
Abstract
Summary
Retrospective claims analysis indicated that high levels of daily and cumulative doses of systemic glucocorticoids were associated with elevated fracture risk in a large cohort of new RA patients under age 65. Heightened risk began to decline within months of discontinuation. Findings were similar among patients age <50 years.
Introduction
We evaluated the impact of systemic glucocorticoid exposure on fracture risk among relatively young patients with new-onset rheumatoid arthritis (RA).
Methods
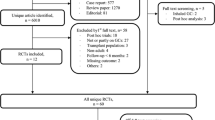
Using administrative data, we identified 42,127 RA patients diagnosed January 1, 2005–December 31, 2012, age 18–64 years, with benefits coverage for ≥12 months before RA diagnosis. Follow-up extended to clinical fracture, cancer diagnosis, or December 31, 2012. Glucocorticoid users were new to therapy. Fracture incidence rates (IR) were stratified by glucocorticoid exposure expressed as prednisone equivalent doses. Cox’s proportional hazards models estimated fracture risk adjusted for demographics and baseline clinical characteristics to assess dose-response relationships with current (daily) and prior (cumulative) dose, and by time since discontinuation.
Results
Most patients (85 %) had glucocorticoid exposure. Exposed and unexposed patients were demographically similar (74 % female; mean age 49.7 and 48.8 years); 1 % had prior fracture. Fracture IRs (95 % confidence intervals) were 5 to 9 per 1000 person-years at doses <15 mg/day, 16.0 (11.0, 22.6) at doses ≥15 mg/day, and 13.4 (10.7, 16.7) at cumulative doses ≥5400 mg. Adjusted fracture risk was approximately 2-fold higher at highest dose levels compared with 0 mg/day current daily dose and <675 mg cumulative dose, respectively. Fracture risk was 29 % lower at 60–182 days post-discontinuation compared with ongoing use and was similar to unexposed patients by 12 months. Findings were similar among patients age <50 years.
Conclusions
Among younger, new-onset RA patients, fracture risk was significantly elevated at high levels of daily and cumulative dose, and was similar to unexposed patients by 12 months post-discontinuation.


Similar content being viewed by others

References
Kirwan J, Power L (2007) Glucocorticoids: action and new therapeutic insights in rheumatoid arthritis. Curr Opin Rheumatol 19(3):233–7. doi:10.1097/BOR.0b013e3280d6471a
van Everdingen AA, Jacobs JW (2002) Siewertsz Van Reesema DR, Bijlsma JW. Low-dose prednisone therapy for patients with early active rheumatoid arthritis: clinical efficacy, disease-modifying properties, and side effects: a randomized, double-blind, placebo-controlled clinical trial. Ann Intern Med 136(1):1–12
Van Staa TP, Leufkens HG, Abenhaim L, Zhang B, Cooper C (2000) Use of oral corticosteroids and risk of fractures. J Bone Miner Res Off J Am Soc Bone Miner Res 15(6):993–1000. doi:10.1359/jbmr.2000.15.6.993
van Staa TP, Leufkens HG, Abenhaim L, Zhang B, Cooper C (2000) Oral corticosteroids and fracture risk: relationship to daily and cumulative doses. Rheumatology 39(12):1383–9
Hoes JN, Jacobs JW, Hulsmans HM, De Nijs RN, Lems WF, Bruyn GA et al (2010) High incidence rate of vertebral fractures during chronic prednisone treatment, in spite of bisphosphonate or alfacalcidol use. Extension of the alendronate or alfacalcidol in glucocorticoid-induced osteoporosis-trial. Clin Exp Rheumatol 28(3):354–9
Pereira RM, Carvalho JF, Canalis E (2010) Glucocorticoid-induced osteoporosis in rheumatic diseases. Clinics 65(11):1197–205
Lukert BP, Raisz LG (1994) Glucocorticoid-induced osteoporosis. Rheum Dis Clin N Am 20(3):629–50
Angeli A, Guglielmi G, Dovio A, Capelli G, de Feo D, Giannini S et al (2006) High prevalence of asymptomatic vertebral fractures in post-menopausal women receiving chronic glucocorticoid therapy: a cross-sectional outpatient study. Bone 39(2):253–9. doi:10.1016/j.bone.2006.02.005
Van Staa TP, Laan RF, Barton IP, Cohen S, Reid DM, Cooper C (2003) Bone density threshold and other predictors of vertebral fracture in patients receiving oral glucocorticoid therapy. Arthritis Rheum 48(11):3224–9. doi:10.1002/art.11283
De Vries F, Bracke M, Leufkens HG, Lammers JW, Cooper C, Van Staa TP (2007) Fracture risk with intermittent high-dose oral glucocorticoid therapy. Arthritis Rheum 56(1):208–14. doi:10.1002/art.22294
