
Abstract
Background
Malignant gastric outlet obstruction represents a terminal stage in pancreatic cancer. Between 5% and 25% of patients with pancreatic cancer ultimately experience malignant gastric outlet obstruction. The aim in palliating patients with malignant gastric outlet obstruction is to reestablish an oral intake by restoring gastrointestinal continuity. This ultimately improves their quality of life in the advanced stages of cancer. The main drawback to operative bypass is the high incidence of delayed gastric emptying, particularly in this group of patients with symptomatic obstruction. This study aimed to compare surgical gastrojejunostomy and endoscopic stenting in palliation of malignant gastric outlet obstruction, acknowledging the diversity and heterogeneity of patients with this presentation.
Methods
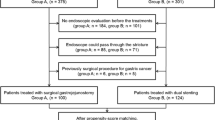
This retrospective study investigated patients treated for malignant gastric outlet obstruction from December 1998 to November 2008 at Nepean Hospital, Sydney, Australia. Endoscopic duodenal stenting was performed under fluoroscopic guidance for placement of the stent. The operative patients underwent open surgical gastrojejunostomy. The outcomes assessed included time to diet, hospital length of stay (LOS), biliary drainage procedures, morbidity, and mortality.
Results
Of the 45 participants in this study, 26 underwent duodenal stenting and 19 had operative bypass. Comparing the stenting and operative patients, the median time to fluid intake was respectively 0 vs. 7 days (P < 0.001), and the time to intake of solids was 2 vs. 9 days (P = 0.004). The median total LOS was shorter in the stenting group (11 vs. 25 days; P < 0.001), as was the median postprocedure LOS (5 vs. 10 days; P = 0.07).
Conclusions
Endoscopic stenting is preferable to operative gastrojejunostomy in terms of shorter LOS, faster return to fluids and solids, and reduced morbidity and in-hospital mortality for patients with a limited life span.



Similar content being viewed by others


References
Watanapa P, Williamson RC (1992) Surgical palliation for pancreatic cancer: developments during the past two decades. Br J Surg 79:8–20
Sarr MG, Cameron JL (1982) Surgical management of unresectable carcinoma of the pancreas. Surgery 91:123–133
Singh SM, Longmire WP Jr, Reber HA (1990) Surgical palliation for pancreatic cancer: the UCLA experience. Ann Surg 212:132–139
Lillemoe KD, Cameron JL, Hardacre JM, Sohn TA, Sauter PK, Coleman J, Pitt JA, Yeo CJ (1999) Is prophylactic gastrojejunostomy indicated for unresectable periampullary cancer? A prospective randomised trial. Ann Surg 230:322
Maetani I, Ogawa S, Hoshi H, Sato M, Yoshioka H, Igarashi Y, Sakai Y (1994) Self-expanding metal stents for palliative treatment of malignant biliary and duodenal stenoses. Endoscopy 26:701–704
Truong S, Bohndorf H, Geller H, Schumpelick V, Gunther RW (1992) Self- expanding metal stents for palliation of malignant gastric outlet obstruction. Endoscopy 24:433–435
Keymling M, Wagner HJ, Vakil N, Knyrim K (1993) Relief of malignant duodenal obstruction by percutaneuous insertion of a metal stent. Gastrointest Endosc 39:439–441
Song Hy, Yang DH, Kuh JH, Choi KC (1993) Obstructing cancer of the gastric antrum: palliative treatment with covered metallic stents. Radiology 187:357–358
Mauro MA, Koehler RE, Baron TH (2000) Advances in gastrointestinal intervention: the treatment of gastroduodenal and colorectal obstructions with metallic stents. Radiology 215:659–669
Yim HB, Jacobson BC, Saltzman JR, Johannes RS, Bounds BCm Lee JH, Shields SJ, Ruymann FW, Van Dam J, Carr-Locke DL (2001) Clinical outcome of the use enteral stents for palliation of patients with malignant upper GI obstruction. Gastrointest Endosc 53:329–332
Wong YT, Brams DM, Munson L, Sanders L, Heiss F, Chase M, Birkett DH (2002) Gastric outlet obstruction secondary to pancreatic cancer: surgical vs endoscopic palliation. Surg Endosc 16(2):310–312
Maetani I, Tada T, Shimura J, Ukita T, Inoue H, Igarashi Y, Hoshi H, Sakai Y (2002) Technical modification and strategies for stenting gastric outlet strictures using oesophageal endoprosthesis. Endoscopy 34:402–406
Maetani I, Tada T, Ukida T, Inoue H, Sakai Y, Yoshikawa M (2004) Comparison of duodenal stent placement with surgical gastrojejunostomy for palliation in patients with duodenal obstructions caused by pancreaticobiliary malignancies. Endoscopy 36:73–78
Dormann A, Meisner S, Verin N, Wenk Lang A (2004) Self- expanding metal stents for gastroduodenal malignancies: systematic review of their clinical effectiveness. Endoscopy 36:543–550
Weaver DW, Wiencek RG, Bouwman DL, Walt AJ (1987) Gastrojejunostomy: is it helpful for patients with pancreatic cancer? Surgery 102:608–613
Mehta S, Hindmarsh A, Cheong E, Cockburn J, Saada J, Tighe R, Lewis MPN, Rhodes M (2006) Prospective randomized trial of laparoscopic gastrojejunostomy versus duodenal stenting for malignant gastric outflow obstruction. Surg Endosc 20:239–242
Doberneck RC, Berndt GA (1987) Delayed gastric emptying after palliative gastrojejunostomy for carcinoma of the pancreas. Arch Surg 122:827–829
Acknowledgments
This study was supported by a Nepean Medical Research Foundation Project Grant. We acknowledge the contribution to this study by the late Professor Christopher J. Martin, MBBS (Hons), FRACS, MSc, BSc (Hons), who was an admired and beloved surgeon in the unit.
Disclosures
Manju D. Chandrasegaram, Guy D. Eslick, Clare O. Mansfield, Han Liem, Mark Richardson, Sulman Ahmed, and Michael R. Cox have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chandrasegaram, M.D., Eslick, G.D., Mansfield, C.O. et al. Endoscopic stenting versus operative gastrojejunostomy for malignant gastric outlet obstruction. Surg Endosc 26, 323–329 (2012). https://doi.org/10.1007/s00464-011-1870-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-011-1870-3