
Abstract
Aim
This study was aimed at retrospectively investigating some common clinical factors, including the serum level of magnesium (Mg), associated with progression and remission/regression of diabetic kidney disease (DKD).
Methods
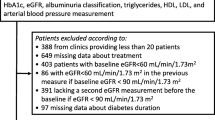
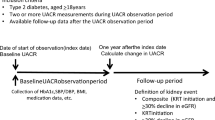
The subjects were 690 Japanese patients with type 2 diabetes mellitus who were receiving treatment with oral antidiabetic drugs other than SGLT2 inhibitors. Routine clinical data were collected on the first and last day of the observation period. The prognosis of DKD is categorized into four stages according to the Kidney Disease Improving Global Outcomes classification. Progression was defined as transition from any of the lower three risk categories (LR, MIR, HR) at the start of the observation period, to the VHR stage/category at the end of the observation period. Remission/regression was defined as improvement of the risk category by at least one stage from the start to the end of the observation period. Factors associated with progression and regression/remission were investigated using Cox proportional hazards analysis. Furthermore, the factors associated with the annual decrease in eGFR of 5 ml/min/1.73 m2 or more were examined by logistic regression analysis. Factors associated with transition of urinary protein negative to trace or positive, or transition of negative or trace to positive, were investigated by Cox proportional hazard analysis.
Results
The observation period was 2251 ± 1614 days. Age (Exp [B] = 1.10, 95% CI; 1.06–1.14; P < 0.01; 1 year old), serum Mg (Exp [B] = 0.82, 95% CI; 0.71–0.95; P < 0.01); 0.1 mg/dl), and serum HbA1c (Exp [B] = 1.03, 95% CI; 1.01–1.05; P < 0.01: 0.1%) were associated with progression of DKD; on the other hand, serum ALT was associated with the likelihood of remission/regression of DKD (Exp [B] = 1.01, 95% CI; 1.002–1.018; P < 0.05; 1 IU/L). The decline in eGFR was associated with higher HbA1c levels, hypomagnesemia, and lower ALT. The new appearance of trace or overt proteinuria was correlated with higher HbA1c levels, advancing age, hypomagnesemia and hypertriglycemia.
Conclusion
Our findings confirmed previous reports that advancing age and serum HbA1c levels were associated with an increased risk of progression of DKD. Lower serum Mg concentrations were also found to be associated with a high risk of progression of DKD, and interventional studies are needed to confirm a causal relationship. Elevated HbA1c levels and hypomagnesemia were common factors in the decline in eGFR and the appearance of trace or overt proteinuria. Lower serum ALT levels were associated with the decline in eGFR. Since serum ALT is known to decrease as the renal function deteriorates, serum ALT is considered to be a marker of renal function.
Similar content being viewed by others

References
Goto A, Noda M, Inoue M, Goto M, Charvat H. Increasing number of people with diabetes in Japan: is this trend real? Intern Med. 2016;55:1827–30.
Sagoo MK, Gnudi L. Diabetic nephropathy: an overview. Methods Mol Biol. 2020;2067:3–7.
Alicic RZ, Rooney MT, Tuttle KR. Diabetic kidney disease: challenges, progress, and possibilities. Clin J Am Soc Nephrol. 2017;12:2032–45.
Berhane AM, Weil EJ, Knowler WC, Nelson RG, Hanson RL. Albuminuria and estimated glomerular filtration rate as predictors of diabetic end-stage renal disease and death. Clin J Am Soc Nephrol. 2011;6:2444–51.
Ohkuma T, Jun M, Chalmers J, Cooper ME, Hamet P, Harrap S, et al. Combination of changes in estimated GFR and albuminuria and the risk of major clinical outcomes. Clin J Am Soc Nephrol. 2019;14:862–72.
Kidney Disease Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease Chapter 1: Definition and classification of CKD. Kidney Int. 2013;3:5–62.
Radcliffe NJ, Seah JM, Clarke M, MacIsaac RJ, Jerums G, Ekinci EI. Clinical predictive factors in diabetic kidney disease progression. J Diabetes Investig. 2017;8:6–18.
Oliveira B, Cunningham J, Walsh SB. Magnesium balance in chronic and end-stage kidney disease. Adv Chronic Kidney Dis. 2018;25:291–5.
Tin A, Grams ME, Maruthur NM, Astor BC, Couper D, Mosley TH, et al. Results from the atherosclerosis risk in communities study suggest that low serum magnesium is associated with incident kidney disease. Kidney Int. 2015;87:820–7.
Pham PC, Pham PM, Pham PA, Pham SV, Pham HV, Miller JM, et al. Lower serum magnesium levels are associated with more rapid decline of renal function in patients with diabetes mellitus type 2. Clin Nephrol. 2005;63:429–36.
Sakaguchi Y, Shoji T, Hayashi T, Suzuki A, Shimizu M, Mitsumoto K, et al. Hypomagnesemia in type 2 diabetic nephropathy: a novel predictor of end-stage renal disease. Diabetes Care. 2012;35:1591–7.
Hovind P, Tarnow L, Parving HH. Remission and regression of diabetic nephropathy. Curr Hypertens Rep. 2004;6:377–82.
Gaede P, Tarnow L, Vedel P, Parving HH, Pedersen O. Remission to normoalbuminuria during multifactorial treatment preserves kidney function in patients with type 2 diabetes and microalbuminuria. Nephrol Dial Transplant. 2004;19:2784–8.
Jiang G, Luk AOY, Tam CHT, Xie F, Carstensen B, Lau ESH, et al. Progression of diabetic kidney disease and trajectory of kidney function decline in Chinese patients with Type 2 diabetes. Kidney Int. 2019;95:178–87.
