
Abstract
Purpose
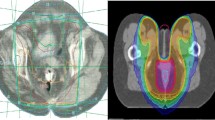
Radiochemotherapy is the standard treatment for anal carcinoma (ACa). Intensity-modulated radiotherapy (IMRT) has been introduced, allowing focused irradiation of the tumor area. Whether physical benefits of IMRT translate to clinical benefits has not been sufficiently demonstrated.
Methods
We retrospectively reviewed data from 82 patients with newly diagnosed ACa. Patients treated with IMRT were compared with previous patients treated with conventional three-dimensional computational radiotherapy (3D-CRT). The influence of IMRT on complete remission and acute and chronic side effects was analyzed in univariate and multivariate analyses.
Results
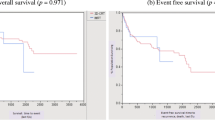
39/40 patients treated with IMRT were in complete remission after 1 year compared to 31/39 patients treated with 3D-CRT (p = 0.014). Multivariate analysis confirmed tumor T stage as well as lack of IMRT treatment as risk factors for persistent tumor at 6 months. No significant benefits of IMRT were apparent at later timepoints (median follow up 52 months, IQR: 31.5–71.8 months). Patients treated with IMRT had a significantly lower degree of skin toxicity (median 2 vs. 3 in a scale ranging from 0 to 3, p = 0.00092). Rates of hematological toxicity/proctitis were not reduced and rates of acute diarrhea increased (p = 0.034). Median length of hospitalization tended to be shorter in patients treated with IMRT (n. s.).
Conclusion
We present a real-world experience of shifting radiation technique from conventional 3D-CRT to IMRT. IMRT patients had better tumor control at 1 year and lower degrees of skin toxicity. Our data indicate that IMRT can enable therapies with lower side effects with equal or better oncological results for patients with ACa.
Zusammenfassung
Hintergrund
Die definitive Radiochemotherapie stellt den Goldstandard für die Therapie des Analkarzinoms (ACa) dar. Die in den letzten Jahren eingeführte intensitätsmodulierte Strahlentherapie (IMRT) erlaubt eine fokussierte Bestrahlung des Tumorgebiets unter Schonung der umliegenden Strukturen. Ob diese Vorteile auch einen klinischen Benefit bringen, wurde bis jetzt nur ungenügend untersucht.
Methodik
Es erfolgte eine retrospektive Analyse von 82 Patienten mit der Neudiagnose eines ACa, mit einem Vergleich zwischen Patienten, die mit IMRT versus mit der traditionell durchgeführten 3D-konformalen Radiotherapie (3D-CRT) behandelt wurden. Es wurde der Einfluss der IMRT auf das Erreichen einer klinischen Remission sowie auf Rezidivrate und Nebenwirkungen untersucht.
Ergebnisse
Die Remissionsrate 1 Jahr nach Ende der Bestrahlung der Patienten lag in der IMRT-Gruppe bei 97,5 % (39/40) vs. 79,5 % (31/39) in der 3D-CRT-Gruppe (p = 0,014). Die multivariate Analyse bestätigte das T‑Stadium als auch die 3D-CRT-Therapie als Risikofaktor für Tumorpersistenz nach 6 Monaten. Weitere Effekte der IMRT-Therapie bei späteren Zeitpunkten wurden nicht beobachtet (medianer Follow-up 52 Monate; IQR 31,5–71,8 Monate). Patienten unter IMRT hatten signifikant weniger schwere Hauttoxizität (median 2 vs. 3 in einer Skala von 0–3; p = 0,00092). Hämatologische Toxizität/Proktitis waren vergleichbar, akute Diarrhoe trat bei IMRT-Patienten häufiger auf (p = 0,034). Die mediane Hospitalisierungsdauer war bei IMRT-Patienten tendenziell verkürzt (ohne statistische Signifikanz).
Schlussfolgerung
Wir präsentieren „Real-world“-Daten des Übergangs der RT von der 3D-CRT- zur IMRT-Technik. Die IMRT-Patienten hatten eine höhere Remissionsrate nach 6 Monaten und eine niedrigere Rate für Hauttoxizitäten. Die IMRT-Therapie führt beim ACa zu insgesamt weniger Nebenwirkungen bei mindestens gleichwertigem oder sogar besserem onkologischem Outcome.