Kanis JA, Johnell O, Oden A, Borgstrom F, Zethraeus N, De Laet C et al (2004) The risk and burden of vertebral fractures in Sweden. Osteoporos Int: a J Established Result Cooperation Between Eur Found Osteoporos Natl Osteoporos Found USA 15(1):20–6. doi:10.1007/s00198-003-1463-7
Donnan PT, Libby G, Boyter AC, Thompson P (2005) The population risk of fractures attributable to oral corticosteroids. Pharmacoepidemiol Drug Saf 14(3):177–86. doi:10.1002/pds.1075
Steinbuch M, Youket TE, Cohen S (2004) Oral glucocorticoid use is associated with an increased risk of fracture. Osteoporos Int: a J Established Result Cooperation Between Eur Found Osteoporos Natl Osteoporos Found USA 15(4):323–8. doi:10.1007/s00198-003-1548-3
Majumdar SR, Morin SN, Lix LM, Leslie WD (2013) Influence of recency and duration of glucocorticoid use on bone mineral density and risk of fractures: population-based cohort study. Osteoporos Int: a J Established Result Cooperation Between Eur Found Osteoporos Natl Osteoporos Found USA 24(9):2493–8. doi:10.1007/s00198-013-2352-3
van Staa TP, Geusens P, Bijlsma JW, Leufkens HG, Cooper C (2006) Clinical assessment of the long-term risk of fracture in patients with rheumatoid arthritis. Arthritis Rheum 54(10):3104–12. doi:10.1002/art.22117
McEvoy CE, Ensrud KE, Bender E, Genant HK, Yu W, Griffith JM et al (1998) Association between corticosteroid use and vertebral fractures in older men with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 157(3 Pt 1):704–9. doi:10.1164/ajrccm.157.3.9703080
Walsh LJ, Wong CA, Oborne J, Cooper S, Lewis SA, Pringle M et al (2001) Adverse effects of oral corticosteroids in relation to dose in patients with lung disease. Thorax 56(4):279–84
Dykman TR, Gluck OS, Murphy WA, Hahn TJ, Hahn BH (1985) Evaluation of factors associated with glucocorticoid-induced osteopenia in patients with rheumatic diseases. Arthritis Rheum 28(4):361–8
Sambrook PN, Cohen ML, Eisman JA, Pocock NA, Champion GD, Yeates MG (1989) Effects of low dose corticosteroids on bone mass in rheumatoid arthritis: a longitudinal study. Ann Rheum Dis 48(7):535–8
Buckley LM, Leib ES, Cartularo KS, Vacek PM, Cooper SM (1997) Effects of low dose methotrexate on the bone mineral density of patients with rheumatoid arthritis. J Rheumatol 24(8):1489–94
Tattersfield AE, Harrison TW, Hubbard RB, Mortimer K (2004) Safety of inhaled corticosteroids. Proc Am Thorac Soc 1(3):171–5. doi:10.1513/pats.200402-016MS
Godschalk MF, Downs RW (1988) Effect of short-term glucocorticoids on serum osteocalcin in healthy young men. J Bone Miner Res Off J Am Soc Bone Miner Res 3(1):113–5. doi:10.1002/jbmr.5650030117
Grossman JM, Gordon R, Ranganath VK, Deal C, Caplan L, Chen W et al (2010) American College of Rheumatology 2010 recommendations for the prevention and treatment of glucocorticoid-induced osteoporosis. Arthritis Care Res 62(11):1515–26. doi:10.1002/acr.20295
Curtis JR, Mudano AS, Solomon DH, Xi J, Melton ME, Saag KG (2009) Identification and validation of vertebral compression fractures using administrative claims data. Med Care 47(1):69–72. doi:10.1097/MLR.0b013e3181808c05
Ray WA, Griffin MR, Fought RL, Adams ML (1992) Identification of fractures from computerized Medicare files. J Clin Epidemiol 45(7):703–14
Baron JA, Lu-Yao G, Barrett J, McLerran D, Fisher ES (1994) Internal validation of Medicare claims data. Epidemiology 5(5):541–4
Faraone SV (2008) Interpreting estimates of treatment effects: implications for managed care. P & T: a Peer-Rev J Formul Manag 33(12):700–11
Singh JA, Furst DE, Bharat A, Curtis JR, Kavanaugh AF, Kremer JM et al (2012) 2012 update of the 2008 American College of Rheumatology recommendations for the use of disease-modifying antirheumatic drugs and biologic agents in the treatment of rheumatoid arthritis. Arthritis Care Res 64(5):625–39. doi:10.1002/acr.21641
Deyo RA, Cherkin DC, Ciol MA (1992) Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol 45(6):613–9
van Staa TP, Leufkens HG, Cooper C (2002) The epidemiology of corticosteroid-induced osteoporosis: a meta-analysis. Osteoporos Int: a J Established Result Cooperation Between Eur Found Osteoporos Natl Osteoporos Found USA 13(10):777–87. doi:10.1007/s001980200108
Amin S, Achenbach SJ, Atkinson EJ, Khosla S, Melton LJ 3rd (2014) Trends in fracture incidence: a population-based study over 20 years. J Bone Min Res Off J Am Soc Bone Miner Res 29(3):581–9. doi:10.1002/jbmr.2072
