
Abstract
Background:
Fetal growth abnormalities in hypoplastic left heart syndrome (HLHS) have been documented primarily by birth measurements. Fetal growth trajectory has not been described. We hypothesized that fetal growth trajectory declines across late gestation in this population.
Methods:
Infants with a prenatal diagnosis of HLHS and no history of prematurity or a genetic syndrome were identified. Fetal ultrasound measurements and birth anthropometrics were obtained from clinical records. z-Scores for estimated fetal weight (EFWz) and birth weight (BWTz) were compared. BWTz for three neonatal standards were compared.
Results:
Paired fetal and neonatal data were identified in 33 cases of HLHS. Mean gestational age at ultrasound and birth were 27 and 38 wk, respectively. BWTz was lower than EFWz by a mean of 0.82 (SD: 0.72, P < 0.0001), with 64% of subjects demonstrating a decrease in z-score of >0.5. Umbilical artery (UA) Doppler found no evidence of significant placental insufficiency. Modest differences in BWTz were seen across BWT standards in this cohort.
Conclusion:
The majority of fetuses with HLHS demonstrate decreased growth velocity during later pregnancy, suggesting growth abnormalities manifest in utero. The potential relationship to future clinical outcomes warrants further study.
Similar content being viewed by others


Main
Birth weight (BWT) is a critical predictor of outcome in infants with cardiovascular malformations (CVMs), especially those with hypoplastic left heart syndrome (HLHS). Infants who are either small for gestational age (<10th percentile) or low BWT (<2.5 kg) are at greater risk of death and complications following cardiac surgery (1,2). Such infants also appear to be at greater risk of the long-term neurodevelopmental morbidities that are increasingly apparent in survivors (3). Unfortunately, the incidence of low BWT appears to be greater in infants with HLHS as compared with the general population (4). This observation is complicated by the association between CVM and prematurity (5). Fetal somatic growth in this population is poorly understood.
BWT is a complex multifactorial trait that is influenced by genetic (6,7) and environmental factors (8). As a single measurement in time, it is a useful summary of the fetal growth preceding delivery. The relationship between growth and clinical outcomes can be further refined through an understanding of the pattern or trajectory of intrauterine growth across gestation (9). Serial measurements, obtained noninvasively by ultrasound, may be used to identify differential growth patterns, which may influence both short and long-term clinical outcomes (10). These patterns have not been described in the fetus with HLHS.
The fetal growth standards used for clinical assessment of the pregnancy also refine the interpretation of BWT as a clinical and research outcome. Such standards have been described using two methods: computational estimates derived from ultrasound measurements (11,12) and direct measurement of live-born infants across the range of viable gestational ages (13,14,15). Both approaches highlight that gestational age is a major determinant of growth and therefore adjust for gestational age when establishing norms. By contrast, standards from the Centers for Disease Control and Prevention (CDC) (16) and the World Health Organization (WHO) (17) were designed to assess BWT and growth in healthy term infants (born 37–42 wk gestation) and children, and therefore do not adjust for gestational age. These distinctions may be important in populations with high rates of prematurity and growth restriction, such as infants with HLHS. Different standards of fetal growth have not been compared in individuals with CVMs.
As such, the aims of this study are (i) to determine fetal growth trajectory in subjects with HLHS, (ii) to determine the proportion of HLHS subjects who demonstrate poor somatic growth in utero, and (iii) to compare different reference standards at both fetal and neonatal time points. We hypothesize that the fetus with HLHS will demonstrate a decreasing growth trajectory from midgestation to birth and that the magnitude of the decline will be influenced by the standard used.
Results
Study Population
A fetal diagnosis of HLHS, fetal biometry measurements, and postnatal birth anthropometrics were available in 33 cases. Characteristics of the cohort are summarized in Table 1 .
