
Abstract
The objective of this study was to compare fluid leakage across endotracheal tube cuffs using a three-dimensional (3D)-printed human tracheal model that anatomically simulates the human trachea. We made two models based on computed tomography data of the neck and chest. Using a Mallinckrodt Hi-Lo™ (HL), ThinCuff® (TC), and Mallinckrodt TaperGuard™ (TG), we sequentially measured the amount of fluid leakage across each endotracheal tube cuff after applying saline or viscous liquid above the cuff. The TG allowed significantly less leakage than the HL and TC with both saline and the viscous liquid. Our study, using a 3D-printed tracheal model, indicated that a conical-shaped endotracheal tube cuff significantly reduces fluid leakage across the cuff compared with conventional cylindrical-shaped cuffs made of polyurethane or polyvinylchloride, contrary to the results of a previous study using a solid cylindrical structure.
Introduction
Endotracheal intubation is an essential method to secure the airway. The merits of an endotracheal tube (ETT) include prophylaxis against aspiration of subglottic secretions compared to a laryngeal mask airway, and assurance of ventilatory volume. Critically ill patients frequently require prolonged mechanical ventilation, and consequently, are susceptible to developing ventilator-associated pneumonia (VAP). VAP, in turn, leads to prolonged intensive care unit and hospital stay and increased medical costs [1]. The mechanism of VAP involves microaspiration of contaminated oropharyngeal secretions due to leakage across the ETT cuff [2]. Thus, many manufacturers have developed and designed various types of ETTs to reduce the incidence of VAP. A recent in vitro study on fluid leakage across the ETT cuff indicated that differences in cuff shape and material contribute to the potential for endotracheal sealing [3]. In past studies, including the above-mentioned study, a solid cylindrical structure was used as a substitute for the human trachea [3–5]. Artificial tracheas have a fixed stiffness and diameter, which contribute to standardization of experimental condition. On the other hand, the cross-section of the human trachea is not a perfect circle, but is C-shaped, U-shaped, or elliptical [6]. Furthermore, the inner surface of the trachea has some unevenness due to tracheal cartilage, and some degree of elasticity [7]. Thus, we hypothesized that fluid leakage across the tracheal tube cuff might be affected by whether we employ a three-dimensional (3D)-printed human tracheal model or a conventional cylindrical model. The objective of this study was to compare the amount of fluid leakage across three ETT cuffs using a 3D-printed human tracheal model that accurately simulates human tracheal anatomy.
After institutional approval by Sapporo Medical University School of Medicine, computed tomography (CT) data of the tracheas of the author and co-author, both of whom have no respiratory tract disorders, were used in this prospective study. We also enrolled this study in the UMIN Clinical Trial Registry (trial registration no. UMIN000017292). At first, CT was used to take thin-slice images of our tracheas and the model was made from CT data of the neck and chest. We then manufactured two 3D-printed tracheal models as shown in Fig. 1, reproducing the human trachea from the first tracheal cartilage to the carina. The model on the left is based on CT data of the first author (34-year-old male), and the model on the right is based on CT data of the co-author (51-year-old male). A 3D printer (Objet500 Connex2™; Stratasys Ltd., MN, USA) made it possible to reconstruct CT data of the two participants into 3D tracheal models, using gum-like acrylic compounds mainly containing 2-propenoic acid, 2-[[(butylamino)carbonyl]oxy]ethyl ester and isobornyl acrylate. These materials are translucent and have a relatively similar stiffness to that of the human body, defined as shore A hardness of 25–28. We examined the Mallinckrodt Hi-Lo™ (HL; Covidien, Dublin, Ireland), ThinCuff® (TC; Parker Medical, Highlands Ranch, CO, USA), and Mallinckrodt TaperGuard™ (TG; Covidien) ETTs in this study. The cuff of the HL, which is made of polyvinylchloride (PVC), is a conventional, cylindrical, high-capacity low-pressure cuff. The cylindrical cuff of the TC, which is made of thin polyurethane (PU), is expected to have fewer folds than a PVC cuff. The cuff of the TG tube, which is made of PVC, has a characteristic conical shape. In our study, the tips of all ETTs were placed approximately 3 cm above the carina, as shown in Fig. 1. Next, the pressure in all the ETT cuffs was continuously maintained at 25 cm H2O using a CuffKeeper (Tokuki Giken, Oita, Japan) throughout the study. All the ETTs used had an internal diameter (ID) of 8.0 mm. We applied 10 ml of saline or a viscous liquid (simulated sputum; Kyoto Kagaku, Japan) to simulate subglottic secretions around the cuff. The viscous liquid was diluted three-fold with water. Even though there is no scientific evidence of simulated sputum fidelity, we assumed that this material was clinically acceptable as a subglottic secretion simulant. We sequentially measured the amount of fluid leakage across the cuff at 5 and 10 min after applying the saline solution and at 30 and 60 min after applying the viscous liquid. We measured the amount of fluid leakage dripping from the two holes on the bottom of 3D tracheal model, and the holes represent the cross-sectional surface of the right and left main bronchus. Measurements of each type of tube were repeated ten times in each model to reduce confounding due to the variance of the attachment to the inner surface of the trachea. The primary outcome was the amount of fluid leakage across each type of ETT cuff. All values are shown as median (minimum to maximum) of data from a total of 20 readings. Data were analyzed using the Kruskal–Wallis test and Dunn’s test for post hoc multiple comparisons. A p value of <0.05 was considered statistically significant.