Wade SW, Strader C, Fitzpatrick LA, Anthony MS (2012) Sex- and age-specific incidence of non-traumatic fractures in selected industrialized countries. Arch Osteoporos 7:219–27. doi:10.1007/s11657-012-0100-5
Haugeberg G, Uhlig T, Falch JA, Halse JI, Kvien TK (2000) Bone mineral density and frequency of osteoporosis in female patients with rheumatoid arthritis: results from 394 patients in the Oslo County Rheumatoid Arthritis register. Arthritis Rheum 43(3):522–30. doi:10.1002/1529-0131(200003)43:3<522::AID-ANR7>3.0.CO;2-Y
Haugeberg G, Uhlig T, Falch JA, Halse JI, Kvien TK (2000) Reduced bone mineral density in male rheumatoid arthritis patients: frequencies and associations with demographic and disease variables in ninety-four patients in the Oslo County Rheumatoid Arthritis Register. Arthritis Rheum 43(12):2776–84. doi:10.1002/1529-0131(200012)43:12<2776::AID-ANR18>3.0.CO;2-N
Hauser B, Riches PL, Wilson JF, Horne AE, Ralston SH (2014) Prevalence and clinical prediction of osteoporosis in a contemporary cohort of patients with rheumatoid arthritis. Rheumatology. doi:10.1093/rheumatology/keu162
Dennison EM, Compston JE, Flahive J, Siris ES, Gehlbach SH, Adachi JD et al (2012) Effect of co-morbidities on fracture risk: findings from the Global Longitudinal Study of Osteoporosis in Women (GLOW). Bone 50(6):1288–93. doi:10.1016/j.bone.2012.02.639
Sinigaglia L, Nervetti A, Mela Q, Bianchi G, Del Puente A, Di Munno O et al (2000) A multicenter cross sectional study on bone mineral density in rheumatoid arthritis. Italian Study Group on Bone Mass in Rheumatoid Arthritis. J Rheumatol 27(11):2582–9
Curtis JR, Westfall AO, Allison JJ, Becker A, Casebeer L, Freeman A et al (2005) Longitudinal patterns in the prevention of osteoporosis in glucocorticoid-treated patients. Arthritis Rheum 52(8):2485–94. doi:10.1002/art.21194
Caplan L, Hines AE, Williams E, Prochazka AV, Saag KG, Cunningham F et al (2011) An observational study of glucocorticoid-induced osteoporosis prophylaxis in a national cohort of male veterans with rheumatoid arthritis. Osteoporos Int: a J Established Result Cooperation Between Eur Found Osteoporos Natl Osteoporos Found USA 22(1):305–15. doi:10.1007/s00198-010-1201-x
Majumdar SR, Lix LM, Yogendran M, Morin SN, Metge CJ, Leslie WD (2012) Population-based trends in osteoporosis management after new initiations of long-term systemic glucocorticoids (1998-2008). J Clin Endocrinol Metab 97(4):1236–42. doi:10.1210/jc.2011-2645
McKeown E, Bykerk VP, De Leon F, Bonner A, Thorne C, Hitchon CA et al (2012) Quality assurance study of the use of preventative therapies in glucocorticoid-induced osteoporosis in early inflammatory arthritis: results from the CATCH cohort. Rheumatology 51(9):1662–9. doi:10.1093/rheumatology/kes079
Acknowledgments
The authors are grateful for the statistical and data analysis contributions of Michael Lane and Lang Chen.
Author contributions
Study design, data interpretation, manuscript revisions, final manuscript approval: all authors. Manuscript drafting, accountability for manuscript content and data integrity: AK and SWW.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
This work was supported by Amgen, Inc. Dr. Balasubramanian is an employee and stockholder of Amgen, Inc. Drs. O’Malley and Lin also own stock and were employed by Amgen, Inc. during the study. Ms. Wade is a partner in Wade Outcomes Research and Consulting and has received consulting fees from Amgen Inc. Dr. Adler is employed by the Department of Veterans’ Affairs. Dr. Maricic is employed by the Catalina Pointe Rheumatology. Drs. Curtis and Saag are employed by the University of Alabama at Birmingham and have both received consulting fees from Amgen, Inc. Drs. Curtis and Saag have also received research grants from Amgen, Inc.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Table 1
(DOCX 14 kb)
Supplementary Table 2
(DOCX 28 kb)
Supplementary Table 3
(DOCX 24 kb)
Supplementary Table 4
(DOCX 16 kb)
Rights and permissions
About this article

Cite this article
Balasubramanian, A., Wade, S.W., Adler, R.A. et al. Glucocorticoid exposure and fracture risk in patients with new-onset rheumatoid arthritis. Osteoporos Int 27, 3239–3249 (2016). https://doi.org/10.1007/s00198-016-3646-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-016-3646-z