Trajectory of Weight z-Score Decreases From Fetal Ultrasound to Birth
Fetal biometry was measured at a median of 27 wk gestation whereas neonatal anthropometrics were measured at a median of 38 wk. Using the Olsen standard for both measurements, gestational age–adjusted z-score for BWT (BWTz) was lower than gestational age–adjusted z-score for estimated fetal weight (EFWz) by a mean of 0.82 (SD: 0.72, P < 0.0001, Figure 1 ). The change in z-score between time points was not associated with gestational age at ultrasound (r: −0.22, P = 0.21) or the duration of time between studies (r: 0.22, P = 0.21). However, using the Hadlock standard for EFWz and the Olsen standard for BWTz showed that BWTz was significantly lower than EFWz by a mean of 0.32 (SD: 0.73, P = 0.02).

Comparison of EFWz and BWTz using the Olsen standard (ref. 14). If the decrease in z-score is >0.5, EFWz (open circles) and BWTz (solid circles) are connected by a solid line. Otherwise, they are connected by a dashed line. BWTz, z-score for estimated birth weight; EFWz, z-score for estimated fetal weight.
The Majority of Subjects Demonstrate Poor Fetal Growth In Utero
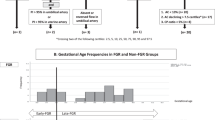
Poor fetal growth, as defined by a decrease of ≥0.5 between EFWz and BWTz, was seen in 64% of subjects. Only 6% (two subjects) demonstrated a BWTz that was greater than the EFWz. Umbilical artery (UA) Doppler resistance index was available in 19 of 33 cases, and no evidence of placental insufficiency was identified in those cases, suggesting normal maternal health and adequate nutritional status.
Gestational Age–Adjusted Standards Differ When Based on Fetal Ultrasound Measurements Vs. Neonatal Anthropometrics
The EFWz calculated by the Olsen standard was significantly increased as compared with EFWz calculated by the Hadlock standard (mean: 0.51, P = 0.0014). The Bland–Altman plot demonstrates that the majority of fetuses had a lower EFWz as calculated by the Hadlock method ( Figure 2 ).

Comparison of EFWz using the Hadlock standard (ref. 30) and the Olsen standard (ref. 14). The Bland–Altman plot shows the difference between the z-scores from the two standards against the average of the z-scores from the two standards. The solid horizontal line corresponds to the zero difference between the z-scores from the two standards, which is the ideal situation. The three dashed horizontal lines are the actual mean differences between the z-scores (middle dashed line) and 1.96 times the SDs from the mean difference (upper and lower dashed lines). EFWz, z-score for estimated fetal weight.
WHO, CDC, and Olsen Standards Demonstrate Modest Differences in BWT z-Scores
The correlations of BWTz among the WHO, CDC, and Olsen methods were generally high (WHO–CDC: 0.99; WHO–Olsen: 0.90; CDC–Olsen: 0.9). However, pairwise comparisons of BWTz demonstrated significant differences for WHO–CDC and CDC–Olsen comparisons ( Table 2 ). Head circumference z-score correlations were also generally high (WHO–CDC: 0.97; WHO–Olsen: 0.72; CDC–Olsen: 0.82), but a significant difference was noted in the CDC–Olsen pairwise comparison. Bland–Altman plots for the comparison of weight methods demonstrate no distinct pattern in the distribution of the difference between WHO and Olsen ( Figure 3b ). For smaller newborns (BWTz: <−1), WHO z-scores were lower than CDC z-scores ( Figure 3a ). For those with BWTz ≥−1, WHO z-scores were higher. For most newborns, CDC z-scores were lower than Olsen z-scores ( Figure 3c ). Head circumference patterns were similar ( Figure 3d – f ).

Comparison of z-scores from different standards. (a) Comparison of BWTz values from the WHO (ref. 17) and CDC standards (ref. 16). (b) Comparison of BWTz values from the WHO and Olsen (ref. 14) standards. (c) Comparison of BWTz values from the CDC and Olsen standards. (d) Comparison of birth head circumference z-scores from the WHO and CDC standards. (e) Comparison of birth head circumference z-scores from the WHO and Olsen standards. (f) Comparison of birth head circumference z-scores from the CDC and Olsen standards. The Bland–Altman plots show the difference between the z-scores against the average of the z-scores. BWTz, z-score for estimated birth weight; CDC, Centers for Disease Control and Prevention; WHO, World Health Organization.
