
Abstract
Background
Studies comparing primary medical treatment of acromegaly with surgery are often non-randomized, and not stratified by illness severity. We prospectively compared primary medical therapy with pituitary surgery in patients with acromegaly. All patients had macroadenomas, at least one random human growth hormone (GH) level ≥12.5 ng/mL, elevated IGF-I levels and failure to suppress GH to <1 ng/mL during an oral glucose tolerance test (oGTT).
Methods
Forty-one patients from seven centers were randomized to primary treatment with octreotide LAR, 30 mg every 4 weeks × 3 months (ARM A, N = 15), or pituitary surgery (ARM B, N = 26) using a 1:2 randomization design. Patients cured by surgery (defined as nadir GH during oGTT <1 ng/mL and normal IGF-I) received no subsequent treatment. Those not cured surgically were then treated with octreotide LAR (SubArm B1) for 3 months.
Results
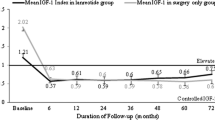
Only one of the 15 patients in ARM A (6.7%) had normalization of both GH and IGF-I. In contrast, 13/26 patients had normalization of both GH and IGF-I after surgery alone (50%). Of the remaining 13 patients who did not normalize with surgery alone, treatment with octreotide LAR resulted in a normal nadir GH and normal serum IGF-I in 7 (53.9%). In total, 20/26 in ARM B (76.9%) experienced normalization of defined biochemical acromegaly parameters.
Conclusions
Pituitary surgery alone was more effective than primary medical treatment (p = 0.006), and the combination of surgery followed by medical therapy was even more effective (p < 0.0001). Subjects treated with medical therapy after surgical debulking had a significant improvement in response rate compared to matched subjects treated with primary medical therapy.