Similar content being viewed by others

Abbreviations
- 3D-CRT:
-
Three-dimensional computational radiotherapy
- 5‑FU:
-
5‑Fluorouracil
- ACa:
-
Anal carcinoma
- CI:
-
Confidence interval
- CR:
-
Complete response
- CT:
-
Computed tomography
- CTCAE:
-
National Cancer Institute Common Terminology Criteria for Adverse Events
- HIV:
-
Human immunodeficiency virus
- HPV:
-
Human papillomavirus
- IMRT:
-
Intensity-modulated radiotherapy
- MMC:
-
Mitomycin
- MRI:
-
Magnetic resonance imaging
- OR:
-
Odds ratio
- RTOG:
-
Radiation Therapy Oncology Group
- SIB:
-
Simultaneous integrated boost
References
Johnson LG, Madeleine MM, Newcomer LM, Schwartz SM, Daling JR (2004) Anal cancer incidence and survival: the surveillance, epidemiology, and end results experience, 1973–2000. Cancer 101(2):281–288
Glynne-Jones R, Nilsson PJ, Aschele C, Goh V, Peiffert D, Cervantes A, Arnold D (2014) Anal cancer: ESMO-ESSO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 25(Suppl 3):iii10–iii20
Nigro ND, Vaitkevicius VK, Considine B Jr. (1974) Combined therapy for cancer of the anal canal: a preliminary report. Dis Colon Rectum 17(3):354–356
Bartelink H, Roelofsen F, Eschwege F, Rougier P, Bosset JF, Gonzalez DG, Peiffert D, van Glabbeke M, Pierart M (1997) Concomitant radiotherapy and chemotherapy is superior to radiotherapy alone in the treatment of locally advanced anal cancer: results of a phase III randomized trial of the European Organization for Research and Treatment of Cancer Radiotherapy and Gastrointestinal Cooperative Groups. J Clin Oncol 15(5):2040–2049
UKCCCR Anal Cancer Trial Working Party, UK Co-ordinating Committee on Cancer Research (1996) Epidermoid anal cancer: results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5‑fluorouracil, and mitomycin. Lancet 348(9034):1049–1054
Leichman L, Nigro N, Vaitkevicius VK, Considine B, Buroker T, Bradley G, Seydel HG, Olchowski S, Cummings G, Leichman C (1985) Cancer of the anal canal. Model for preoperative adjuvant combined modality therapy. Am J Med 78(2):211–215
Flam M, John M, Pajak TF, Petrelli N, Myerson R, Doggett S, Quivey J, Rotman M, Kerman H, Coia L et al (1996) Role of mitomycin in combination with fluorouracil and radiotherapy, and of salvage chemoradiation in the definitive nonsurgical treatment of epidermoid carcinoma of the anal canal: results of a phase III randomized intergroup study. J Clin Oncol 14(9):2527–2539
Gunderson LL, Winter KA, Ajani JA, Pedersen JE, Moughan J, Benson AB, Thomas CR, Mayer RJ, Haddock MG, Rich TA et al (2012) Long-term update of US GI intergroup RTOG 98-11 phase III trial for anal carcinoma: survival, relapse, and colostomy failure with concurrent chemoradiation involving fluorouracil/mitomycin versus fluorouracil/cisplatin. J Clin Oncol 30(35):4344–4351
Mayer RJ, Venook AP, Schilsky RL (2014) Progress against GI cancer during the American Society of Clinical Oncology’s first 50 years. J Clin Oncol 32(15):1521–1530
Vuong T, Kopek N, Ducruet T, Portelance L, Faria S, Bahoric B, Devic S (2007) Conformal therapy improves the therapeutic index of patients with anal canal cancer treated with combined chemotherapy and external beam radiotherapy. Int J Radiat Oncol Biol Phys 67(5):1394–1400
Morris DE, Emami B, Mauch PM, Konski AA, Tao ML, Ng AK, Klein EA, Mohideen N, Hurwitz MD, Fraas BA et al (2005) Evidence-based review of three-dimensional conformal radiotherapy for localized prostate cancer: an ASTRO outcomes initiative. Int J Radiat Oncol Biol Phys 62(1):3–19
