
Abstract
Background
Osteoporotic fractures are common, and their incidence are increasing worldwide. The first fracture doubles the risk of new fractures. Despite that, up to 80% of patients with a fragility fracture are evaluated or treated to reduce the risk of new fractures.
Aims
To evaluate the results of the operation of the hospital Fracture Liaison Service (FLS) and to analyze the clinical characteristics of the patients attending the service in its first 2 years of operation and to estimate the fracture risk reduction ratio.
Methods
The FLS managed patients older than 50 years who were admitted with a low-energy trauma fracture between January 2017 and April 2018. This management consists in a full medical evaluation, nutritional and physical activity guidance, and specific osteoporosis treatment, if needed.
Results
We monitored and treated 135 patients. Forty percent of them had a previous fracture and only 20.3% of them received treatment to prevent new fractures. On Kaplan–Meier analysis, the estimated incidence of new fractures over 24 months was 12.1% (95% CI 7.2–20.8%), indicating that the percentage of patients without new fractures due to bone fragility during treatment was estimated at 87.9% (95% CI 79.2–92.8%).
Conclusions
The evaluation and treatment of patients who sustained a fragility fracture to prevent a secondary fracture is effective in reducing the risk of new fractures in high-risk patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is a prevalent disease characterized by reduced bone mass and deteriorated bone microarchitecture [1], predisposing the individual to an increased risk of fracture. Osteoporotic fractures occur due to decreased bone strength and are usually associated with low-energy trauma [2]. One osteoporotic fracture is estimated to occur at each 3 s worldwide [3,4,5]. According to data published in 2017 by the International Osteoporosis Foundation (IOF) [6], the number of hip fractures in Brazil is estimated to increase from 80,640 cases in 2015 to 198,000 cases in 2040, representing approximately one hip fracture every 2.6 min [7]. A survey carried out in 2014 by the Ministry of Health and the Unified Health System (SUS) in Brazil identified 3.2 million procedures for fractures due to bone fragility performed between 2008 and 2010, representing an estimated staggering cost of R$ 289 million [8]. In addition, a study published by the Mayo Clinic has shown that hospital and non-hospital costs for the treatment of osteoporotic fractures outweigh the combined costs for the treatment of acute myocardial infarction, stroke, or breast cancer [9].
About half of future hip fractures will occur in individuals who have already experienced a fracture due to bone fragility, i.e., approximately 15% of the population [10,11,12,13,14,15]. The occurrence of a first fracture due to osteoporosis doubles the risk of a new fracture and increases up to four times the risk of a new fracture when the first fracture affects the vertebrae [16, 17]. The subsequent fracture usually occurs within the first few years after the first fracture, on average 6–8 months after that [18]. Despite that, the literature indicates that many patients do not receive treatment for osteoporosis after the first fracture. Indeed, up to 80% of the patients with fractures due to bone fragility are not evaluated or treated for osteoporosis or advised on the prevention of falls to reduce the incidence of new fractures [19]. This means that many fractures that occur today could have been prevented [19]. Some studies also show that the number of patients who are evaluated and treated after a fracture due to bone fragility has been decreasing over the years [20, 21].
Early management of patients after a fracture due to bone fragility can reduce by 30 to 60% the incidence of new fractures in this group [22]. For the same reduction in the incidence of fractures through primary prevention, five to six times more patients must be identified and evaluated [11, 23]. In an attempt to reduce gaps in care pointed out by studies in osteoporosis, the IOF has launched the Capture the Fracture program, a global initiative aimed at reducing subsequent fractures by creating standards for the implementation of Fracture Liaison Services (FLSs). These services, centralized around a coordinator, identify patients with fractures and implement treatment to prevent subsequent fractures. Additionally, FLSs direct the patient to undergo evaluation with bone densitometry and implement educational measures in osteoporosis. This program uses a systematic approach to osteoporosis, which improves the quality of care for patients who have experienced a fracture caused by bone fragility. All these measures provide a significant reduction in costs [11]. To date, the IOF Capture the Fracture program has over 600 registered FLSs across 48 countries. In Brazil, there are 44 installed and registered services with FLS characteristics. One such service is the Service for Prevention of Osteoporotic Fracture of the Hospital da Cruz Vermelha Brasileira no Paraná, located in Curitiba; this is the first service in the state of Paraná to be mapped by the program. This service has received a “gold” classification in the criteria of good practices recommended by the program. The primary objective of the present study was to evaluate the results of the operation of this secondary fracture prevention service. A secondary objective of the study was to analyze the clinical characteristics of the patients attending the service in its first 2 years of operation.