Similar content being viewed by others


References
Melmed S (2006) Medical progress: acromegaly. NEW Engl J Med 355:2558–2573
Caron PJ, Bevan JS, Petersenn S et al (2014) Tumor shrinkage with lanreotide Autogel 120 mg as primary therapy in acromegaly: results of a prospective multicenter clinical trial. J Clin Endocrinol Metab 99:1282–1290
Howlett TA, Willis D, Walker G, Wass JA, Trainer PJ, Group UKARS (2013) Control of growth hormone and IGF1 in patients with acromegaly in the UK: responses to medical treatment with somatostatin analogues and dopamine agonists. Clin Endocrinol 79:689–699
Bevan JS, Atkin SL, Atkinson AB et al (2002) Primary medical therapy for acromegaly: an open, prospective, multicenter study of the effects of subcutaneous and intramuscular slow-release octreotide on growth hormone, insulin-like growth factor-I, and tumor size. J Clin Endocrinol Metab 87:4554–4563
Karaca Z, Tanriverdi F, Elbuken G et al (2011) Comparison of primary octreotide-lar and surgical treatment in newly diagnosed patients with acromegaly. Clin Endocrinol 75:678–684
Giustina A, Barkan A, Casanueva FF et al (2000) Criteria for cure of acromegaly: a consensus statement. J Clin Endocrinol Metab 85:526–529
Capatina C, Wass JA (2015) 60 Years of neuroendocrinology: acromegaly. J Endocrinol 226:T141-T160
Freda PU (2003) Current concepts in the biochemical assessment of the patient with acromegaly. Growth Horm IGF Res 13:171–184
Holdaway IM, Rajasoorya RC, Gamble GD (2004) Factors influencing mortality in acromegaly. J Clin Endocrinol Metab 89:667–674
Jane JA Jr, Starke RM, Elzoghby MA et al (2011) Endoscopic transsphenoidal surgery for acromegaly: remission using modern criteria, complications, and predictors of outcome. J Clin Endocrinol Metab 96:2732–2740
Gittoes NJ, Sheppard MC, Johnson AP, Stewart PM (1999) Outcome of surgery for acromegaly–the experience of a dedicated pituitary surgeon. QJM 92:741–745
Wass JA, Turner HE, Adams CB (1999) The importance of locating a good pituitary surgeon. Pituitary 2:51–54
Ahmed S, Elsheikh M, Stratton IM, Page RC, Adams CB, Wass JA (1999) Outcome of transphenoidal surgery for acromegaly and its relationship to surgical experience. Clin Endocrinol 50:561–567
Lissett CA, Peacey SR, Laing I, Tetlow L, Davis JR, Shalet SM (1998) The outcome of surgery for acromegaly: the need for a specialist pituitary surgeon for all types of growth hormone (GH) secreting adenoma. Clin Endocrinol 49:653–657
Hazer DB, Isik S, Berker D et al (2013) Treatment of acromegaly by endoscopic transsphenoidal surgery: surgical experience in 214 cases and cure rates according to current consensus criteria. J Neurosurg 119:1467–1477
Starke RM, Raper DM, Payne SC, Vance ML, Oldfield EH, Jane JA Jr (2013) Endoscopic vs microsurgical transsphenoidal surgery for acromegaly: outcomes in a concurrent series of patients using modern criteria for remission. J Clin Endocrinol Metab 98:3190–3198
Cappabianca P, de Divitiis E (2003) Image guided endoscopic transnasal removal of recurrent pituitary adenomas. Neurosurgery 52:483–484
Newman CB, Melmed S, George A et al (1998) Octreotide as primary therapy for acromegaly. J Clin Endocrinol Metab 83:3034–3040
Kreutzer J, Vance ML, Lopes MB, Laws ER Jr (2001) Surgical management of GH-secreting pituitary adenomas: an outcome study using modern remission criteria. J Clin Endocrinol Metab 86:4072–4077
Rajasoorya C, Holdaway IM, Wrightson P, Scott DJ, Ibbertson HK (1994) Determinants of clinical outcome and survival in acromegaly. Clin Endocrinol 41:95–102
Shimon I, Cohen ZR, Ram Z, Hadani M (2001) Transsphenoidal surgery for acromegaly: endocrinological follow-up of 98 patients. Neurosurgery 48:1239–1243
Jallad RS, Musolino NR, Kodaira S, Cescato VA, Bronstein MD (2007) Does partial surgical tumour removal influence the response to octreotide-LAR in acromegalic patients previously resistant to the somatostatin analogue? Clin Endocrinol 67:310–315
Petrossians P, Borges-Martins L, Espinoza C et al (2005) Gross total resection or debulking of pituitary adenomas improves hormonal control of acromegaly by somatostatin analogs. Eur J Endocrinol 152:61–66
Colao A, Attanasio R, Pivonello R et al (2006) Partial surgical removal of growth hormone-secreting pituitary tumors enhances the response to somatostatin analogs in acromegaly. J Clin Endocrinol Metab 91:85–92
Karavitaki N, Turner HE, Adams CB et al (2008) Surgical debulking of pituitary macroadenomas causing acromegaly improves control by lanreotide. Clin Endocrinol 68:970–975
Wass J (2005) Debulking of pituitary adenomas improves hormonal control of acromegaly by somatostatin analogues. Eur J Endocrinol 152:693–694
Reubi JC, Landolt AM (1989) The growth hormone responses to octreotide in acromegaly correlate with adenoma somatostatin receptor status. J Clin Endocrinol Metab 68:844–850
Herman-Bonert VS, Zib K, Scarlett JA, Melmed S (2000) Growth hormone receptor antagonist therapy in acromegalic patients resistant to somatostatin analogs. J Clin Endocrinol Metab 85:2958–2961
Trainer PJ, Drake WM, Katznelson L et al (2000) Treatment of acromegaly with the growth hormone-receptor antagonist pegvisomant. New Engl J Med 342:1171–1177
van der Lely AJ, Hutson RK, Trainer PJ et al (2001) Long-term treatment of acromegaly with pegvisomant, a growth hormone receptor antagonist. The Lancet 358:1754–1759
Trainer PJ, Ezzat S, D’Souza GA, Layton G, Strasburger CJ (2009) A randomized, controlled, multicentre trial comparing pegvisomant alone with combination therapy of pegvisomant and long-acting octreotide in patients with acromegaly. Clin Endocrinol 71:549 –557
Acknowledgements
The authors wish to acknowledge the invaluable contribution of Ms. Heather Levitt, who was instrumental in organizing the multicenter effort as well as the original development of the study materials. This study was supported by Novartis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors disclose the following potential conflict of interest issues: AB is a recipient of an Investigator Initiated Grant from Novartis and received consulting fees and honoraria from Novartis, Ipsen and Pfizer; BS owns stock from Novartis and Pfizer; AMC is a consultant and recipient of unrestricted research grants from Novartis and Ipsen; RP received consulting fees from Novartis, and honoraria and research funding from Ipsen and Pfizer; BB received research funding from Novartis and served as a consultant for Ipsen, Novartis and Pfizer; AK received grant support from Pfizer, is a consultant for Chiasma and is on a Scientific Advisory Board for Crinetics. The rest of the authors reported no potential conflict of interest.
Additional information
This article is dedicated to the memory of Dr. David Kleinberg.
Rights and permissions
About this article

Cite this article
Fahlbusch, R., Kleinberg, D., Biller, B. et al. Surgical debulking of pituitary adenomas improves responsiveness to octreotide lar in the treatment of acromegaly. Pituitary 20, 668–675 (2017). https://doi.org/10.1007/s11102-017-0832-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11102-017-0832-8