Three-dimensional tracheal models (left one model A, right one model B). Two three-dimensional tracheal models were set vertically and intubated such that the tip of the ETT was located approximately 3 cm above the carina
The following were the major results of this study.
-
1.
Saline solution
We found a significant difference in fluid leakage among the three types of ETTs. The median amounts of leakage (minimum to maximum) at 5 min after applying saline were 7.5 ml (1.0–10) for HL, 6.7 ml (1.6–10) for TC and 0.8 ml (0.3–2.3) for TG. The median amounts of leakage at 10 min after applying saline were 10 ml (2.9–10) for HL, 9.8 ml (2.7–10) for TC and 1.6 ml (0.6–4.0) for TG. At both 5 and 10 min, the TG showed significantly less amounts of leakage than the HL or TC, as shown in Fig. 2a. On the other hand, there was no significant difference between leakage from the HL and TC. Data variance on each tracheal model is almost similar (data not shown).
Fig. 2 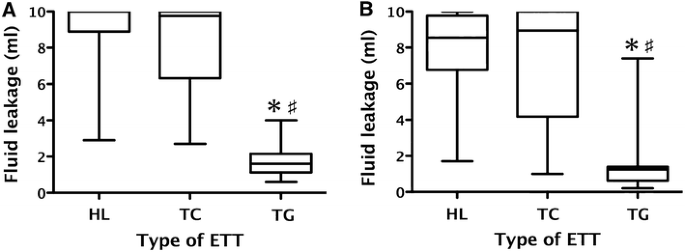
Fluid leakage across the cuffs of the three endotracheal tubes was assessed. a Fluid leakage 10 min after applying saline. b Fluid leakage 60 min after applying a viscous liquid. The amount of fluid leakage across the cuff of the TG endotracheal tube was significantly less than that across the HL or TC. *p < 0.05 vs HL, # p < 0.05 vs TC. HL Mallinckrodt Hi-Lo™, TC ThinCuff®, TG Mallinckrodt TaperGuard™
-
2.
Viscous liquid
The median amounts of leakage (minimum to maximum) at 30 min after applying the viscous liquid were 4.6 ml (1.0–9.8) for HL, 4.9 ml (0.7–10) for TC and 0.8 ml (0.1–4.5) for TG. The median amounts of leakage at 60 min after applying the viscous liquid were 8.6 ml (1.7–10) for HL, 9.0 ml (1.0–10) for TC and 1.3 ml (0.2–7.4) for TG. At both 30 and 60 min, the TG showed significantly less amounts of leakage than the HL or TC, as shown in Fig. 2b. On the other hand, there was no significant difference between leakage from the HL and TC. Data variance on each tracheal model is almost similar (data not shown).
