
Abstract
Objective
To assess the conspicuity of invasive carcinomas (solid masses) originating from pancreatic intraductal papillary mucinous neoplasms (invasive IPMNs) and the primary sites of the solid masses on thin-slice dynamic CT.
Methods
Twenty patients with pathologically proven invasive IPMNs underwent triple-phase dynamic CT examinations (arterial, portal, and delayed phases). Qualitative and quantitative analyses of conspicuity of the solid masses were performed for all phases. The primary sites [branch duct and/or main pancreatic duct (MPD)] of the solid masses were evaluated on CT in comparison to the pathologic findings.
Results
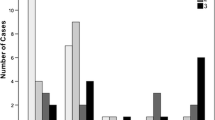
The qualitative and quantitative analyses of the conspicuity of the solid masses showed that the arterial phase images were superior to those of the portal and delayed phases. The primary sites of the solid mass were histopathologically diagnosed as branch ducts in 6 (30%) patients, MPD in 13 (65%), and both branch ducts and the MPD in one (5%). The sensitivity and specificity of the CT evaluation of the primary sites were 100% for the branch ducts, and for the MPD 93% and 100%, respectively.
Conclusion
Arterial phase images are useful for the diagnosis of invasive IPMNs, and attention should be paid to pancreatic parenchyma surrounding the MPD when detecting invasive carcinomas.



Similar content being viewed by others


References
Rickaert F, Cremer M, Deviere J, et al. (1991) Intraductal mucin hypersecreting neoplasms of the pancreas. Gastroenterology 101:512–519
Loftus EV, Olivares-Pakzad BA, Batts KP, et al. (1996) Intraductal papillary-mucinous tumors of the pancreas: clinicopathologic features, outcome, and nomenclature. Gastroenterology 110:1909–1918
Morohoshi T, Kanda M, Asamura K, et al. (1989) Intraductal papillary neoplasms of the pancreas. A clinicopathologic study of six patients. Cancer 64:1329–1335
Tanaka M (2004) Intraductal papillary mucinous neoplasm of the pancreas: diagnosis and treatment. Pancreas 28:282–288
Farrell JL, Brugge WR (2002) Intraductal papillary mucinous tumor of the pancreas. Gastrointest Endosc 55:701–714
Kloppel G, Solcia E, Longnecker DS, et al. (1996) Histological typing of tumours of the exocrine pancreas: WHO International histological classification of tumours, 2nd edn. Berlin: Springer
Solcia E, Capella C, Kloppel G (1997) Intraductal papillary-mucinous tumor. In: Rosai J (ed) Atlas of tumor pathology. Tumor of the pancreas. Washington, DC: AFIP, pp 53–64
Sohn TA, Yeo CJ, Cameron JL, et al. (2004) Intraductal papillary mucinous neoplasms of the pancreas: an updated experience. Ann Surg 239:788–799
Fukukura Y, Fujiyoshi F, Sasaki M, et al. (2000) Intraductal papillary mucinous tumors of the pancreas: thin section helical CT findings. AJR 174:441–447
Taouli B, Vilgrain V, Vullierme MP, et al. (2000) Intraductal papillary mucinous tumors of the pancreas: helical CT with histopathologic correlation. Radiology 217:757–764
Kawamoto S, Lawler LP, Horton KM, et al. (2006) MDCT of intraductal papillary mucinous neoplasm of the pancreas: evaluation of features predictive of invasive carcinoma. AJR 186:687–695
Vullierme MP, Giraud-Cohen M, Hammel P (2007) Malignant intraductal papillary mucinous neoplasm of the pancreas: in situ versus invasive carcinoma surgical resectability. Radiology 245:483–490
Yamada Y, Mori H, Matsumoto S, Kamei N, Hongo N (2006) Invasive carcinomas originated from intraductal papillary mucinous neoplasms of the pancreas: a long-term follow-up assessment with CT imaging. J Comput Assist Tomogr 30:885–890
