
Abstract
Background
Patients with decompensated cirrhosis have high morbidity and are commonly hospitalized with acute kidney injury.
Aims
We examined serum levels of Siglec-7, a transmembrane receptor that regulates immune activity, as a biomarker for mortality in patients with cirrhosis and acute kidney injury.
Methods
Serum Siglec-7 was measured in hospitalized patients with cirrhosis and acute kidney injury, as well as in reference groups with acute liver injury/acute kidney injury, cirrhosis without acute kidney injury, and sepsis without liver disease. Clinical characteristics and subsequent outcomes were examined using univariate and multivariable analyses according to initial Siglec-7 levels. Primary outcome was death by 90 days.
Results
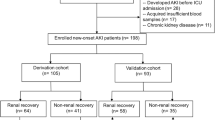
One hundred twenty-eight subjects were included, 92 of which had cirrhosis and acute kidney injury and were used in the primary analysis. Average Model for End-Stage Liver Disease (MELD) score was 24 [95 % CI 23, 26], and serum creatinine was 2.5 [2.2, 2.8] mg/dL at the time Siglec-7 was measured. After adjusting for age and MELD score, high serum Siglec-7 level predicted mortality with a hazard ratio of 1.96 [1.04, 3.69; p = 0.04]. There was no difference in Siglec-7 levels by etiology of AKI (p = 0.24). Addition of serum Siglec-7 to MELD score improved discrimination for 90-day mortality [category-free net reclassification index = 0.38 (p = 0.04); integrated discrimination increment = 0.043 (p = 0.04)].
Conclusion
Serum Siglec-7 was associated with increased mortality among hospitalized patients with cirrhosis and acute kidney injury. Addition of Siglec-7 to MELD score may increase discrimination to predict 90-day mortality.




Similar content being viewed by others


Abbreviations
- MELD:
-
Model for End-Stage Liver Disease
- AKI:
-
Acute kidney injury
- HRS:
-
Hepatorenal syndrome
- AKIN:
-
Acute Kidney Injury Network
- ROC:
-
Receiver operating characteristic
- ANOVA:
-
Analysis of variance
- NRI:
-
Net reclassification index
- IDI:
-
Integrated discrimination index
- APRI:
-
AST to platelet ratio index
References
Garcia-Tsao G, Lim JK. Members of Veterans Affairs Hepatitis C Resource Center Program. Management and treatment of patients with cirrhosis and portal hypertension: recommendations from the Department of Veterans Affairs Hepatitis C Resource Center Program and the National Hepatitis C Program. Am J Gastroenterol. 2009;104:1802–1829.
Murray CJ, Atkinson C, Bhalla K, et al. The state of US health, 1990–2010: burden of diseases, injuries, and risk factors. JAMA. 2013;310:591–608.
Asrani SK, Larson JJ, Yawn B et al. Underestimation of liver-related mortality in the United States. Gastroenterology. 2013;145:375.e1-2–382.e1-2.
Martin-Llahi M, Guevara M, Torre A et al. Prognostic importance of the cause of renal failure in patients with cirrhosis. Gastroenterology. 2011;140:488.e4–496.e4.
Allegretti AS, Ortiz G, Cui J, et al. Changes in kidney function after transjugular intrahepatic portosystemic shunts versus large-volume paracentesis in cirrhosis: A matched cohort analysis. Am J Kidney Dis. 2016;68:381–391. doi:10.1053/j.ajkd.2016.02.041.
Garcia-Tsao G, Parikh CR, Viola A. Acute kidney injury in cirrhosis. Hepatology. 2008;48:2064–2077.
Tsien CD, Rabie R, Wong F. Acute kidney injury in decompensated cirrhosis. Gut. 2013;62:131–137.
Wiesner R, Edwards E, Freeman R, et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology. 2003;124:91–96.
Bernardi M, Gitto S, Biselli M. The MELD score in patients awaiting liver transplant: strengths and weaknesses. J Hepatol. 2011;54:1297–1306.