Discussion
This study demonstrates that growth trajectory declines from midgestation to birth in the fetus with HLHS. A threshold decrease in z-score of ≥0.5 identified poor growth in 64% of subjects. Of note, the choice of growth standard can influence the magnitude, although not the direction, of these findings.
The growth abnormalities in the fetuses with HLHS result in a population of neonates who are, on average, smaller than expected for gestational age and may have growth abnormalities in the context of even “normal” BWT. Given the importance of BWT (1,2) and gestational age (18,19) as predictors of clinical outcome in CVMs, the observation is important. However, the fetal growth patterns underlying these BWT observations are largely unknown and may influence short- and long-term neurodevelopmental outcomes (10). Both somatic growth and brain growth (20,21) may be adversely effected in HLHS. These findings likely make important contributions to the neurodevelopmental outcomes that are now a major focus of the field (22).
The observation of a declining growth trajectory in later pregnancy may suggest a suboptimal energy balance. Although the available UA resistance index results did not identify definitive placental insufficiency, vascular pathology in the placenta could lead to reduced substrate delivery that is not detectable by current clinical testing. It is also possible that, despite oxygen delivery via the maternal–fetal circulation and compensatory mechanisms within the central nervous system (23), the fetus with HLHS is subject to metabolic inefficiencies of hypoxia, particularly in the brain (24). Cerebral hypoxia is one potential explanation for the well-described reduction in head and brain size associated with HLHS and may contribute to subsequent adverse clinical outcomes (25).
An improved understanding of fetal growth trajectory may also facilitate clinical decision making by the medical team that is monitoring the pregnancy. These results inform antenatal testing in the nearly 75% of HLHS cases that are identified by prenatal diagnosis. It appears that some decline in growth trajectory occurs in the vast majority of fetuses with HLHS. For a given fetus with HLHS and decelerating growth on ultrasound, the observation may not confer the same risk of fetal death as primary placental pathology. Given the apparent benefits of even small increases in BWT and gestational age in the neonate with HLHS, the risk–benefit balance of scheduled deliveries favors waiting until at least 39, if not 40 wk. In addition, a closer inspection of placental pathology and growth abnormalities is warranted.
The importance of methodology and reference standards is critical to understanding the magnitude of the growth problem (26). Differences between ultrasound measurements of the fetus in utero and measurements of the live-born premature infant are well described (27). These differences appear to vary when there is suspected macrosomia or growth restriction (28). To date, there are no standards that reconcile high-quality ultrasound measures with neonatal anthropometric reference values in the same population. Our findings of reduced growth velocity persist with all three standards examined in this study. However, it should be noted that the observation of decreased growth trajectory is attenuated when the EFW is referenced to ultrasound standard values. Researchers should be aware of these differences when categorizing BWT in neonates with CVMs.
The recent introduction of WHO growth standards may result in reclassification of some infants who are at the lower end of the growth curve (“low normal” to small for gestational age). There are several methodological differences between the WHO and CDC standards (26). These differences include characteristics of the population, intervals of measurement, and statistical analyses. Differences may be magnified at the lower BWTs that are common in HLHS. Furthermore, the lower gestational age of many newborns with HLHS must be considered. The Olsen standard was specifically chosen to incorporate gestational age. These differences were most apparent when comparing Olsen values to the CDC standard values. Our cohort suggests that the WHO and Olsen standards function quite similarly for neonates born at 37 wk gestation or greater with HLHS.
