
Abstract
Aim
The purpose of this is to evaluate the safety and feasibility of recrossing the interatrial septum in case of inadvertent loss of or need for repeated left atrial access using a simple electroanatomical landmark without the use of fluoroscopy.
Methods
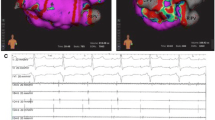
Twenty-five consecutive patients undergoing pulmonary vein isolation (PVI) for paroxysmal (n = 12) or persistent (n = 13) atrial fibrillation ablation were included. All procedures were performed using an electroanatomical mapping system (Carto 3, Biosense Webster, Diamond Bar, USA). After fluoroscopy-guided double transseptal puncture and fast anatomical mapping of the left atrium, a reconstruction of the transseptal access was created by retracting the mapping catheter into the sheath to the level of the inferior vena cava. After completing the left sided ablation, both sheaths and catheters were withdrawn to the inferior vena cava. Recrossing was then attempted by fellows (EF) and experienced operators (EO) using the reconstruction of the transseptal access in a standard right anterior oblique (RAO) and left anterior oblique (LAO) projection without the use of fluoroscopy.
Results
Using the described technique, EP fellows and experienced operators could recross the interatrial septum without fluoroscopy in all patients. Median time needed for recrossing was 14 s (interquartile range (IQR) 7–20). Median recrossing times did not differ significantly between EF and EO (14 (IQR 8–26.5 s) versus 12 (IQR 6.5–17.5 s), p = 0.26). In five (20 %) procedures, recrossing was necessary during the procedure after intermittent mapping of the right atrium or inadvertent catheter dislodgment.
Conclusion
Adding a simple and fast anatomical reconstruction of the transseptal access to the standard left atrial mapping procedure allows for easy and fluoroscopy-free recrossing of the interatrial septum during atrial fibrillation ablation and further reduces radiation exposure.

Similar content being viewed by others


Abbreviations
- AF:
-
Atrial fibrillation
- BMI:
-
Body mass index
- EF:
-
Electrophysiology fellow
- EO:
-
Experienced operator
- IQR:
-
Interquartile range
- LA:
-
Left atrium
- PVI:
-
Pulmonary vein isolation
- PFO:
-
Patent foramen ovale
- TSP:
-
Transseptal puncture
References
Cappato, R., Calkins, H., Chen, S.-A., Davies, W., Iesaka, Y., Kalman, J., et al. (2010). Updated worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circulation. Arrhythmia and Electrophysiology, 3(1), 32–38.
Calkins, H., Kuck, K. H., Cappato, R., Brugada, J., Camm, A. J., Chen, S.-A., et al. (2012). 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design: a report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. Developed in partnership with the European Heart Rhythm Association (EHRA), a registered branch of the European Society of Cardiology (ESC) and the European Cardiac Arrhythmia Society (ECAS); and in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), the Asia Pacific Heart Rhythm Society (APHRS), and the Society of Thoracic Surgeons (STS). Endorsed by the governing bodies of the American College of Cardiology Foundation, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, the Asia Pacific Heart Rhythm Society, and the Heart Rhythm Society. Journal of Interventional Cardiac Electrophysiology, 33, 171–257.
De Ponti, R., Cappato, R., Curnis, A., Della Bella, P., Padeletti, L., Raviele, A., et al. (2006). Transseptal catheterization in the electrophysiology laboratory: data from a multicenter survey spanning 12 years. Journal of the American College of Cardiology, 47(5), 1037–1042.
Tucker, K. J., Curtis, A. B., Murphy, J., Conti, J. B., Kazakis, D. J., Geiser, E. A., et al. (1996). Transesophageal echocardiographic guidance of transseptal left heart catheterization during radiofrequency ablation of left-sided accessory pathways in humans. Pacing and Clinical Electrophysiology: PACE, 19(3), 272–281.
Daoud, E. G., Kalbfleisch, S. J., & Hummel, J. D. (1999). Intracardiac echocardiography to guide transseptal left heart catheterization for radiofrequency catheter ablation. Journal of Cardiovascular Electrophysiology, 10(3), 358–363.
Hunter, R. J., Diab, I., Tayebjee, M., Richmond, L., Sporton, S., Earley, M. J., et al. (2011). Characterization of fractionated atrial electrograms critical for maintenance of atrial fibrillation a randomized, controlled trial of ablation strategies (the CFAE AF trial). Circulation. Arrhythmia and Electrophysiology, 4(5), 622–629.
O’Neill, M. D., Wright, M., Knecht, S., Jaïs, P., Hocini, M., Takahashi, Y., et al. (2009). Long-term follow-up of persistent atrial fibrillation ablation using termination as a procedural endpoint. European Heart Journal, 30(9), 1105–1112.
Camm, A. J., Lip, G. Y. H., De Caterina, R., Savelieva, I., Atar, D., Hohnloser, S. H., et al. (2012). 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. European Heart Journal, 33(21), 2719–2747.
Natarajan, M. K., Paul, N., Mercuri, M., Waller, E. J., Leipsic, J., Traboulsi, M., et al. (2013). Canadian Cardiovascular Society position statement on radiation exposure from cardiac imaging and interventional procedures. Canadian Journal of Cardiology, 29(11), 1361–1368.
Picano, E., Vañó, E., Rehani, M. M., Cuocolo, A., Mont, L., Bodi, V., et al. (2014). The appropriate and justified use of medical radiation in cardiovascular imaging: a position document of the ESC Associations of Cardiovascular Imaging, Percutaneous Cardiovascular Interventions and Electrophysiology. European Heart Journal, eht394.
Yamada, T., McElderry, H. T., Epstein, A. E., Plumb, V. J., & Kay, G. N. (2007). One-puncture, double-transseptal catheterization manoeuvre in the catheter ablation of atrial fibrillation. Europace, 9(7), 487–489.
Sporton, S. C., Earley, M. J., Nathan, A. W., & Schilling, R. J. (2004). Electroanatomic versus fluoroscopic mapping for catheter ablation procedures: a prospective randomized study. Journal of Cardiovascular Electrophysiology, 15(3), 310–315.
Rotter, M., Takahashi, Y., Sanders, P., Haïssaguerre, M., Jaïs, P., Hsu, L.-F., et al. (2005). Reduction of fluoroscopy exposure and procedure duration during ablation of atrial fibrillation using a novel anatomical navigation system. European Heart Journal, 26(14), 1415–1421.
Nguyen, B., Merino, J., Shachar, Y., Estrada, A., Doiny, D., Castrejon, S., et al. (2013). Non-fluoroscopic transseptal catheterization during electrophysiology procedures using a remote magnetic navigation system. JAFIB: Journal of Atrial Fibrillation, 6(4), 6–9.
Lehrmann, H., Schneider, J., Jadidi, A. S., Park, C.-I., Schiebeling-Römer, J., Allgeier, J., et al. (2014). Transseptal access for left atrial ablation: the catheter-probing techniques are not without risk. Journal of Cardiovascular Electrophysiology, 25, 479–484.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Pavlović, N., Reichlin, T., Kühne, M. et al. Fluoroscopy-free recrossing of the interatrial septum during left atrial ablation procedures. J Interv Card Electrophysiol 41, 261–266 (2014). https://doi.org/10.1007/s10840-014-9952-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-014-9952-5