Methods
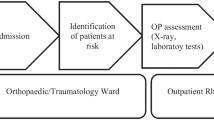
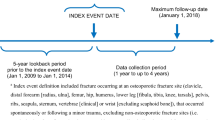
All patients older than 50 years admitted after April 2018 to the emergency unit of the Hospital da Cruz Vermelha Brasileira no Paraná (Curitiba, Paraná) with a diagnosis of fracture caused by low-energy trauma and undergoing conservative or surgical treatment were identified by the local FLS. The search included fractures affecting the vertebrae, proximal femur, proximal humerus, distal radius, ankle, elbow, and patella. A retrospective survey was also carried out through analysis of medical records of patients older than 50 years who underwent surgical treatment for fractures at the hospital between January 2017 and April 2018 for identification of cases with fractures caused by low-energy trauma. We excluded from the study those patients with fractures caused by high-energy trauma or metastatic diseases, periprosthetic fractures, atypical fractures, and age below 50 years.
The identified patients were invited to follow-up at the FLS through a telephone call from the nursing staff and were referred for medical consultation with an orthopedic surgeon specialized in osteoporosis. During the appointment, we investigated the patients’ risk factors for bone fragility, including the presence of comorbidities, use of medications that interfere with bone metabolism, sedentary lifestyle, lifestyle habits, and family history of osteoporosis and fractures, among others. The complementary tests requested in the baseline evaluation included complete blood count, measurement of fasting blood glucose and serum calcium, ionized calcium, vitamin D (25-hydroxyvitamin D), parathyroid hormone (PTH), alkaline phosphatase, creatinine, phosphorus, magnesium, TSH, free thyroxine (T4), and glycated hemoglobin levels, urinalysis, creatinine clearance, 24-h urinary calcium, protein electrophoresis, bone densitometry, and dorsal and lumbar spine X-rays. We also calculated the patients’ Fracture Risk Assessment Tool (FRAX) score to estimate their risk of major fractures and hip fractures in 10 years [7].
After having the results of the complementary tests analyzed, the patients received dietary guidance on the consumption of foods with calcium, sun exposure, and physical activity. Prescriptions of calcium and vitamin D supplementation and medications for the treatment of osteoporosis were individualized for each patient. The patients then followed up with medical appointments at individualized intervals tailored to their needs and characteristics, at intervals ranging from quarterly to annually. At least once yearly, the patients were evaluated with measurement of serum calcium, vitamin D, and PTH levels, renal function tests, dorsal and lumbar spine X-rays, and bone densitometry. The patients were also monitored for the occurrence of new fractures, diagnosis of new comorbidities, and adherence to the use of the prescribed medications. Adherence was assessed by questioning the patients about the use of medications and was considered “good” when they reported using the prescribed doses, “regular” when they reported skipping or forgetting some doses but continuing treatment, and “poor” when they abandoned treatment.
All patients agreed to participate in the study and signed an informed consent form. The study project was approved by the Research Ethics Committee of Universidade Positivo with the number 13433819.9.0000.0093.
Statistical analysis
The sample size was calculated to estimate the percentage of patients free from a new fracture in 24 months. Considering this estimate to be 90%, a sample of 137 patients was deemed sufficient with a margin of error of 5% and a confidence level of 95%.
The data were analyzed using the Stata/SE program, version 14.1 (StataCorp LP, College Station, TX, USA). Quantitative variables were described as mean, standard deviation, median, and minimum and maximum values, while categorical variables were described as frequencies and percentages. Cox regression models were adjusted for quantitative variables while the log-rank test was used for categorical variables to analyze the variables associated with the time from treatment start to the occurrence of a new fracture (fracture during ongoing treatment). The effect size was expressed by hazard ratios and 95% confidence intervals. P values < 0.05 indicated statistical significance.
