the interpretation into Urdu when necessary. Dorte Strange is acknowledged for the DXA scannings. Birgitte Hermansen is acknowledged for assisting the DXA-scannings and assisting designing the FFQ. Karin Hess Ygil, Tue Christensen and Anders Møller are acknowledged for the dietary intake calculations. The study was part of the OPTIFORD-project ‘Towards a strategy for optimal vitamin D fortification’, financed by EU, the Fifth Framework Programme (QLK1-CT-2000-00623).
Author information
Authors and Affiliations
Corresponding author
Additional information
Guarantor: R Andersen.
Contributors: RA collected the data, wrote the manuscript and undertook the statistical analyses with advice from LTS, CM and LO. RA, CB, KDC, CL-A, CM and LO designed the study. JJ undertook the measurements of S-25OHD. KDC undertook the measurements of bone turnover markers. CL-A undertook the measurements of S-iPTH, calcium and phosphate. All contributed to the manuscript.
Rights and permissions
About this article
Cite this article
Andersen, R., Mølgaard, C., Skovgaard, L. et al. Pakistani immigrant children and adults in Denmark have severely low vitamin D status. Eur J Clin Nutr 62, 625–634 (2008). https://doi.org/10.1038/sj.ejcn.1602753
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ejcn.1602753
Keywords
This article is cited by
-
Low vitamin D in dark-skinned immigrants is mainly due to clothing habits and low UVR exposure: a Danish observational study
Photochemical & Photobiological Sciences (2021)
-
Increased calcium intake is associated lower serum 25-hydroxyvitamin D levels in subjects with adequate vitamin D intake: a population-based observational study
BMC Nutrition (2020)
-
Vitamin D-fortified foods improve wintertime vitamin D status in women of Danish and Pakistani origin living in Denmark: a randomized controlled trial
European Journal of Nutrition (2020)
-
Effect of vitamin D fortified foods on bone markers and muscle strength in women of Pakistani and Danish origin living in Denmark: a randomised controlled trial
Nutrition Journal (2019)
-
Differences in the dietary requirement for vitamin D among Caucasian and East African women at Northern latitude
European Journal of Nutrition (2019)
