
Abstract
Objective
Asymmetry in odontoid-lateral mass interspace in trauma patients is a common finding that regularly leads to additional diagnostic work-up, since its dignity is not entirely clear. There is little evidence in the literature that atlantoaxial asymmetry is associated with C1–C2 instability or (sub) luxation. Asymmetry in odontoid-lateral mass interspace seems to occur occasionally in healthy individuals and patients suffering a cervical spine injury. Congenital abnormalities in odontoid-lateral mass asymmetry may mimic an atlantoaxial asymmetry. The center of C1–C2 rotation is based in the peg of dens axis; therefore, a C1–C2 rotational influence seems unlikely. So far, no study examined the influence of C0–C1–C2 tilt to an asymmetry in odontoid-lateral mass interspace.
Subjects and methods
In order to determine if rotation or tilt influences the lateral atlantodental interval (LADI) and to estimate physiologic values, we examined 300 CT scans of the cervical spine.
Results
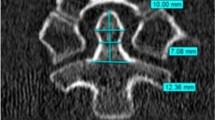
The mean LADI was 3.57 mm and the mean odontoid-lateral mass asymmetry was 1.0 mm. Head position during CT examination was found to be rotated in 39 % of the cases in more than 5°. Subsequent mean C0/C2 rotation was 4.6°. There was no significant correlation between atlantoaxial asymmetry and head rotation (p = 0.437). The average tilt of C0–C1–C2 was found to be 2°. We found a significant correlation between tilt of C0–C1–C2 and asymmetry in odontoid-lateral mass interspace (p = 0.000).
Conclusion
We conclude that an atlantoaxial asymmetry revealed in CT scans of the cervical spine occurs occasionally. Since head tilt correlates with an atlantoaxial asymmetry, it is crucial to perform cervical spine CT scans in a precise straight head position.



