
Abstract
Aim:
To investigate the SLCO1B1 388A>G and 521T>C polymorphisms in hyperlipidemia patients and evaluate the effect of the two polymorphisms on the lipid-lowering efficacy of pitavastatin.
Methods:
The functional polymorphisms of SLCO1B1 (388A>G and 521T>C) were genotyped in 140 Chinese patients with essential hyperlipidemia using polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) and one-step tetra-primers ARMS-PCR. Eighty-five patients were enrolled in the clinical trial and given 2 mg of pitavastatin daily for 8 weeks. Total cholesterol (TC), triglyceride (TG), high-density lipoprotein (HDL), and low-density lipoprotein (LDL) serum levels were measured at baseline, after 4 weeks and after 8 weeks of treatment.
Results:
The allele frequencies of SLCO1B1 388A>G and 521T>C in essential hyperlipidemia patients were 71.1% and 11.1%, respectively. The 4- and 8-week treatment with pitavastatin significantly reduced TC, TG, and LDL levels, but there was no statistical difference among patients with wild type, SLCO1B1 388A>G or SLCO1B1 521T>C in the lipid-lowering efficacy of pitavastatin.
Conclusion:
The present study found that the allele frequencies of SLCO1B1 388A>G and 521T>C in Chinese patients with essential hyperlipidemia are comparable to those in healthy Chinese population. SLCO1B1 388A>G and 521T>C do not affect the lipid-lowering efficacy of pitavastatin.
Similar content being viewed by others


Introduction
The organic anion transporting polypeptide 1B1 (OATP1B1, also known as OATP-C, OATP2, and LST-1), exclusively expressed in the basolateral membrane of hepatocytes1 is an important transporter of the OATP family, which contributes to the hepatic uptake of many endogenous and xenobiotic compounds including bile acids, sulfate and glucuronide conjugates, thyroid hormones, peptides and drugs such as pravastatin, pitavastatin, methotrexate and rifampin2.
The highly polymorphic gene SLCO1B1 encodes OATP1B1: to date, more than 20 single nucleotide polymorphisms (SNPs) have been identified, some of which are associated with altered function. SLCO1B1 388A>G (Asn130Asp) and 521T>C (Val174Ala) are common variants and have altered transport activities in vitro. In addition, cumulative evidence indicates that SLCO1B1 polymorphisms can significantly affect the pharmacokinetics of statins.
Pitavastatin (p-INN) is a novel synthetic 3-hydroxy-3-methylglutaryl coenzyme A reductase (HMG-CoA) inhibitor. It has a stronger hypolipidemic profile and a safer profile than other statins, and may be a better choice for treatment of hypercholesterolemic patients3. In vivo, pitavastatin is scarcely metabolized by cytochrome P450 2C9 and undergoes reversible lactonization3, 4. OATP1B1 is a transporter in the liver and plays an important role in the distribution of pitavastatin5. Some research6, 7, 8 indicates that SLCO1B1 polymorphisms have significant effects on the pharmacokinetics of pitavastatin. The dose-normalized area under the plasma concentration–time curve (AUC) and peak plasma concentration (Cmax) values of pitavastatin in heterozygous subjects of SLCO1B1 *15 (388A>G and 521T>C) or 521T>C were 1.4- and 1.8-fold higher, respectively, than in subjects without these SNPs7. SLCO1B1 polymorphisms had greater effects on the pharmacokinetic parameters of pitavastatin than those previously reported in pravastatin8. In addition, recent studies9, 10, 11, 12 reported that SLCO1B1 polymorphisms were associated with the lipid-lowering response to HMG-CoA inhibitors and adverse effects of simvastatin and irinotecan. The present study was conducted to investigate the contribution of the SLCO1B1 388A>G and 521T>C polymorphisms to inter-individual response to pitavastatin in Chinese primary hyperlipidemia patients.
Materials and methods
Subjects
We genotyped 140 Chinese primary hyperlipidemia patients with total cholesterol (TC)≥5.72 mmol/L, triglyceride (TG)≥1.70 mmol/L, or high-density lipoprotein cholesterol (HDL-c)≤ 0.91 mmol/L after dietary intervention: 85 of those patients (ages 18–70) with varying genotypes were enrolled in this clinical trial. Exclusion criteria were as follows: hyperlipidemia caused by drugs or other causes, previous hypersensitivity to statins or other drugs, severe impairment of renal or/and hepatic function, history of thyroid hypofunction, history of mental illness, history of acute myocardial infarction, cerebrovascular accident, or myopathy, and treatment with other drugs (eg cyclosporin) that may increase the risk of toxic response to pitavastatin. Patients currently receiving treatment with lipid-regulating drugs were eligible to participate in the clinical trial after a 2-week washout period. This study was approved by the Ethics Committee of the Third Xiangya Hospital of Central South University. All subjects were informed of the detailed protocol of the clinical trial and gave their informed consent.