Gotthardt D, Weiss KH, Baumgartner M et al. Limitations of the MELD score in predicting mortality or need for removal from waiting list in patients awaiting liver transplantation. BMC Gastroenterol. 2009;9:72,230X-9-72.
Crocker PR, Paulson JC, Varki A. Siglecs and their roles in the immune system. Nat Rev Immunol. 2007;7:255–266.
Pillai S, Netravali IA, Cariappa A, et al. Siglecs and immune regulation. Annu Rev Immunol. 2012;30:357–392.
Nicoll G, Ni J, Liu D, et al. Identification and characterization of a novel siglec, siglec-7, expressed by human natural killer cells and monocytes. J Biol Chem. 1999;274:34089–34095.
Varchetta S, Mele D, Lombardi A et al. Lack of Siglec-7 expression identifies a dysfunctional natural killer cell subset associated with liver inflammation and fibrosis in chronic HCV infection. Gut. 2015. doi:10.1136/gutjnl-2015-310327.
Miyazaki K, Sakuma K, Kawamura YI, et al. Colonic epithelial cells express specific ligands for mucosal macrophage immunosuppressive receptors siglec-7 and -9. J Immunol. 2012;188:4690–4700.
Varchetta S, Brunetta E, Roberto A, et al. Engagement of Siglec-7 receptor induces a pro-inflammatory response selectively in monocytes. PLoS One. 2012;7:e45821.
Mitsuki M, Nara K, Yamaji T, et al. Siglec-7 mediates nonapoptotic cell death independently of its immunoreceptor tyrosine-based inhibitory motifs in monocytic cell line U937. Glycobiology. 2010;20:395–402.
Falco M, Biassoni R, Bottino C, et al. Identification and molecular cloning of p75/AIRM1, a novel member of the sialoadhesin family that functions as an inhibitory receptor in human natural killer cells. J Exp Med. 1999;190:793–802.
Yamaji T, Teranishi T, Alphey MS, et al. A small region of the natural killer cell receptor, Siglec-7, is responsible for its preferred binding to alpha 2,8-disialyl and branched alpha 2,6-sialyl residues. A comparison with Siglec-9. J Biol Chem. 2002;277:6324–6332.
Varki A. Since there are PAMPs and DAMPs, there must be SAMPs? Glycan “self-associated molecular patterns” dampen innate immunity, but pathogens can mimic them. Glycobiology. 2011;21:1121–1124.
Delputte PL, Nauwynck HJ. Porcine arterivirus infection of alveolar macrophages is mediated by sialic acid on the virus. J Virol. 2004;78:8094–8101.
Rempel H, Calosing C, Sun B, et al. Sialoadhesin expressed on IFN-induced monocytes binds HIV-1 and enhances infectivity. PLoS One. 2008;3:e1967.
Zou Z, Chastain A, Moir S, et al. Siglecs facilitate HIV-1 infection of macrophages through adhesion with viral sialic acids. PLoS One. 2011;6:e24559.
Varchetta S, Lusso P, Hudspeth K et al. Sialic acid-binding Ig-like lectin-7 interacts with HIV-1 gp120 and facilitates infection of CD4pos T cells and macrophages. Retrovirology. 2013;10:154,4690-10-154.
Brunetta E, Fogli M, Varchetta S, et al. The decreased expression of Siglec-7 represents an early marker of dysfunctional natural killer-cell subsets associated with high levels of HIV-1 viremia. Blood. 2009;114:3822–3830.
Hudak JE, Canham SM, Bertozzi CR. Glycocalyx engineering reveals a Siglec-based mechanism for NK cell immunoevasion. Nat Chem Biol. 2014;10:69–75.
Jandus C, Boligan KF, Chijioke O, et al. Interactions between Siglec-7/9 receptors and ligands influence NK cell-dependent tumor immunosurveillance. J Clin Invest. 2014;124:1810–1820.
Miyazaki K, Ohmori K, Izawa M, et al. Loss of disialyl Lewis(a), the ligand for lymphocyte inhibitory receptor sialic acid-binding immunoglobulin-like lectin-7 (Siglec-7) associated with increased sialyl Lewis(a) expression on human colon cancers. Cancer Res. 2004;64:4498–4505.