Eisbruch A, Ship JA, Dawson LA, Kim HM, Bradford CR, Terrell JE, Chepeha DB, Teknos TN, Hogikyan ND, Anzai Y et al (2003) Salivary gland sparing and improved target irradiation by conformal and intensity modulated irradiation of head and neck cancer. World J Surg 27(7):832–837
Zelefsky MJ, Fuks Z, Leibel SA (2002) Intensity-modulated radiation therapy for prostate cancer. Semin Radiat Oncol 12(3):229–237
Mell LK, Roeske JC, Mundt AJ (2003) A survey of intensity-modulated radiation therapy use in the United States. Cancer 98(1):204–211
Milano MT, Jani AB, Farrey KJ, Rash C, Heimann R, Chmura SJ (2005) Intensity-modulated radiation therapy (IMRT) in the treatment of anal cancer: toxicity and clinical outcome. Int J Radiat Oncol Biol Phys 63(2):354–361
Kachnic LA, Tsai HK, Coen JJ, Blaszkowsky LS, Hartshorn K, Kwak EL, Willins JD, Ryan DP, Hong TS (2012) Dose-painted intensity-modulated radiation therapy for anal cancer: a multi-institutional report of acute toxicity and response to therapy. Int J Radiat Oncol Biol Phys 82(1):153–158
Kachnic LA, Winter K, Myerson RJ, Goodyear MD, Willins J, Esthappan J, Haddock MG, Rotman M, Parikh PJ, Safran H et al (2013) RTOG 0529: a phase 2 evaluation of dose-painted intensity modulated radiation therapy in combination with 5‑fluorouracil and mitomycin‑C for the reduction of acute morbidity in carcinoma of the anal canal. Int J Radiat Oncol Biol Phys 86(1):27–33
Vinayan A, Glynne-Jones R (2016) Anal cancer—what is the optimum chemoradiotherapy? Best Pract Res Clin Gastroenterol 30(4):641–653
Sauter M, Vavricka SR, Keilholz G, Heinrich H, Winder T, Kranzbuhler H, Lombriser N, Misselwitz B (2017) Surveillance of anal carcinoma after radiochemotherapy : a retrospective analysis of 80 patients. Strahlenther Onkol 193(8):639–647
Sauter M, Keilholz G, Kranzbuhler H, Lombriser N, Prakash M, Vavricka SR, Misselwitz B (2016) Presenting symptoms predict local staging of anal cancer: a retrospective analysis of 86 patients. BMC Gastroenterol 16:46
Edge SBBD, Compton CC (eds) (2010) AJCC cancer staging handbook, 7th edn. Springer, New York
Common Terminology Criteria for Adverse Events v4.0 (CTCAE). https://www.eortc.be/services/doc/ctc/ctcae_4.03_2010-06-14_quickreference_5x7.pdf. Accessed: 29 January 2018
Bazan JG, Hara W, Hsu A, Kunz PA, Ford J, Fisher GA, Welton ML, Shelton A, Kapp DS, Koong AC et al (2011) Intensity-modulated radiation therapy versus conventional radiation therapy for squamous cell carcinoma of the anal canal. Cancer 117(15):3342–3351
Chuong MD, Freilich JM, Hoffe SE, Fulp W, Weber JM, Almhanna K, Dinwoodie W, Rao N, Meredith KL, Shridhar R (2013) Intensity-modulated radiation therapy vs. 3D conformal radiation therapy for squamous cell carcinoma of the anal canal. Gastrointest Cancer Res 6(2):39–45
Dasgupta T, Rothenstein D, Chou JF, Zhang Z, Wright JL, Saltz LB, Temple LK, Paty PB, Weiser MR, Guillem JG et al (2013) Intensity-modulated radiotherapy vs. conventional radiotherapy in the treatment of anal squamous cell carcinoma: a propensity score analysis. Radiother Oncol 107(2):189–194
Dewas CV, Maingon P, Dalban C, Petitfils A, Peignaux K, Truc G, Martin E, Khoury C, Dewas S, Crehange G (2012) Does gap-free intensity modulated chemoradiation therapy provide a greater clinical benefit than 3D conformal chemoradiation in patients with anal cancer? Radiat Oncol 7:201