Clinical trial protocol
Subjects were treated with 2 mg of pitavastatin once daily after supper for 8 weeks. TC, TG, HDL, and low-density lipoprotein (LDL) plasma concentrations were determined at 0, 4, and 8 weeks of treatment. Vital signs, hepatic function, renal function, creatine kinase levels, fasting blood glucose levels and adverse events were monitored in safety evaluations.
Genotyping
Venous blood (5 mL) was collected from patients in a sterile tube containing EDTA and stored at 4 °C. Genomic DNA was extracted by the QIAamp whole blood mini kit (Qiagen) following the manufacturer's instructions. Polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) was performed for 388G>A genotyping, and an amplification refractory mutation system (ARMS-PCR) was used for 521T>C genotyping as previously described13.
Statistical analysis
Genotype frequencies of SLCO1B1 388G>A and 521T>C were assessed for deviation from Hardy-Weinberg equilibrium using the χ2-test of goodness-of-fit. Differences between lipid parameters before and after pitavastatin treatment were tested using the paired t-test. Potential differences in drug response among the genotypes were tested using a one-way analysis of variance (ANOVA). The statistical significance level was defined as a P-value of less than 0.05 and statistical calculations were performed using the SPSS software (SPSS 11.0 for Windows; SPSS Inc, Chicago, IL).
Results
Allelic frequencies of SLCO1B1 SNPs
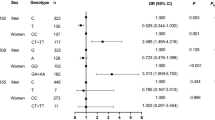
In the 140 Chinese hypercholesterolemic subjects, there were 57 (40.7%) heterozygotes and 71 (50.7%) homozygotes for the 388A>G mutation, and 27 (19.3%) heterozygotes and 2 (1.4%) homozygotes for the 521T>C mutation. The frequencies of the alleles and genotypes are listed in Table 1. The distribution of the genotypes of the 388G>A and 521T>C polymorphisms conformed to predictions of Hardy-Weinberg equilibrium (P>0.05).
Association of SLCO1B1 polymorphisms with pharmacodynamics of pitavastatin
Subjects (41 males, 44 females) of the Han population were enrolled in and finished the clinical trial. The mean (±SD) age was 56±9 years and the mean (±SD) BMI was 24.85±2.73 kg/m2. Our study showed that 4- and 8-week treatment with pitavastatin significantly reduced TC, TG, and LDL cholesterol plasma levels (P<0.05). However, the pitavastatin treatment did not affect the level of HDL cholesterol (P>0.05). Plasma lipid parameters of patients before treatment and after 4 and 8 weeks of pitavastatin treatment are listed in Table 2 and 3. There was no difference in age, sex, BMI, and lipid parameters before treatment among different genotypes, and after 4 and 8 weeks of treatment, serum lipid parameters did not show statistical difference among various genotype groups.
Discussion
SLCO1B1 is a newly identified transporter with functional genetic polymorphisms. Based on the functional variability of OATP1B1 and its broad range of substrates, SNPs in SLCO1B1 may play an important role in pharmacology and toxicology. One such polymorphism, 521T>C, has been consistently associated with altered transport activity both in vitro14, 15 and in vivo7, 8, 9, 16, 17, 18 though results regarding the 388G>A variant are contradictory14, 15, 19, 20. In the present study, the allele frequencies of 521C (11.1%) and 388A (71.1%) in Chinese primary hyperlipidemia patients were similar to those previously reported in healthy Chinese populations13. These results indicate that SLCO1B1 388G>A and 521T>C variants are not associated with primary hyperlipidemia, although SLCO1B1 has been reported to be involved in the transportation of cholesterol and statins.
Recent studies7, 8, 9, 21, 22, 23, 24 consistently showed SLCO1B1 variants altered the pharmacokinetics of pitavastatin, rosuvastatin, simvastatin acid, atorvastatin and pravastatin, but our data revealed that there was no significant difference in therapeutic effect of pitavastatin among various genotypes. Interestingly, the alteration of pharmacokinetics did not extend to the response to pitavastatin. Similar results were also obtained for other statins in separate studies24, 25: the plasma concentration of pravastatin in subjects with haplotypes *15 or *17 (11187G>A, 388A>G, and 521T>C) was higher than in wild-type subjects when they were given 40 mg of pravastatin daily for 3 weeks, but there was no statistical difference in the lipid-lowering efficacy between genotypes24.