Results
From January 1st, 2017, to August 31st, 2020, we identified 522 patients older than 50 years and diagnosed with fragility fracture who met the study inclusion criteria. After initial contact, 251 patients underwent a first medical assessment at the FLS, and 135 continued to be monitored and treated, comprising the study cohort. One hundred and sixteen patients did not complete the follow-up for not returning to medical consultation to complementary exams analysis, not to start proposed treatment or for having refused to return for evaluation. Table 1 shows the main characteristics available of the total group (522), and compared patients included or not in the study. Patients not included had a greater percentage of deaths, more hip, and less spine fractures. Table 2 shows clinical and demographic characteristics of the 135 patients included in the study. One 48-year-old patient were included in the study because she presented with an ankle fracture caused by a low-energy sprain, densitometric osteoporosis and other risk factors for bone fragility.
In the study cohort, 123 patients were women (91.1%) and 12 were men (8.9%). The mean age at the time of the fracture was 71.7 ± 11.6 years. The mean follow-up was 16.0 ± 9.4 months, during which 78.5% of the patients had at least three medical appointments. Regarding the anatomical distribution of the fractures, 17.8% occurred in the hip, 28.1% in vertebrae, 25.2% in the distal portion of the radius, 10.4% in the proximal portion of the humerus, 7.4% in the ankle, and 11.1% elsewhere. The treatment of the fractures was surgical in 65 (48.1%) patients and conservative in 70 (51.9%) of them. There were 6 (4.4%) deaths in the treatment group, with a mean time from the initiation of osteoporosis treatment to death of 10.2 ± 4.3 months. Of the 135 patients, 54 (40%) had at least one fragility fracture before the sentinel fracture that led to their identification by the FLS, and among these, only 11 (20.4%) received treatment for osteoporosis after the previous fracture. We found 48 patients (35.8%) with incidental and asymptomatic vertebral fractures on lumbar and dorsal spine X-rays requested at baseline or during follow-up.
Table 3 shows the frequency of associated comorbidities presented by the study patients. The mean risk of new fractures according to the FRAX algorithm at baseline was 5.6 ± 8.3% for hip fractures and 12.2 ± 9.3% for major fractures.
In all, 34.8% of the patients were treated with oral bisphosphonates, 54.1% with denosumab, and 5.9% with intravenous zoledronic acid. In 5.2% of the patients, only supplementation with calcium and vitamin D was prescribed due to the low risk of fractures and absence of other risk factors besides the occurrence of a previous fracture. The medication and supplementation choice, when indicated, were made together with patient and family, considering the osteoporosis severity, estimated risk fracture with the FRAX algorithm, clinical contraindications, dosage comfort, financial conditions, and patients’ preferences. Patient adherence to treatment was considered good in 80.7% of the cases, regular in 8.1%, and poor in 11.1% of them. Table 3 shows the results of the baseline laboratory tests and bone densitometry results, Tables 4 and 5 show the clinical outcomes of the study patients.
Among the 135 patients followed up for a median of 13 months (2 to 24 months), 15 (11.1%) presented new fractures due to bone fragility while receiving treatment. On Kaplan–Meier analysis, the estimated incidence of new fractures over 24 months was 12.1% (95% CI 7.2–20.8%), indicating that the percentage of patients without new fractures due to bone fragility during treatment was estimated at 87.9% (95% CI 79.2–92.8%). The incidence rate of new fractures was 9 per 100 patient-years (Fig. 1).