Bax M, Kuijf ML, Heikema AP, et al. Campylobacter jejuni lipooligosaccharides modulate dendritic cell-mediated T cell polarization in a sialic acid linkage-dependent manner. Infect Immun. 2011;79:2681–2689.
Kannagi R. Carbohydrate antigen sialyl Lewis a–its pathophysiological significance and induction mechanism in cancer progression. Chang Gung Med J. 2007;30:189–209.
Gines P, Schrier RW. Renal failure in cirrhosis. N Engl J Med. 2009;361:1279–1290.
Wadei HM, Mai ML, Ahsan N, et al. Hepatorenal syndrome: pathophysiology and management. Clin J Am Soc Nephrol. 2006;1:1066–1079.
Adebayo D, Morabito V, Davenport A, et al. Renal dysfunction in cirrhosis is not just a vasomotor nephropathy. Kidney Int. 2015;87:509–515.
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl. 2012;2:1–138.
Salerno F, Gerbes A, Gines P, et al. Diagnosis, prevention and treatment of hepatorenal syndrome in cirrhosis. Gut. 2007;56:1310–1318.
Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580–637.
Moreau R, Jalan R, Gines P et al. Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterology. 2013;144:1426.e1-9–1437.e1-9.
Hajian-Tilaki K. Receiver operating characteristic (ROC) curve analysis for medical diagnostic test evaluation. Casp J Intern Med. 2013;4:627–635.
Kim WR, Biggins SW, Kremers WK, et al. Hyponatremia and mortality among patients on the liver-transplant waiting list. N Engl J Med. 2008;359:1018–1026.
Pencina MJ, D’Agostino RB, Vasan RS. Statistical methods for assessment of added usefulness of new biomarkers. Clin Chem Lab Med. 2010;48:1703–1711.
R Core Team. R: a language and environment for statistical computing 2015.
Poynard T, Munteanu M, Luckina E, et al. Liver fibrosis evaluation using real-time shear wave elastography: applicability and diagnostic performance using methods without a gold standard. J Hepatol. 2013;58:928–935.
Angeli P, Gines P, Wong F, et al. Diagnosis and management of acute kidney injury in patients with cirrhosis: revised consensus recommendations of the International Club of Ascites. Gut. 2015;64:531–537.
Radaeva S, Sun R, Jaruga B, et al. Natural killer cells ameliorate liver fibrosis by killing activated stellate cells in NKG2D-dependent and tumor necrosis factor-related apoptosis-inducing ligand-dependent manners. Gastroenterology. 2006;130:435–452.
Melhem A, Muhanna N, Bishara A, et al. Anti-fibrotic activity of NK cells in experimental liver injury through killing of activated HSC. J Hepatol. 2006;45:60–71.
O’Reilly MK, Paulson JC. Siglecs as targets for therapy in immune-cell-mediated disease. Trends Pharmacol Sci. 2009;30:240–248.
Silva PE, Fayad L, Lazzarotto C, et al. Single-centre validation of the EASL-CLIF consortium definition of acute-on-chronic liver failure and CLIF-SOFA for prediction of mortality in cirrhosis. Liver Int. 2015;35:1516–1523.
Lee M, Lee JH, Oh S, et al. CLIF-SOFA scoring system accurately predicts short-term mortality in acutely decompensated patients with alcoholic cirrhosis: a retrospective analysis. Liver Int. 2015;35:46–57.
Acknowledgments
ASA is supported by NIH Grant 5T32DK007540-30. RTC is supported by NIH Grant K24DK078772. RIT is supported by NIH Grants R01DK094486 and K24DK094872. SAK was supported by funds from the Howard Hughes Medical Institute.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Allegretti, A.S., Ortiz, G., Kalim, S. et al. Siglec-7 as a Novel Biomarker to Predict Mortality in Decompensated Cirrhosis and Acute Kidney Injury. Dig Dis Sci 61, 3609–3620 (2016). https://doi.org/10.1007/s10620-016-4316-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-016-4316-x