In vivo, part of pitavastatin is reversibly converted to a lactone form, and the disposition of pitavastatin lactone is different from that of the parent drug. Chung et al7 reported that SLCO1B1 521T>C and 388G>A were not associated with a change in the pharmacokinetics of pitavastatin lactone. In addition, the alteration of pharmacokinetics due to polymorphisms in SLCO1B1 may not be sufficient to affect the pharmacodynamics of pitavastatin. Takane et al26 reported that the SLCO1B1*15 allele was associated with a slow response to pravastatin therapy, and the combined genotype of CYP7A1 and APOE was a more useful index to predict the lipid-lowering effect of pravastatin. This implies that polymorphisms in other genes may play an important role in inter-individual variable response to statins.
In conclusion, the present study found that allele frequencies of SLCO1B1 388G>A and 521T>C in patients with essential hyperlipidemia were comparable to those in healthy Chinese population and there was no significant difference in the lipid-lowering efficacy of pitavastatin among various genotype groups.
Author contribution
Guo-ping YANG, Hong YUAN, Zhi-jun HUANG and Hong-hao ZHOU designed the research; Guo-ping YANG and Bin TANG performed the research; Dong-sheng OU-YANG, Lian-sheng WANG, Bin TANG and Wei ZHANG analyzed the data; and Gui-xiang ZHANG and Bin TANG wrote the paper.
References
König J, Cui Y, Nies AT, Keppler D . A novel human organic anion transporting polypeptide localized to the basolateral hepatocyte membrane. Am J Physiol Gastrointest Liver Physiol 2000; 278: G156–164.
van der Deure WM, Friesema EC, de Jong FJ, de Rijke YB, de Jong FH, Uitterlinden AG, et al. Organic anion transporter 1B1: an important factor in hepatic thyroid hormone and estrogen transport and metabolism. Endocrinology 2008; 149: 4695–701.
Fujino H, Yamada I, Shimada S, Yoneda M, Kojima J . Metabolic fate of pitavastatin, a new inhibitor of HMG-CoA reductase: human UDP-glucuronosyltransferase enzymes involved in lactonization. Xenobiotica 2003; 33: 27–41.
Yamada I, Fujino H, Shimada S, Kojima J . Metabolic fate of pitavastatin, a new inhibitor of HMG-CoA reductase: similarities and difference in the metabolism of pitavastatin in monkeys and humans. Xenobiotica 2003; 33: 789–803.
Hirano M, Maeda K, Shitara Y, Sugiyama Y . Contribution of OATP2 (OATP1B1) and OATP8 (OATP1B3) to the hepatic uptake of pitavastatin in humans. J Pharmacol Exp Ther 2004; 311: 139–46.
Ieiri I, Suwannakul S, Maeda K, Uchimaru H, Hashimoto K, Kimura M, et al. SLCO1B1 (OATP1B1, an uptake transporter) and ABCG2 (BCRP, an efflux transporter) variant alleles and pharmacokinetics of pitavastatin in healthy volunteers. Clin Pharmacol Ther 2007; 82: 541–7.
Chung JY, Cho JY, Yu KS, Kim JR, Oh DS, Jung HR, et al. Effect of OATP1B1 (SLCO1B1) variant alleles on the pharmacokinetics of pitavastatin in healthy volunteers. Clin Pharmacol Ther 2005; 78: 342–50.
Deng JW, Song IS, Shin HJ, Yeo CW, Cho DY, Shon JH, et al. The effect of SLCO1B1*15 on the disposition of pravastatin and pitavastatin is substrate dependent: the contribution of transporting activity changes by SLCO1B1*15. Pharmacogenet Genomics 2008; 18: 424–33.
Tachibana-Iimori R, Tabara Y, Kusuhara H, Kohara K, Kawamoto R, Nakura J, et al. Effect of genetic polymorphism of OATP-C (SLCO1B1) on lipid-lowering response to HMG-CoA reductase inhibitors. Drug Metab Pharmacokinet 2004; 19: 375–80.
Couvert P, Giral P, Dejager S, Gu J, Huby T, Chapman MJ, et al. Association between a frequent allele of the gene encoding OATP1B1 and enhanced LDL-lowering response to fluvastatin therapy. Pharmacogenomics 2008; 9: 1217–27.
Han JY, Lim HS, Shin ES, Yoo YK, Park YH, Lee JE, et al. Influence of the organic anion-transporting polypeptide 1B1 (OATP1B1) polymorphisms on irinotecan-pharmacokinetics and clinical outcome of patients with advanced non-small cell lung cancer. Lung Cancer 2008; 59: 69–75.