Fredman ET, Abdel-Wahab M, Kumar AMS (2017) Influence of radiation treatment technique on outcome and toxicity in anal cancer. J Radiat Oncol 6(4):413–421
Koerber SA, Slynko A, Haefner MF, Krug D, Schoneweg C, Kessel K, Kopp-Schneider A, Herfarth K, Debus J, Sterzing F (2014) Efficacy and toxicity of chemoradiation in patients with anal cancer—a retrospective analysis. Radiat Oncol 9:113
Muirhead R, Drinkwater K, O’Cathail SM, Adams R, Glynne-Jones R, Harrison M, Hawkins MA, Sebag-Montefiore D, Gilbert DC (2017) Initial results from the Royal College of Radiologists’ UK national audit of anal cancer radiotherapy 2015. Clin Oncol (R Coll Radiol) 29(3):188–197
Pollom EL, Wang G, Harris JP, Koong AC, Bendavid E, Bhattacharya J, Chang DT (2017) The impact of intensity modulated radiation therapy on hospitalization outcomes in the SEER-medicare population with anal squamous cell carcinoma. Int J Radiat Oncol Biol Phys 98(1):177–185
Kemmerer EMA, Ranganna S, Price R, Komarnicky L, Poli J (2016) (P044) Comparison of toxicity-related breaks in treatment utilizing intensity-modulated radiation therapy (IMRT) vs three-dimensional (3D) Conformal techniques in the treatment of anal cancer. Oncology 30(Suppl 1). https://www.cancernetwork.com/ars-2016/p044-comparison-toxicity-related-breaks-treatment-utilizing-intensity-modulated-radiation-therapy
Cendales R, Vasquez J, Arbelaez J, Bobadilla I, Torres F, Gaitan A (2014) IMRT, RapidArc(R) and conformal radiotherapy in the treatment of tumours of the anal canal. Ecancermedicalscience 8:469
Chang Y, Yang ZY, Li GL, Li Q, Yang Q, Fan JQ, Zhao YC, Song YQ, Wu G (2016) Correlations between radiation dose in Bone marrow and hematological toxicity in patients with cervical cancer: a comparison of 3DCRT, IMRT, and rapidARC. Int J Gynecol Cancer 26(4):770–776
Kumar T, Schernberg A, Busato F, Laurans M, Fumagalli I, Dumas I, Deutsch E, Haie-Meder C, Chargari C (2019) Correlation between pelvic bone marrow radiation dose and acute hematological toxicity in cervical cancer patients treated with concurrent chemoradiation. Cancer Manag Res 11:6285–6297
Elson JK, Kachnic LA, Kharofa JR (2018) Intensity-modulated radiotherapy improves survival and reduces treatment time in squamous cell carcinoma of the anus: a national cancer data base study. Cancer 124(22):4383–4392
Peiffert D, Tournier-Rangeard L, Gerard JP, Lemanski C, Francois E, Giovannini M, Cvitkovic F, Mirabel X, Bouche O, Luporsi E et al (2012) Induction chemotherapy and dose intensification of the radiation boost in locally advanced anal canal carcinoma: final analysis of the randomized UNICANCER ACCORD 03 trial. J Clin Oncol 30(16):1941–1948
Ferris RL, Blumenschein G Jr., Fayette J, Guigay J, Colevas AD, Licitra L, Harrington K, Kasper S, Vokes EE, Even C et al (2016) Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med 375(19):1856–1867
Hamid O, Robert C, Daud A, Hodi FS, Hwu WJ, Kefford R, Wolchok JD, Hersey P, Joseph RW, Weber JS et al (2013) Safety and tumor responses with lambrolizumab (anti-PD-1) in melanoma. N Engl J Med 369(2):134–144
Morris VK, Salem ME, Nimeiri H, Iqbal S, Singh P, Ciombor K, Polite B, Deming D, Chan E, Wade JL et al (2017) Nivolumab for previously treated unresectable metastatic anal cancer (NCI9673): a multicentre, single-arm, phase 2 study. Lancet Oncol 18(4):446–453
Martin D, Rodel C, Fokas E (2018) Nivolumab for pretreated metastatic anal cancer : immune checkpoint blockade is also advised in combination with radiochemotherapy. Strahlenther Onkol 194(4):356–357