Curve of cumulative incidence of new fractures. On Kaplan–Meier analysis, after 24 month of follow-up, 87.9% of patients were free of new fractures, as the incidence was 12.1%
No significant difference was observed in terms of FRAX-calculated risk between patients who experienced new fractures (hip fractures 6.5 ± 6.1 and major fractures 14.1 ± 7.7, HR 1.01, 95% CI 0.95–1.07, p = 0.680) and those who did not experience new fractures (hip fractures 5.5 ± 8.5 and larger fractures 12 ± 9.5, HR 1.02, 95% CI 0.97–1.07, p = 0.476). Fifteen patients were diagnosed with new fragility fractures in the follow-up period. The new fractures involved vertebrae in eight patients, hip in two patients, distal radius in two patients, proximal humerus in two patients, and the pubic bone in one patient. Of these, 13 were woman (86.7%) and 2 man (13.3%) and the mean age at the time of the sentinel fracture were 71 years old (53–97 y.o.). Two patients died after the new fracture. The new fracture happened, in average, after 10.4 months of the beginning of the treatment, and 12 patients (80%) were using denosumab and 3 patients (20%) risedronate. The adherence was considered as good in 14 patients (93.3%) and regular in 1 patient (6.7%). This one patient delayed her denosumab dose in 3 months and had a vertebral fracture diagnosed in this interval. Nine out of 15 patients (60%) were diagnosed with an incidental vertebral fracture in the FLS initial evaluation and 6 of them (40%) had at least one other previous fragility fracture before the sentinel fracture. Only 2 of these patients received treatment to prevent new fractures before the inclusion in the FLS.
Discussion
The results of the present study confirm previous observations that (1) a fracture due to bone fragility represents a risk for new fractures, (2) few patients receive treatment to prevent new fractures after an osteoporotic fracture and (3) FLSs are effective in reducing the risk of fractures in patients with a history of fracture due to bone fragility. Altogether, 40% of the patients included in the study had fractures due to bone fragility before the fracture that led to their identification by the FLS, and only 20.4% of these patients received treatment for secondary prevention of fractures. Our sample have a high rate of woman of 87.7% in the total group of identified patients and 91.1% in the study group. The possible explanation for these is that women live longer than men, having more time to develop a fragility fracture, and that osteoporosis is a disease that affects women much more than men.
In general, more than 80% of the patients who experience a fracture due to bone fragility are not evaluated or treated with the intention of preventing new fractures [19]. A retrospective study including more than 6000 patients who experienced vertebral fracture between 2008 and 2015 has shown that only 28.8% of them received treatment for osteoporosis in the first year after the fracture and that this number dropped from 30% in 2008 to 24% in 2015 [20]. Another study in patients who experienced a hip fracture between 2002 and 2011 has shown that the use of medications for osteoporosis treatment decreased from 40% in 2002 to 21% in 2011 [21]. Similarly, 40% of our cohort of 135 patients had fragility fractures before the sentinel event that led to their identification by the FLS, and only 20.3% of them had received treatment for osteoporosis to reduce the risk of new fractures.
A recent systematic review and meta-analysis of 74 studies has reported that FLSs have resulted in a 24% increase in the number of patients undergoing bone densitometry [24]. This increase is still considered insufficient, considering that less than 50% of the patients involved in these studies underwent this evaluation. During our study, all the patients underwent at least one evaluation with bone densitometry, allowing for easier monitoring and better diagnosis and follow-up of the patients’ osteoporosis. All our patients also underwent radiographic examination of the dorsal and lumbar spine, improving substantially the diagnosis of prevalent vertebral fractures, which can be asymptomatic and difficult to identify. In the same review mentioned above, the authors also reported that patients treated in FLSs had a 20% higher rate of osteoporosis treatment initiation compared with those who were not treated in a FLS and that the FLSs increased the adherence rate by 22%, whereas uncontrolled studies have reported a mean adherence rate of 75%. The adherence of the patients involved in our study was considered good in 80.7% of the cases, regular in 8.1%, and poor in 11.1% of them, which is aligned with rates reported in the literature. The FLS’s also have the goal to increase the access to bone densitometry to the patients who sustain a fragility fracture as well as raise the screening and diagnosis of secondary causes of bone fragility. All patients followed by this study have done at least on bone densitometry and the laboratorial screening for secondary causes of bone fragility. Another important role of the FLS is to search the diagnosis of prevalent vertebral fractures. We know that up to 70% of the osteoporotic vertebral fractures are asymptomatic and that the risk of a new vertebral fracture in the first year after the first fracture can be as high as 7 times bigger [25]. All FLS patients made at least one dorsal and lumbar spine x-ray and we identified 48 (35.8%) patients with incidental and asymptomatic vertebral fractures.