Similar content being viewed by others


References
Bland JH. Rheumatoid arthritis of the cervical spine. Bull Rheum Dis. 1967;18(2):471–6.
Bland JH. Rheumatoid subluxation of the cervical spine. J Rheumatol. 1990;17:134–7.
White AA 3rd, Panjabi MM. The basic kinematics of the human spine. A review of past and current knowledge. Spine (Phila Pa 1976). 1978;3:12–20.
Maile S, Slongo T. Atlantoaxial rotatory subluxation: realignment and discharge within 48 h. Eur J Emerg Med. 2007;14:167–9.
Dumas JL, Thoreux P, Attali P, Goldlust D, Chevrel JP. Three-dimensional CT analysis of atlantoaxial rotation: results in the normal subject. Surg Radiol Anat. 1994;16:199–204.
Mazzara JT, Fielding JW. Effect of C1–C2 rotation on canal size. Clin Orthop Relat Res. 1988;237:115–9.
Roy PV. Left-right asymmetries and other common anatomical variants of the first cervical vertebra Part 1 Left-right asymmetries in 1 vertebrae. Manual Therapy. 1997.
Chen Y, Zhuang Z, Qi W, et al. A three-dimensional study of the atlantodental interval in a normal Chinese population using reformatted computed tomography. Surg Radiol Anat. 2011;33:801–6.
Monu J, Bohrer SP, Howard G. Some upper cervical spine norms. Spine (Phila Pa 1976). 1987;12:515–19.
Iannacone WM, DeLong WG Jr, Born CT, Bednar JM, Ross SE. Dynamic computerized tomography of the occiput-atlas-axis complex in trauma patients with odontoid lateral mass asymmetry. J Trauma. 1990;30:1501–5.
Lee S, Joyce S, Seeger J. Asymmetry of the odontoid-lateral mass interspaces: a radiographic finding of questionable clinical significance. Ann Emerg Med. 1986;15:1173–6.
Sutherland JP Jr., Yaszemski MJ, White AA 3rd. Radiographic appearance of the odontoid lateral mass interspace in the occipitoatlantoaxial complex. Spine (Phila Pa 1976). 1995;20:2221–225.
Harty JA. Odontoid lateral mass asymmetry: do we over-investigate? Emerg Med J. 2005;22:625–7.
Fielding JW, Hawkins RJ. Atlanto-axial rotatory fixation. (Fixed rotatory subluxation of the atlanto-axial joint). J Bone Joint Surg Am. 1977;59:37–44.
Ellis GL. Imaging of the atlas (C1) and axis (C2). Emerg Med Clin North Am. 1991;9:719–32.
Wortzman G, Dewar FP. Rotary fixation of the atlantoaxial joint: Rotational atlantoaxial subluxation. Radiology. 1968;90(3):479–87.
Hosalkar HS. Congenital osseous anomalies of the upper cervical spine. J Bone Joint Surg (Am). 2008;90(2):337.
Roche C. The Atlanto-axial joint physiological range of rotation on MRI and CT. Clin Rad. 2002.
Ajmal M, O’Rourke SK. Odontoid Lateral Mass Interval (OLMI) asymmetry and rotary subluxation: a retrospective study in cervical spine injury. J Surg Orthop Adv. 2005;14(1):23–6.
Deliganis AV, Baxter AB, Hanson JA, et al. Radiologic spectrum of craniocervical distraction injuries. Radiographics. 2000;20(Spec No):S237–250.
Monckeberg JE, Tome CV, Matias A, Alonso A, Vasquez J, Zubieta JL. CT scan study of atlantoaxial rotatory mobility in asymptomatic adult subjects: a basis for better understanding C1–C2 rotatory fixation and subluxation. Spine (Phila Pa 1976). 2009;34:1292–295.
Mirvis SE. How much lateral atlantodental interval asymmetry and atlantoaxial lateral mass asymmetry is acceptable on an open-mouth odontoid radiograph, and when is additional investigation necessary? AJR Am J Roentgenol. 1998;170:1106–7.
Meza Escobar LE, Osterhoff G, Ossendorf C, Wanner GA, Simmen HP, Werner CM. Traumatic atlantoaxial rotatory subluxation in an adolescent: a case report. J Med Case Rep. 2012;6:27.
Willauschus WG, Kladny B, Beyer WF, Gluckert K, Arnold H, Scheithauer R. Lesions of the alar ligaments. In vivo and in vitro studies with magnetic resonance imaging. Spine (Phila Pa 1976). 1995;20:2493–498.
German JW, Hart BL, Benzel EC. Nonoperative management of vertical C2 body fractures. Neurosurgery. 2005;56:516–21 (discussion 516–21).
Greene KA, Dickman CA, Marciano FF, Drabier JB, Hadley MN, Sonntag VK. Acute axis fractures. Analysis of management and outcome in 340 consecutive cases. Spine (Phila Pa 1976). 1997;22:1843–852.
Burke JT, Harris JH Jr. Acute injuries of the axis vertebra. Skeletal Radiol. 1989;18(5):335–46.
Sherk HH, Nicholson JT. Fractures of the atlas. J Bone Joint Surg Am. 1970;52:1017–24.
Hinck VC, Hopkins CE. Measurement of the atlanto-dental interval in the adult. Am J Roentgenol Radium Ther Nucl Med. 1960;84:945–51.
Jackson H. The diagnosis of minimal atlanto-axial subluxation. Br J Radiol. 1950;23:672–4.
Levine AM, Edwards CC. Traumatic lesions of the occipitoatlantoaxial complex. Clin Orthop Relat Res. 1989:53–68.
Hudek RWG, Wanner G, Simmen HP, Werner CML. C1 fracture in a patient with a congenital cleft in the posterior arch: report on a failed conservative treatment. BMJ Case Rep. 2013;2013:13.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr. Sebastian Guenkel, Dr. Max Joseph Scheyerer, PD. Dr. Georg Osterhoff, Prof. Dr. Guido A Wanner, Prof. Dr. Hans-Peter Simmen, and Prof. Dr. Clement ML Werner declare that they have no conflict of interest.
Ethical standards
By compliance with ethical requirements, the approval was waived by the institutional ethical committee.
Rights and permissions
About this article

Cite this article
Guenkel, S., Scheyerer, M.J., Osterhoff, G. et al. It is the lateral head tilt, not head rotation, causing an asymmetry of the odontoid-lateral mass interspace. Eur J Trauma Emerg Surg 42, 749–754 (2016). https://doi.org/10.1007/s00068-015-0602-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-015-0602-0