
Abstract
Objective
To report a unique retinal signaling defect in GNB5-related disease.
Methods
A 3-year-old female child underwent detailed systemic and ophthalmological evaluation. The eye examination included fundus photography, spectral domain optical coherence tomography and an extended protocol full-field electroretinography (ERG) including the ISCEV recommended standard steps. The dark-adapted (DA) ERGs were performed to a series of white flashes (range 0.006–30.0 cd s m−2) and two red flashes. The DA ERGs to higher stimulus intensities (3.0, 10.0 and 30.0 cd s m−2) were tested using a range of inter-stimulus intervals (ISI) of up to 60 s. In addition to standard light-adapted (LA) ERGs, a short-duration (0.5 s) LA 3.0 30-Hz flicker ERG and a long-duration LA ON–OFF ERG were also performed. Genetic testing included microarray, mitochondrial genome testing and whole exome sequencing.
Results
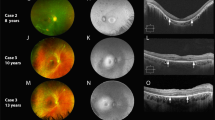
The child was diagnosed to have status epilepticus and bradycardia at 6 months of age. Subsequently, she was diagnosed to have global developmental delay and hypotonia. On ophthalmological evaluation, the child fixes and follows light. Fundus evaluation showed mild optic disk pallor; macular SD-OCT was normal. The dim flash DA ERGs (DA 0.006 and DA 0.01 cd s m−2) were non-detectable. DA red flash ERGs showed the presence of an x-wave (cone component) and no rod component. The DA 3.0, 10.0 and 30.0 ERGs showed electronegative configuration regardless of the ISI; the averaged a-wave amplitude (4 flashes) was smaller at shorter ISI but became normal at a prolonged ISI (60 s). The LA 30-Hz flicker ERG was severely reduced but detectable for the initial 0.5 s; this became non-detectable after 5 s of averaging. The LA 3.0 2-Hz ERG showed markedly reduced a- and b-wave amplitudes and a reduced b:a ratio; the LA ON–OFF ERGs were non-detectable. WES identified a homozygous null mutation in G protein subunit beta 5 (GNB5; c.1032C>A/p.Tyr344*).
Conclusion
This report identifies for the first time a unique retinopathy associated with biallelic mutations in GNB5. The observed phenotype is consistent with a dual retinal signaling defect reminiscent of features of bradyopsia and rod ON-bipolar dysfunction.


Similar content being viewed by others


References
Lodder EM et al (2016) GNB5 mutations cause an autosomal-recessive multisystem syndrome with sinus bradycardia and cognitive disability. Am J Hum Genet 99(3):704–710
McCulloch DL et al (2015) ISCEV standard for full-field clinical electroretinography (2015 update). Doc Ophthalmol 130(1):1–12
Krispel CM et al (2003) Prolonged photoresponses and defective adaptation in rods of Gbeta5−/− mice. J Neurosci 23(18):6965–6971
Rao A et al (2007) Gbeta5 is required for normal light responses and morphology of retinal ON-bipolar cells. J Neurosci 27(51):14199–14204
Nishiguchi KM et al (2004) Defects in RGS9 or its anchor protein R9AP in patients with slow photoreceptor deactivation. Nature 427(6969):75–78
Michaelides M et al (2010) Novel mutations and electrophysiologic findings in RGS9- and R9AP-associated retinal dysfunction (Bradyopsia). Ophthalmology 117(1):120–127
Cao Y et al (2008) Targeting of RGS7/Gbeta5 to the dendritic tips of ON-bipolar cells is independent of its association with membrane anchor R7BP. J Neurosci 28(41):10443–10449
Cheever ML et al (2008) Crystal structure of the multifunctional Gbeta5-RGS9 complex. Nat Struct Mol Biol 15(2):155–162
Vincent A, Robson AG, Holder GE (2013) Pathognomonic (diagnostic) ERGs. A review and update. Retina 33(1):5–12
Vincent A et al (2016) Biallelic mutations in GNB3 cause a unique form of autosomal-recessive congenital stationary night blindness. Am J Hum Genet 98(5):1011–1019
Funding
This work was supported by the Foundation Fighting Blindness, USA (Grant No: CD-CL-0617-0727-HSC). The funding organization had no role in the design or conduct of this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Statement of human rights
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its later amendments.
Statement on the welfare of animals
This article does not contain any studies with animals performed by any of the authors.
Conflict of interest
No conflicting relationships exist for any author.
Informed consent
The patient’s guardian has consented to the submission of the case report to the journal.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Shao, Z., Tumber, A., Maynes, J. et al. Unique retinal signaling defect in GNB5-related disease. Doc Ophthalmol 140, 273–277 (2020). https://doi.org/10.1007/s10633-019-09735-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10633-019-09735-1