The implementation of a systematic approach for the identification, assessment, and treatment of patients presenting with fractures due to bone fragility has been shown to be effective in reducing the incidence of new fractures. In general, FLSs are associated with a lower risk of new fragility fracture, with a 30 to 60% reduction in the incidence of new fractures [22, 26, 27]. The first service operating according to the guidelines of the Capture the Fracture program in Brazil was the PrevRefrat, at the Hospital de Ipanema in Rio de Janeiro. Based on data provided by a health care provider, the service in 2016 had a 50% reduction in vertebral fractures compared with 2014, 33% reduction in surgical fractures compared with 2015 and 66% reduction in surgical hip fractures compared with 2014. An analysis after 6 years of operation and including 196 men and women older than 60 years presenting with a hip fracture, two or more vertebral fractures, or a vertebral fracture plus another fragility fracture, 89.2% of the patients remained without new fractures in the study period. In the group of patients at higher risk—with previous hip fractures (n = 89)—only eight new fractures occurred over the 6-year period, i.e., 93% of the patients remained free from new fractures [28]. In our cohort, using Kaplan–Meier analysis to estimate the incidence of new fractures over 24 months, we identified that 87.9% of the patients would not have new fragility fractures during the follow-up period, corroborating the literature data.
Limitations of the present study include the absence of a control group and the small sample size. According to a recent review on the efficacy and efficiency of FLSs [29], no randomized clinical trials have been conducted to date demonstrating superiority of FLSs in reducing the risk of fracture, perhaps because of the logistical and ethical challenges of carrying out such studies. The author of the review reported that the sample needed to demonstrate a 25% reduction in refractures in 2 years with an expected 12% refracture rate would exceed 15,000 participants and take more than 4 years to complete. It also does not seem appropriate to use as a control group those patients who do not attend or choose not to be treated at the FLS, as this approach would result in a large selection bias (known as “immortal”) since these patients would not have the opportunity to experience the outcome in part of the follow-up during the study. Furthermore, patients who attend FLSs tend to be healthier and have fewer comorbidities. The median follow-up time of 13 months (2–24 months) in our study was also short. The incidence of new fractures is known to not be constant as it fluctuates over time, with 25% of them occurring in the first year and 50% in the first 5 years after the initial fracture [30]. Half of the risk of a new fracture occurs within 2 years from the sentinel fracture, a period known as “imminent fracture risk” [31]. Additionally, the COVID-19 pandemic affected the adherence of the patients in our study, as it prevented face-to-face consultations and exams from being carried out. Many patients ended up interrupting treatment or having irregular adherence to medication use due to difficult contact or follow-up.
Conclusion
The results of the present study suggest that setting up a secondary fracture prevention service is effective in reducing the risk of new fractures in high-risk patients, i.e., those with a recent fracture due to bone fragility. In our sample, 87.9% of the patients would not have new fragility fractures during the 24-month follow-up period. More studies with longer follow-ups and larger sample sizes are needed to confirm these findings.