This study has several limitations. The cohort probably represents a “best-case scenario” for patients with HLHS because high-risk subsets were excluded. This may limit the generalizability of the findings. However, by excluding premature infants and infants with genetic syndromes, the cohort allows for an assessment of fetal growth pattern that attempts to isolate the role of structural heart disease while minimizing the confounding influences of maternal disease and extracardiac anomalies. In addition, all ultrasound measurements were obtained during routine clinical care. The variability of such measurements may influence the results but would likely underestimate the true differences, therefore minimizing the risk of a type I error. Assessment of placental function was limited to UA Doppler in a subset of the subjects. More detailed assessment of fetal and uterine flow patterns may provide further insights. Finally, the cohort is underpowered to perform subgroup comparisons such as between HLHS phenotypes (e.g., aortic stenosis vs. aortic atresia).
In summary, a large proportion of fetuses with HLHS demonstrate decreased growth velocity during later pregnancy, which appears unrelated to placental function. The resulting lower BWTs in this population illustrate the importance of using gestational age–adjusted reference standards. Our results provide evidence that growth problems associated with HLHS manifest in utero and warrant careful examination of somatic growth in the fetus. Elucidating different patterns of fetal growth in HLHS may inform outcomes and create opportunities for new prenatal therapies.
Methods
Study Population
Infants born following prenatal diagnosis of HLHS between January 1998 and June 2010 were identified from databases within the Heart Institute at Cincinnati Children’s Hospital Medical Center. HLHS was strictly defined as atresia or stenosis of the aortic and mitral valves, and hypoplasia of the left ventricle and ascending aorta (21). All patients had intact ventricular septa and normally related great arteries. Exclusion criteria included known genetic syndromes (e.g., Turner Syndrome), prematurity (<37 wk gestation), and multiple-gestation pregnancies. The institutional review board at Cincinnati Children’s Hospital Medical Center approved this study with waiver of consent for the collection of de-identified data from existing medical records.
Ultrasound and Neonatal Measurements
Fetal biometry and anthropometrics were assessed using the earliest available obstetric ultrasound reports and the Hadlock standard (29,30). Head circumference, EFW, and gestational age data were collected. Neonatal anthropometrics included BWT, length, and head circumference. Fetal and newborn z-scores were evaluated using the Olsen standard, a contemporary reference based on growth curves derived from a large, racially diverse US sample adjusted for gestational age and gender (14). Newborn z-scores were also evaluated using CDC (16) and WHO standards (17). Intrauterine growth restriction was defined as an EFW ≤10th percentile. Small for gestational age was defined as BWT ≤10th percentile. Low BWT was considered <2,500 g. Poor weight gain and poor head growth were defined as decreases in weight and head circumference z-score, respectively, greater than 0.5 (31) from midgestation to birth.
Echocardiographic Data
Diagnosis of HLHS was confirmed by neonatal echocardiogram following prenatal diagnosis. Fetal echocardiograms were performed on either Sequoia C512 (Siemens, Mountain View, CA) or Vivid 7 (General Electric, Milwaukee, WI) ultrasound systems with either a 2–6 MHz curvilinear or 3–5 MHz phased array transducer. Complete two-dimensional, color flow, and spectral Doppler studies were performed according to accepted standards (32). In recent years, Doppler profiles of the UA were performed routinely as a part of clinical care. This information is available for a subset of the cohort. When performed, the peak systolic, end diastolic, and mean velocities were measured offline to calculate the resistance index. All measurements were performed in triplicate and averaged to take into account beat-to-beat variation.
Statistical Analysis
Descriptive characteristics are presented as frequencies and proportions, mean ± SD, and medians with interquartile ranges where appropriate. The EFWz and the BWTz were compared using paired t-tests. Correlation of z-score change and gestational age at the time of ultrasound were assessed by Pearson correlation coefficient. Pairwise comparisons of z-scores based on the Hadlock, Olsen, and CDC standards were performed using paired t-tests. Considering three pairs of comparisons, P < 0.017 was considered statistically significant using Bonferroni adjustment of 0.05 type I error. Bland–Altman plots were constructed by plotting the difference between two methods vs. the average of two methods. For all other comparisons, the experiment-wise error rate was set at the nominal (α = 0.05) level.
Statement of Financial Support
This project was supported by a Summer Undergraduate Research Fellowship (to P.T.H.) and National Institutes of Health grant HL085122 (to R.B.H.).
