
Abstract
Purpose
Unruptured intracranial aneurysms (UIAs) occur in 2–3% of the adult population, but, once discovered, do not always require treatment. Untreated patients are usually followed with serial imaging to identify interval growth. In this study, we assessed the risk and risk factors for growth in a homogenous series of patients with conservatively managed UIAs.
Methods
Data from consecutive patients without history of subarachnoid hemorrhage and a conservatively managed UIA were retrospectively reviewed and only patients with at least 2 years of radiological follow-up were included in our study. We evaluated patients for the incidence of UIA growth, as well as analyzed risk factors for UIA growth.
Results
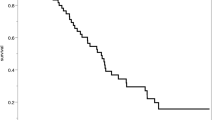
In 349 patients and 385 conservatively managed UIAs with 2210 patient-years of radiological follow-up, the risk of growth was 2.9% per aneurysm-year. Size (diameter greater than 5 mm), location (basilar artery apex), and weight loss (decrease in BMI over follow-up period) were all significantly associated with increased risk of UIA growth. There was a greater risk of UIA growth during the first 3 years of follow-up (7.5% per aneurysm-year) compared to the remaining years (2.7% per aneurysm-year).
Conclusions
Conservatively managed UIAs in patients without prior history of SAH have a 2.9% risk of growth per aneurysm-year. UIAs greater than 5 mm in diameter, those located at the basilar artery apex, or patients who experience a decrease in BMI are more likely to grow and warrant closer follow-up. The risk of aneurysm growth is increased in the few years after diagnosis and decreases afterward.

Similar content being viewed by others


References
Backes D, Rinkel GJE, Greving JP, Velthuis BK, Murayama Y, Takao H, Ishibashi T, Igase M, terBrugge KG, Agid R, Jaaskelainen JE, Lindgren AE, Koivisto T, von Und Zu Fraunberg M, Matsubara S, Moroi J, Wong GKC, Abrigo JM, Igase K, Matsumoto K, Wermer MJH, van Walderveen MAA, Algra A, Vergouwen MDI (2017) ELAPSS score for prediction of risk of growth of unruptured intracranial aneurysms. Neurology 88:1600–1606
Brinjikji W, Zhu YQ, Lanzino G, Cloft HJ, Murad MH, Wang Z, Kallmes DF (2016) Risk factors for growth of intracranial aneurysms: a systematic review and meta-analysis. AJNR Am J Neuroradiol 37:615–620
Burns JD, Huston J 3rd, Layton KF, Piepgras DG, Brown RD Jr (2009) Intracranial aneurysm enlargement on serial magnetic resonance angiography: frequency and risk factors. Stroke 40:406–411
Hilditch CA, Brinjikji W, Tsang AC, Nicholson P, Kostynskyy A, Tymianski M, Krings T, Radovanovic I, Pereira VM (2018) Application of PHASES and ELAPSS scores to ruptured cerebral aneurysms: how many would have been conservatively managed? J Neurosurg Sci. https://doi.org/10.23736/S0390-5616.18.04498-3
Hughes JD, Samarage M, Burrows AM, Lanzino G, Rabinstein AA (2015) Body mass index and aneurysmal subarachnoid hemorrhage: decreasing mortality with increasing body mass index. World Neurosurg 84:1598–1604
Lanzino G (2016) Modern management of intracranial aneurysms. J Neurosurg Sci 60(21)
Lanzino G, Brown RD Jr (2012) Natural history of unruptured intracranial aneurysms. J Neurosurg 117:50–51 discussion 51–52
Mehan WA Jr, Romero JM, Hirsch JA, Sabbag DJ, Gonzalez RG, Heit JJ, Schaefer PW (2014) Unruptured intracranial aneurysms conservatively followed with serial CT angiography: could morphology and growth predict rupture? J Neurointerv Surg 6:761–766
Sandvei MS, Lindekleiv H, Romundstad PR, Muller TB, Vatten LJ, Ingebrigtsen T, Njolstad I, Mathiesen EB, Vik A (2012) Risk factors for aneurysmal subarachnoid hemorrhage - BMI and serum lipids: 11-year follow-up of the HUNT and the Tromso Study in Norway. Acta Neurol Scand 125:382–388
So TY, Dowling R, Mitchell PJ, Laidlaw J, Yan B (2010) Risk of growth in unruptured intracranial aneurysms: a retrospective analysis. J Clin Neurosci 17:29–33
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required. All included patients agreed to be included in our aneurysm research database.
This article does not contain any studies with animals performed by any of the authors.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Comments
This interesting article, from an experienced and scholarly unit, confirms some things that we know and informs us of some that we didn’t know yet.
To make it simple - first, unsurprisingly, unruptured aneurysms enlarge over time. The process is accelerated if the UIA is 5mm or more at discovery. Curiously, these authors show evidence that this growth appears to taper off after a few years (the rate was materially higher in the first three years after discovery). Second, basilar caput aneurysms have a higher growth rate than other sites. Third - and previously unknown to me - weight loss during the observation period is a risk factor for UIA growth.
What they do not report, unfortunately, is the incidence of SAH in this series of elegantly followed UIA’s. This would be useful and fascinating data to know.
The implications of this study are intuitive to anyone who must routinely counsel patients about what to do for a UIA. As for me, my default setting is for treatment, so long as the treatment risk is low. I remain unconvinced that we know enough about UIA’s and their natural history to declare with certainty that any aneurysm is truly innocent.
Christopher M. Loftus
Philadelphia, USA
This article is part of the Topical Collection on Vascular Neurosurgery - Aneurysm
Rights and permissions
About this article

Cite this article
Giordan, E., Sorenson, T.J., Brinjikji, W. et al. Risk factors for growth of conservatively managed unruptured intracranial aneurysms. Acta Neurochir 160, 2419–2423 (2018). https://doi.org/10.1007/s00701-018-3729-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-018-3729-z