
Abstract
Background
The 2011 St. Gallen Consensus Statement advocated using histological grade (HG) as a proliferation marker of breast cancer (BC) if reliable Ki67 labeling index (Ki67-LI) assessment is not available. However, it has been difficult to evaluate tumor aggressiveness in case of HG2.
Methods
A total of 259 cases of BC were assessed for HG, Ki67-LI and other clinicopathological features. The cut point for Ki67-LI was interpreted as low and high using a 14 % threshold.
Results
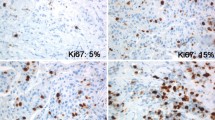
The average age at diagnosis was 58.2 years (range 28–86); 64.9 % of the patients were postmenopausal. Of the 259 cases, 151 were stage I, 78 were stage II, 29 were stage III, and 1 was stage IV. The subtypes based on immunohistochemical staining were 60 cases of luminal A (LA) type (23.2 %), 37 cases of luminal B (LB) (HER2−) type (14.3 %), 91 cases of LB (HER2+) type (35.1 %), 40 cases of human epidermal growth factor receptor 2 (HER2) type (15.4 %) and 31 cases of triple negative (TN) type (12 %). HG was 1 (89 cases, 34.4 %), 2 (117 cases, 45.2 %) and 3 (53 cases, 20.5 %). High Ki67-LI cases were observed in HG1 (37.1 %), HG2 (56.4 %) and HG3 (96.2 %). Especially in cases of HG2, high Ki67-LI cases were observed in 0 % of LA type, 100 % of LB (HER2−) type, 71.2 % of LB (HER2+) type, 68.8 % of HER2 type and 40.0 % of TN type. The average Ki67-LI was 6.0 ± 3.8 (LA type), 31.4 ± 15.7 [LB (HER2−) type], 20.2 ± 14.8 [LB (HER2+) type], 32.7 ± 21.9 (HER2 type) and 55.7 ± 32.2 (TN type). All LA-type cases and 66.7 % of LB (HER2+)-type cases were low Ki67-LI.
Conclusions
Our study demonstrates that all LA-type cases and most HG1 of LB (HER2+)-type cases are low proliferative. However, HG was not informative enough for estimating tumor proliferation in cases of LB (HER2−), HER2 and TN types. It is necessary to add other proliferation tools such as the gene expression profiling tool and Ki67-LI except in LA and HG1 of LB (HER2+)-type cases.
Similar content being viewed by others


References
Gerdes J, Lemke H, Baisch H, Wacker HH, Schwab U, Stein H. Cell cycle analysis of a cell proliferation-associated human nuclear antigen defined by the monoclonal antibody Ki-67. J Immunol. 1984;133:1710–5.
de Azambuja E, Cardoso F, de Castro G, Colozza M Jr, Mano MS, Durbecq V, et al. Ki-67 as prognostic marker in early breast cancer: a meta-analysis of published studies involving 12,155 patients. Br J Cancer. 2007;96:1504–13.
Goldhirsch A, Wood WC, Coates AS, Gelber RD, Thürlimann B, Panel members. Strategies for subtypes—dealing with the diversity of breast cancer: highlights of the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann Oncol. 2011;22:1736–47.
Cheang MC, Chia SK, Voduc D, Gao D, Leung S, Snider J, et al. Ki67 index, HER2 status, and prognosis of patients with luminal B breast cancer. J Natl Cancer Inst. 2009;101:736–50.
Elston CW, Ellis IO. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: experience from a large study with long-term follow-up. Histopathology. 1991;19:403–10.
Perou CM, Sørlie T, Eisen MB, van de Rijn M, Jeffrey SS, Rees CA, et al. Molecular portraits of human breast tumours. Nature. 2000;406:747–52.
Aleskandarany MA, Rakha EA, Macmillan RD, Powe DG, Ellis IO, Green AR. MIB1/Ki-67 labeling index can classify grade 2 breast cancer into two clinically distinct subgroups. Breast Cancer Res Treat. 2011;127:591–9.
Klintman M, Bendahl PO, Grabau D, Lövgren K, Malmström P, South Sweden Breast Cancer Group. The prognostic value of Ki67 is dependent on estrogen receptor status and histological grade in premenopausal patients with node-negative breast cancer. Mod Pathol. 2010;23:251–9.
Rosa FE, Caldeira JR, Felipes J, Bertonha FB, Quevedo FC, Domingues MA, et al. Evaluation of estrogen receptor alpha and beta and progesterone receptor expression and correlation with clinicopathologic factors and proliferative marker Ki-67 in breast cancers. Hum Pathol. 2008;39:720–30.
Jarzabek K, Koda M, Kozlowski L, Mittre H, Sulkowski S, Kottler ML, et al. Distinct mRNA, protein expression patterns and distribution of oestrogen receptors alpha and beta in human primary breast cancer: correlation with proliferation marker Ki-67 and clinicopathological factors. Eur J Cancer. 2005;41:2924–34.
Dai J, Jian J, Bosland M, Frenkel K, Bernhardt G, Huang X. Roles of hormone replacement therapy and iron in proliferation of breast epithelial cells with different estrogen and progesterone receptor status. Breast. 2008;17:172–9.
Press MF, Bernstein L, Thomas PA, Meisner LF, Zhou JY, Ma Y, et al. HER-2/neu gene amplification characterized by fluorescence in situ hybridization: poor prognosis in node-negative breast carcinomas. J Clin Oncol. 1997;15:2894–904.
Fasching PA, Heusinger K, Haberle L, Niklos M, Hein A, Bayer CM, et al. Ki67, chemotherapy response, and prognosis in breast cancer patients receiving neoadjuvant treatment. BMC Cancer. 2011;11:486.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Hayashi, S., Kitada, M., Sato, K. et al. Histological grade as an alternative to the Ki67 labeling index is only available for luminal-type breast cancers. Breast Cancer 21, 47–51 (2014). https://doi.org/10.1007/s12282-012-0353-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12282-012-0353-2