References
Curzon CL, Milford-Beland S, Li JS, et al. Cardiac surgery in infants with low birth weight is associated with increased mortality: analysis of the Society of Thoracic Surgeons Congenital Heart Database. J Thorac Cardiovasc Surg 2008;135:546–51.
Karamlou T, McCrindle BW, Blackstone EH, et al. Lesion-specific outcomes in neonates undergoing congenital heart surgery are related predominantly to patient and management factors rather than institution or surgeon experience: A Congenital Heart Surgeons Society Study. J Thorac Cardiovasc Surg 2010;139:569–77 e1.
Gaynor JW, Wernovsky G, Jarvik GP, et al. Patient characteristics are important determinants of neurodevelopmental outcome at one year of age after neonatal and infant cardiac surgery. J Thorac Cardiovasc Surg 2007;133:1344–53, 1353.e1–3.
Atz AM, Travison TG, Williams IA, et al.; Pediatric Heart Network Investigators. Prenatal diagnosis and risk factors for preoperative death in neonates with single right ventricle and systemic outflow obstruction: screening data from the Pediatric Heart Network Single Ventricle Reconstruction Trial(*). J Thorac Cardiovasc Surg 2010;140:1245–50.
Williams RV, Ravishankar C, Zak V, et al.; Pediatric Heart Network Investigators. Birth weight and prematurity in infants with single ventricle physiology: pediatric heart network infant single ventricle trial screened population. Congenit Heart Dis 2010;5:96–103.
Freathy RM, Mook-Kanamori DO, Sovio U, et al.; Genetic Investigation of ANthropometric Traits (GIANT) Consortium; Meta-Analyses of Glucose and Insulin-related traits Consortium; Wellcome Trust Case Control Consortium; Early Growth Genetics (EGG) Consortium. Variants in ADCY5 and near CCNL1 are associated with fetal growth and birth weight. Nat Genet 2010;42:430–5.
Knight B, Shields BM, Turner M, Powell RJ, Yajnik CS, Hattersley AT . Evidence of genetic regulation of fetal longitudinal growth. Early Hum Dev 2005;81:823–31.
Blumenshine P, Egerter S, Barclay CJ, Cubbin C, Braveman PA . Socioeconomic disparities in adverse birth outcomes: a systematic review. Am J Prev Med 2010;39:263–72.
Bloomfield FH, Oliver MH, Harding JE . The late effects of fetal growth patterns. Arch Dis Child Fetal Neonatal Ed 2006;91:F299–304.
van Batenburg-Eddes T, de Groot L, Steegers EA, et al. Fetal programming of infant neuromotor development: the generation R study. Pediatr Res 2010;67:132–7.
Verburg BO, Steegers EA, De Ridder M, et al. New charts for ultrasound dating of pregnancy and assessment of fetal growth: longitudinal data from a population-based cohort study. Ultrasound Obstet Gynecol 2008;31:388–96.
Marsál K, Persson PH, Larsen T, Lilja H, Selbing A, Sultan B . Intrauterine growth curves based on ultrasonically estimated foetal weights. Acta Paediatr 1996;85:843–8.
Oken E, Kleinman KP, Rich-Edwards J, Gillman MW . A nearly continuous measure of birth weight for gestational age using a United States national reference. BMC Pediatr 2003;3:6.
Olsen IE, Groveman SA, Lawson ML, Clark RH, Zemel BS . New intrauterine growth curves based on United States data. Pediatrics 2010;125:e214–24.
Alexander GR, Himes JH, Kaufman RB, Mor J, Kogan M . A United States national reference for fetal growth. Obstet Gynecol 1996;87:163–8.
Kuczmarski RJ, Ogden CL, Guo SS, et al. 2000 CDC Growth Charts for the United States: methods and development. Vital Health Stat 11 2002;246:1–190.
de Onis M, Garza C, Victora CG, Onyango AW, Frongillo EA, Martines J . The WHO Multicentre Growth Reference Study: planning, study design, and methodology. Food Nutr Bull 2004;25:Suppl 1:S15–26.