In this study, we compared the amount of fluid leakage with three ETT cuffs using a 3D-printed human tracheal model. We found that the TG showed significantly less amounts of leakage than the HL or TC. Thus, we suggest that a conical-shaped ETT cuff might have superior sealing efficacy than a cylindrical-shaped cuff made of PVC or PU, and that the excellent sealing efficacy of the TG may be attributed to the characteristic shape of the cuff, which has a permanent sealing zone between the cuff and the inner surface of the trachea. However, previous studies have reported that cylindrical PU cuffs had an equal or superior sealing efficacy than conical-shaped PVC cuffs [3–5]. This discrepancy may be partly explained by the difference in the tracheal models used in the evaluations. A thin PU cuff is known to have less folds when it is inflated in the substitute for the human trachea and has superior sealing efficacy [5]. However, a 3D tracheal model has a varying diameter, irregular inner surface and some degree of elasticity unlike a solid cylindrical structure. Thus, we speculated that a PU cuff might not fit when inflated within our 3D tracheal model. The 3D tracheal model in our study is based on human CT data. Therefore, this model can precisely reproduce human anatomical features compared with a solid cylindrical structure, at least in the aspect of tracheal shape. Our results show that a 3D-printed tracheal model has advantages for assessing ETT cuff sealing efficacy and that a 3D tracheal model can also be used in the clinical setting.
However, our study has several limitations. First, the 3D tracheal model in our study was based on CT data from only two healthy males. Our limited sample size may not be sufficient to estimate a statistical difference. Moreover, it is unknown whether a gender-related difference in anatomy of the human trachea affects assessment of ETT sealing efficacy. Second, our 3D tracheal model might not be applicable to individuals with respiratory tract stenosis. Individual anatomical discrepancies of the trachea could lead to a bias. Hence, future studies are needed to validate our results. Third, although our 3D tracheal model accurately simulates human tracheal anatomy, the component of the human trachea is different from our gum-like acrylic compound. Furthermore, we used no lubricant around the cuff, and the 3D tracheal model had no secretion and no ciliary movement on the tracheal wall unlike a human trachea. In other words, our study model has some weakness when reproducing human patients [8].
In conclusion, our study using a 3D-printed tracheal model showed that a conical-shaped ETT cuff significantly reduces fluid leakage across the cuff compared to a conventional cylindrical-shaped cuff made of PU or PVC.
-
2.

References
Rello J, Ollendorf DA, Oster G, Vera-Llonch M, Bellm L, Redman R, Kollef MH. VAP Outcomes Scientific Advisory Group. Epidemiology and outcomes of ventilator-associated pneumonia in a large US database. Chest. 2002;122:2115–21.
Estes RJ, Meduri GU. The pathogenesis of ventilator-associated pneumonia: I. Mechanisms of bacterial transcolonization and airway inoculation. Intensive Care Med. 1995;21:365–83.
Zanella A, Scaravilli V, Isgrò S, Milan M, Cressoni M, Patroniti N, Fumagalli R, Pesenti A. Fluid leakage across tracheal tube cuff, effect of different cuff material, shape, and positive expiratory pressure: a bench-top study. Intensive Care Med. 2011;37:343–7.
Li Bassi G, Ranzani OT, Marti JD, Giunta V, Luque N, Isetta V, Ferrer M, Farre R, Pimentel GL, Torres A. An in vitro study to assess determinant features associated with fluid sealing in the design of endotracheal tube cuffs and exerted tracheal pressures. Crit Care Med. 2013;41:518–26.
Dullenkopf A, Gerber A, Weiss M. Fluid leakage past tracheal tube cuffs: evaluation of the new microcuff endotracheal tube. Intensive Care Med. 2003;29:1849–53.
Mehta S, Myat HM. The cross-sectional shape and circumference of the human trachea. Ann R Coll Surg Engl. 1984;66:356–8.
Trabelsi O, del Palomar AP, López-Villalobos JL, Ginel A, Doblaré M. Experimental characterization and constitutive modeling of the mechanical behavior of the human trachea. Med Eng Phys. 2010;32(1):76–82.
Schebesta K, Hüpfl M, Rössler B, Ringl H, Müller MP, Kimberger O. Degrees of reality: airway anatomy of high-fidelity human patient simulators and airway trainers. Anesthesiology. 2012;116:1204–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Tomohiko Kimijima, Mitsutaka Edanaga, and Michiaki Yamakage have no conflict of interest.
About this article

Cite this article
Kimijima, T., Edanaga, M. & Yamakage, M. Comparison of fluid leakage across endotracheal tube cuffs using a three-dimensional printed model of the human trachea. J Anesth 30, 510–513 (2016). https://doi.org/10.1007/s00540-016-2138-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-016-2138-9