Yamada Y, Mori H, Matsumoto S (2008) Intraductal papillary mucinous neoplasms of the pancreas: correlation of helical CT and dynamic MR imaging features with pathologic findings. Abdom Imaging 33:474–481
Kitagawa Y, Unger TA, Taylor S, Kozarek RA, Traverso LW (2003) Mucus is a predictor of better prognosis and survival in patients with intraductal papillary mucinous tumor of the pancreas. J Gastrointest Surg 7:12–19
Salvia R, Fernández-del Castillo C, Bassi C (2004) Main-duct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and long-term survival following resection. Ann Surg 239:678–687
Sugiyama M, Atomi Y (1998) Intraductal papillary mucinous tumors of the pancreas: imaging studies and treatment strategies. Ann Surg 228:685–691
Landis JR, Koch GG (1977) An application of hierarchical kappa-type statistics in the assessment of majority agreement among multiple observers. Biometrics 33:363–374
Hale CA, Fleiss JL (1993) Interval estimation under two study designs for kappa with binary classifications. Biometrics 49:523–534
Longnecker DS (1998) Observations on the etiology and pathogenesis of intraductal papillary-mucinous neoplasms of the pancreas. Hepatogastroenterology 45:1973–1980
Adsay NV, Longnecker DS, Klimstra DS (2000) Pancreatic tumors with cystic dilatation of the ducts: intraductal papillary mucinous neoplasms and intraductal oncocytic papillary neoplasms. Semin Diagn Pathol 17:16–30
Adsay NV, Conlon KC, Zee SY, Brennan MF, Klimstra DS (2002) Intraductal papillary-mucinous neoplasms of the pancreas: an analysis of in situ and invasive carcinomas in 28 patients. Cancer 94:62–77
Kloppel G (1998) Clinicopathologic view of intraductal papillary-mucinous tumor of the pancreas. Hepatogastroenterology 45:1981–1985
Boland GW, O’Malley ME, Saez M, et al. (1999) Pancreatic-phase versus portal vein-phase helical CT of the pancreas: optimal temporal window for evaluation of pancreatic adenocarcinoma. AJR 172:605–608
McNulty NJ, Francis IR, Platt JF, et al. (2001) Multi-detector row helical CT of the pancreas: effect of contrast-enhanced multiphasic imaging on enhancement of the pancreas, peripancreatic vasculature, and pancreatic adenocarcinoma. Radiology 220:97–102
Bluemke DA, Cameron JL, Hruban RH, et al. (1995) Potentially respectable pancreatic adenocarcinoma: spiral CT assessment with surgical and pathologic correlation. Radiology 197:381–385
Furukawa H, Takayasu K, Mukai K, et al. (1996) Late contrast-enhanced CT for small pancreatic carcinoma: delayed enhanced area on CT with histopathological correlation. Hepatogastroenterology 43:1230–1237
Demachi H, Matsui O, Kobayashi S, et al. (1997) Histological influence on contrast-enhanced CT of pancreatic ductal adenocarcinoma. J Comput Assist Tomogr 21:980–985
Kobari M, Egawa S, Shibuya K, et al. (1999) Intraductal papillary mucinous tumors of the pancreas comprise 2 clinical subtypes: differences in clinical characteristics and surgical management. Arch Surg 134:1131–1136
Terris B, Ponsot P, Paye F, et al. (2000) Intraductal papillary mucinous tumors of the pancreas confined to secondary ducts show less aggressive pathologic features as compared with those involving the main pancreatic duct. Am J Surg Pathol 24:1372–1377
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yamada, Y., Mori, H., Matsumoto, S. et al. Invasive carcinomas originating from intraductal papillary mucinous neoplasms of the pancreas: conspicuity and primary sites of the solid masses on triple-phase dynamic CT imaging. Abdom Imaging 35, 181–188 (2010). https://doi.org/10.1007/s00261-009-9580-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-009-9580-1