Cnota JF, Gupta R, Michelfelder EC, Ittenbach RF . Congenital heart disease infant death rates decrease as gestational age advances from 34 to 40 weeks. J Pediatr 2011;159:761–5.
Costello JM, Polito A, Brown DW, et al. Birth before 39 weeks’ gestation is associated with worse outcomes in neonates with heart disease. Pediatrics 2010;126:277–84.
Shillingford AJ, Ittenbach RF, Marino BS, et al. Aortic morphometry and microcephaly in hypoplastic left heart syndrome. Cardiol Young 2007;17:189–95.
Hinton RB, Andelfinger G, Sekar P, et al. Prenatal head growth and white matter injury in hypoplastic left heart syndrome. Pediatr Res 2008;64:364–9.
Barbu D, Mert I, Kruger M, Bahado-Singh RO . Evidence of fetal central nervous system injury in isolated congenital heart defects: microcephaly at birth. Am J Obstet Gynecol 2009;201:43.e1–7.
Donofrio MT, Bremer YA, Schieken RM, et al. Autoregulation of cerebral blood flow in fetuses with congenital heart disease: the brain sparing effect. Pediatr Cardiol 2003;24:436–43.
Berg C, Gembruch O, Gembruch U, Geipel A . Doppler indices of the middle cerebral artery in fetuses with cardiac defects theoretically associated with impaired cerebral oxygen delivery in utero: is there a brain-sparing effect? Ultrasound Obstet Gynecol 2009;34:666–72.
Hangge PT, Cnota JF, Woo JG, et al. Microcephaly is associated with early adverse neurologic outcomes in hypoplastic left heart syndrome. Pediatr Res 2013; e-pub ahead of print 10 April 2013.
de Onis M, Garza C, Onyango AW, Borghi E . Comparison of the WHO child growth standards and the CDC 2000 growth charts. J Nutr 2007;137:144–8.
Fry AG, Bernstein IM, Badger GJ . Comparison of fetal growth estimates based on birth weight and ultrasound references. J Matern Fetal Neonatal Med 2002;12:247–52.
Ben-Haroush A, Yogev Y, Bar J, et al. Accuracy of sonographically estimated fetal weight in 840 women with different pregnancy complications prior to induction of labor. Ultrasound Obstet Gynecol 2004;23:172–6.
Hadlock FP, Harrist RB, Carpenter RJ, Deter RL, Park SK . Sonographic estimation of fetal weight. The value of femur length in addition to head and abdomen measurements. Radiology 1984;150:535–40.
Hadlock FP, Harrist RB, Sharman RS, Deter RL, Park SK . Estimation of fetal weight with the use of head, body, and femur measurements–a prospective study. Am J Obstet Gynecol 1985;151:333–7.
Burnham N, Ittenbach RF, Stallings VA, et al. Genetic factors are important determinants of impaired growth after infant cardiac surgery. J Thorac Cardiovasc Surg 2010;140:144–9.
Rychik J, Ayres N, Cuneo B, et al. American Society of Echocardiography guidelines and standards for performance of the fetal echocardiogram. J Am Soc Echocardiogr 2004;17:803–10.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cnota, J., Hangge, P., Wang, Y. et al. Somatic growth trajectory in the fetus with hypoplastic left heart syndrome. Pediatr Res 74, 284–289 (2013). https://doi.org/10.1038/pr.2013.100
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pr.2013.100
This article is cited by
-
Application of the INTERGROWTH-21st chart compared to customized growth charts in fetuses with left heart obstruction: late trimester biometry, cerebroplacental hemodynamics and perinatal outcome
Archives of Gynecology and Obstetrics (2019)
-
Fetal somatic growth trajectory differs by type of congenital heart disease
Pediatric Research (2018)
-
In Utero Evidence of Impaired Somatic Growth in Hypoplastic Left Heart Syndrome
Pediatric Cardiology (2017)