Martin D, Rodel C, Fokas E (2019) Chemoradiotherapy for anal cancer: are we as good as we think? Strahlenther Onkol 195(5):369–373
Leon O, Guren MG, Radu C, Gunnlaugsson A, Johnsson A (2015) Phase I study of cetuximab in combination with 5‑fluorouracil, mitomycin C and radiotherapy in patients with locally advanced anal cancer. Eur J Cancer 51(18):2740–2746
Garg MK, Zhao F, Sparano JA, Palefsky J, Whittington R, Mitchell EP, Mulcahy MF, Armstrong KI, Nabbout NH, Kalnicki S et al (2017) Cetuximab plus Chemoradiotherapy in immunocompetent patients with anal carcinoma: a Phase II Eastern Cooperative Oncology Group-American College of Radiology Imaging Network Cancer Research Group Trial (E3205). J Clin Oncol 35(7):718–726
Kouloulias V, Plataniotis G, Kouvaris J, Dardoufas C, Gennatas C, Uzunoglu N, Papavasiliou C, Vlahos L (2005) Chemoradiotherapy combined with intracavitary hyperthermia for anal cancer: feasibility and long-term results from a phase II randomized trial. Am J Clin Oncol 28(1):91–99
Ott OJ, Schmidt M, Semrau S, Strnad V, Matzel KE, Schneider I, Raptis D, Uter W, Grutzmann R, Fietkau R (2019) Chemoradiotherapy with and without deep regional hyperthermia for squamous cell carcinoma of the anus. Strahlenther Onkol. https://doi.org/10.1007/s00066-018-1396-x
Ajani JA, Winter KA, Gunderson LL, Pedersen J, Benson AB 3rd, Thomas CR Jr., Mayer RJ, Haddock MG, Rich TA, Willett C (2008) Fluorouracil, mitomycin, and radiotherapy vs fluorouracil, cisplatin, and radiotherapy for carcinoma of the anal canal: a randomized controlled trial. JAMA 299(16):1914–1921
Acknowledgements
The authors would like to thank Brian Lang, Department of Biosystems Science and Engineering, ETH Basel, for help with the statistics.
Author information
Authors and Affiliations
Contributions
MSa, BM, SV, NL: study design. MSa, SB, GK, BM: data acquisition. MSa, SB, NL, SV, HH, BM, MSa, FB: data analysis. MSa, SB, GK, NL, BM: drafting of manuscript. All authors reviewed and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
M. Sauter, N. Lombriser, S. Bütikofer, G. Keilholz, H. Kranzbühler, H. Heinrich, G. Rogler, S.R. Vavricka, and B. Misselwitz declare that they have no competing interests.
Caption Electronic Supplementary Material
66_2019_1534_MOESM1_ESM.pdf
Supplementary Figure S1: Rates of complete response at 6 months and at end of study. Statistical analysis: Fisher’s exact test. IMRT: intensity modulated radiotherapy, 3D-CRT: three-dimensional computational radiotherapy
66_2019_1534_MOESM2_ESM.pdf
Supplementary Figure S2: Acute side effects of treatment and length of hospitalization. Statistical analysis: Fisher’s exact test, Mann-Whitney‑U test. IMRT: intensity modulated radiotherapy, 3D-CRT: three-dimensional computational radiotherapy
66_2019_1534_MOESM3_ESM.pdf
Supplementary Figure S3: Chronic side effects of treatment. Statistical analysis: Fisher’s exact test. IMRT: intensity modulated radiotherapy, 3D-CRT: three-dimensional computational radiotherapy
Rights and permissions
About this article

Cite this article
Sauter, M., Lombriser, N., Bütikofer, S. et al. Improved treatment outcome and lower skin toxicity with intensity-modulated radiotherapy vs. 3D conventional radiotherapy in anal cancer. Strahlenther Onkol 196, 356–367 (2020). https://doi.org/10.1007/s00066-019-01534-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-019-01534-6