SEARCH Collaborative Group. SLCO1B1 variants and statin-induced myopathy — a genomewide study. N Engl J Med 2008; 359: 789–99.
Xu LY, He YJ, Zhang W, Deng S, Li Q, Zhang WX, et al. Organic anion transporting polypeptide-1B1 haplotypes in Chinese patients. Acta Pharmacol Sin 2007; 28: 1693–7.
Tirona RG, Leake BF, Merino G, Kim RB . Polymorphisms in OATP-C: identification of multiple allelic variants associated with altered transport activity among European- and African-Americans. J Biol Chem 2008; 276: 35669–75.
Kameyama Y, Yamashita K, Kobayashi K, Hosokawa M, Chiba K . Functional characterization of SLCO1B1 (OATP-C) variants, SLCO1B1*5, SLCO1B1*15 and SLCO1B1*15+C1007G, by using transient expression systems of HeLa and HEK293 cells. Pharmacogenet Genomics 2005; 15: 513–22.
Niemi M, Kivistö KT, Hofmann U, Schwab M, Eichelbaum M, Fromm MF . Fexofenadine pharmacokinetics are associated with a polymorphism of the SLCO1B1 gene (encoding OATP1B1). Br J Clin Pharmacol 2005; 59: 602–4.
Niemi M, Backman JT, Kajosaari LI, Leathart JB, Neuvonen M, Daly AK, et al. Polymorphic organic anion transporting polypeptide 1B1 is a major determinant of repaglinide pharmacokinetics. Clin Pharmacol Ther 2005; 77: 468–78.
Lee E, Ryan S, Birmingham B, Zalikowski J, March R, Ambrose H, et al. Rosuvastatin pharmacokinetics and pharmacogenetics in white and Asian subjects residing in the same environment. Clin Pharmacol Ther 2005; 78: 330–41.
Mwinyi J, Johne A, Bauer S, Roots I, Gerloff T . Evidence for inverse effects of OATP-C (SLC21A6) 5 and 1b haplotypes on pravastatin kinetics. Clin Pharmacol Ther 2004; 75: 415–21.
Nishizato Y, Ieiri I, Suzuki H, Kimura M, Kawabata K, Hirota T, et al. Polymorphisms of OATP-C (SLC21A6) and OAT3 (SLC22A8) genes: consequences for pravastatin pharmacokinetics. Clin Pharmacol Ther 2003; 73: 554–65.
Pasanen MK, Neuvonen M, Neuvonen PJ, Niemi M . SLCO1B1 polymorphism markedly affects the pharmacokinetics of simvastatin acid. Pharmacogenet Genomics 2006; 16: 873–9.
Choi JH, Lee MG, Cho JY, Lee JE, Kim KH, Park K . Influence of OATP1B1 genotype on the pharmacokinetics of rosuvastatin in Koreans. Clin Pharmacol Ther 2008; 83: 251–7.
Pasanen MK, Fredrikson H, Neuvonen PJ, Niemi M . Different effects of SLCO1B1 polymorphism on the pharmacokinetics of atorvastatin and rosuvastatin. Clin Pharmacol Ther 2007; 82: 726–33.
Igel M, Arnold KA, Niemi M, Hofmann U, Schwab M, Lütjohann D, et al. Impact of the SLCO1B1 polymorphism on the pharmacokinetics and lipid-lowering efficacy of multiple-dose pravastatin. Clin Pharmacol Ther 2006; 79: 419–26.
Thompson JF, Man M, Johnson KJ, Wood LS, Lira ME, Lloyd DB, et al. An association study of 43 SNPs in 16 candidate genes with atorvastatin response. Pharmacogenomics J 2005; 5: 352–8.
Takane H, Miyata M, Burioka N, Shigemasa C, Shimizu E, Otsubo K, et al. Pharmacogenetic determinants of variability in lipid-lowering response to pravastatin therapy. J Hum Genet 2006; 51: 822–6.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yang, Gp., Yuan, H., Tang, B. et al. Lack of effect of genetic polymorphisms of SLCO1B1 on the lipid-lowering response to pitavastatin in Chinese patients. Acta Pharmacol Sin 31, 382–386 (2010). https://doi.org/10.1038/aps.2009.203
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/aps.2009.203
Keywords
This article is cited by
-
Physiologically based pharmacokinetic (PBPK) modeling of pitavastatin in relation to SLCO1B1 genetic polymorphism
Archives of Pharmacal Research (2024)
-
Frequency of functional exonic single-nucleotide polymorphisms and haplotype distribution in the SLCO1B1 gene across genetic ancestry groups in the Qatari population
Scientific Reports (2022)