Neuen BL, Young T, Heerspink HJL, Neal B, Perkovic V, Billot L, et al. SGLT2 inhibitors for the prevention of kidney failure in patients with type 2 diabetes: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2019;7:845–54.
American Diabetes Association 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2020. Diabetes Care. 2020;43(1):S14–31.
Miyazaki H, Babazono A, Nishi T, Maeda T, Imatoh T, Ichiba M, et al. Does antihypertensive treatment with renin-angiotensin system inhibitors prevent the development of diabetic kidney disease? BMC Pharmacol Toxicol. 2015;16:22.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al. Collaborators developing the Japanese equation for estimated GFR. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
Krolewski AS, Skupien J, Rossing P, Warram JH. Fast renal decline to end-stage renal disease: an unrecognized feature of nephropathy in diabetes. Kidney Int. 2017;91:1300–11.
Rosenstock J, Perkovic V, Johansen OE, Cooper ME, Kahn SE, Marx N, et al. Effect of linagliptin vs. placebo on major cardiovascular events in adults with type 2 diabetes and high cardiovascular and renal risk: the CARMELINA randomized clinical trial. JAMA. 2019;321:69–79.
Denic A, Glassock RJ, Rule AD. Structural and functional changes with the aging kidney. Adv Chronic Kidney Dis. 2016;23:19–28.
Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321:405–12.
Ferrè S, Li X, Adams-Huet B, Maalouf NM, Sakhaee K, Toto RD, et al. Low serum magnesium is associated with faster decline in kidney function: the Dallas Heart Study experience. J Investig Med. 2019;67:987–94.
Del Gobbo LC, Imamura F, Wu JH, de Oliveira Otto MC, Chiuve SE, Mozaffarian D. Circulating and dietary magnesium and risk of cardiovascular disease: a systematic review and meta-analysis of prospective studies. Am J Clin Nutr. 2013;98:160–73.
Rebholz CM, Tin A, Liu Y, Kuczmarski MF, Evans MK, Zonderman AB, Crews DC. Dietary magnesium and kidney function decline: the healthy aging in neighborhoods of diversity across the life span study. Am J Nephrol. 2016;44:381–7.
Gröber U, Schmidt J, Kisters K. Magnesium in prevention and therapy. Nutrients. 2015;7:8199–226.
Hata A, Doi Y, Ninomiya T, Mukai N, Hirakawa Y, Hata J, et al. Magnesium intake decreases Type 2 diabetes risk through the improvement of insulin resistance and inflammation: the Hisayama Study. Diabet Med. 2013;30:1487–94.
Qu X. Magnesium and the risk of cardiovascular events: a meta-analysis of prospective cohort studies. PLoS ONE. 2013;8:e57720.
Dong JF, Cruz MA, Aboulfatova K, Martin C, Choi H, Bergeron AL, et al. Magnesium maintains endothelial integrity, upregulates proteolysis of ultra-large von Willebrand factor, and reduces platelet aggregation under flow conditions. Thromb Haemost. 2008;99:586–93.
Vervloet M. Modifying phosphate toxicity in chronic kidney disease. Toxins (Basel). 2019;11:522.
Sakaguchi Y, Hamano T, Obi Y, Monden C, Oka T, Yamaguchi S, et al. A randomized trial of magnesium oxide and oral carbon adsorbent for coronary artery calcification in predialysis CKD. J Am Soc Nephrol. 2019;30:1073–85.
Miyake T, Kumagi T, Hirooka M, Koizumi M, Furukawa S, Ueda T, et al. Metabolic markers and ALT cutoff level for diagnosing nonalcoholic fatty liver disease: a community-based cross-sectional study. J Gastroenterol. 2012;47:696–703.
Jia G, Di F, Wang Q, Shao J, Gao L, Wang L, et al. Non-alcoholic fatty liver disease is a risk factor for the development of diabetic nephropathy in patients with type 2 diabetes mellitus. PLoS ONE. 2015;10:e0142808.
Orlić L, Mikolasevic I, Bagic Z, Racki S, Stimac D, Milic S. Chronic kidney disease and nonalcoholic Fatty liver disease-is there a link? Gastroenterol Res Pract. 2014;4:847539.
Adiga US, Malawadi BN. Association of diabetic nephropathy and liver disorders. J Clin Diagn Res. 2016;10:BC05–7.
Ray L, Nanda SK, Chatterjee A, Sarangi R, Ganguly S. A comparative study of serum aminotransferases in chronic kidney disease with and without end-stage renal disease: Need for new reference ranges. Int J Appl Basic Med Res. 2015;5:31–5.
Candinas D, Keusch G, Schlumpf R, Burger HR, Gmür J, Largiadèr F. Hemolytic-uremic syndrome following kidney transplantation: prognostic factors. Schweiz Med Wochenschr. 1994;124:1789–99.
Ruhl CE, Everhart JE. The association of low serum alanine aminotransferase activity with mortality in the US population. Am J Epidemiol. 2013;178:1702–11.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
TY designed the study, analyzed, and interpreted the data, performed the literature search, and wrote the first draft of the manuscript. KK collected and. Interpreted the data. KA analyzed and interpreted the data.
Corresponding author
Ethics declarations
Conflict of interest
Not applicable.
Author agreement
All authors have read and approved the final version of the manuscript being submitted. They certify that the contents of the article represent the authors’ original work, and that the article had neither been published previously, nor is under consideration for publication in any other journal.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
About this article

Cite this article
Yanagawa, T., Koyano, K. & Azuma, K. Retrospective study of factors associated with progression and remission/regression of diabetic kidney disease-hypomagnesemia was associated with progression and elevated serum alanine aminotransferase levels were associated with remission or regression-. Diabetol Int 12, 268–276 (2021). https://doi.org/10.1007/s13340-020-00483-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13340-020-00483-1