References
McCloskey E (2009) FRAX® identifying people at high risk of fracture: WHO fracture risk assessment tool, a new clinical tool for informed treatment decisions. Nyon, Switzerland
Seeman E, Delmas PD (2006) Bone quality the material and structural basis of bone strength and fragility. N Engl J Med 354:2250–2261
Johnell O, Kanis JA (2004) An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Intl 15:897–902
Johnell O, Kanis JA (2006) An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int 17:1726–1733
Oden A, McCloskey EV, Johansson H et al (2013) Assessing the impact of osteoporosis on the burden of hip fractures. Calcif Tissue Int 92:42–49
Cooper C, Ferrari S. IOF Compendium 2017, 1st edn. International Osteoporosis Foundation
Zerbini CA, Szejnfeld VL, Abergaria BH et al (2015) Incidence of hip fracture in Brazil and the development of a FRAX model. Arch Osteoporos 10:224
Moraes LF, Silva EN, Silva DA et al (2014) Expenditures on the treatment of osteoporosis in the elderly in Brazil (2008–2010): analysis of associated factors. Rev Bras Epidemiol 17:719–734
Singer A, Exuzides A, Spangler L et al (2015) Burden of illness for osteoporotic fractures compared with other serious diseases among postmenopausal women in the United States. Mayo Clin Proc 90:53–62
Gauthier A, Kanis JA, Jiang Y et al (2011) Epidemiological burden of postmenopausal osteoporosis in the UK from 2010 to 2021: estimations from a disease model. Arch Osteoporos 6:179–188
Marsh D, Akesson K, Beaton DE et al (2011) Coordinator-based systems for secondary prevention in fragility fracture patients. Osteoporos Int 22:2051–2065
Gallagher JC, Melton LJ, Riggs BL et al (1980) Epidemiology of fractures of the proximal femur in Rochester, Minnesota. Clin Orthop Relat Res 150:163–171
Port L, Center J, Briffa NK et al (2003) Osteoporotic fracture: missed opportunity for intervention. Osteoporos Int 14:780–784
McLellan A, Reid D, Forbes K, Reid R, Campbell C, Gregori A, Raby N, Simpson A (2004) Effectiveness of strategies for the secondary prevention of osteoporotic fractures in Scotland (CEPS 99/03) [Internet]. NHS Quality Improvement Scotland, Glasgow. http://www.healthcareimprovementscotland.org/previous_resources/audit_report/osteoporotic_fractures_audit.aspx. Accessed 9 July 2012
EdwardS BJ, Bunta AD, Simonelli C et al (2007) Prior fractures are common in patients with subsequent hip fractures. Clin Orthop Relat Res 461:226–230
Klotzbuecher CM, Ross PD, Landsman PB et al (2000) Patients with prior fractures have an increased risk of future fractures: a summary of the literature and statistical synthesis. J Bone Miner Res 15:721–739
Kanis JA, Johnell O, De Laet C et al (2004) A meta-analysis of previous fracture and subsequent fracture risk. Bone 35:375–382
Dell R (2011) Fracture prevention in Kaiser Permanente Southern California. Osteoporos Int 22:S457-460
Hooven F, Gehlbach SH, Pekow P et al (2005) Follow-up treatment for osteoporosis after fracture. Osteoporos Int 16:296–301
Malik AT, Retchin S, Phillips FM et al (2020) Declining trend in osteoporosis management and screening following vertebral compression fractures–a national analysis of commercial insurance and medicare advantage beneficiaries. Spine J 20:538–546
Solomon DH, Johnston SS, Boyston NN et al (2014) Osteoporosis medication use after hip fractures in US patients between 2002 and 2011. J Bone Miner Res 29:1929–1937
King AB, Saag KG, Burge RT et al (2005) Fracture reduction affects medicare economics (FRAME): impact of increased osteoporosis diagnosis and treatment. Osteoporos Int 16:1545–1557
Mitchell PJ (2013) Fracture liaison services in the United Kingdom. Curr Osteoporos Rep 11:377–384
Wu CH, Te Tu S, Chang YF et al (2018) Fracture liaison services improve outcomes of patients with osteoporosis-related fractures: a systematic literature review and metanalysis. Bone 111:92–100
Gelbach S, Saag KG, Adachi JD et al (2012) Previous fractures at multiple sites increase the risk for subsequent fractures: the global longitudinal study of osteoporosis in women. J B Miner Res 27:645–653
Li N, Hiligsman M, Boonen A, van Oostwaard MM, de Bot RTA, Wyers CE, Bours SPG, van der Bergh JP (2021) The impact of fracture liaison services os subsequent fractures and mortality: a systematic literature review and meta-analysis. Osteoporos Int 32:1517–1530
Axelsson KF, Jacobsson R, Lund D et al (2016) Effectiveness of a minimal resource FLS. Osteoporos Int 27:3165–3175
Stolnicki B, Galdino R, Melo R et al (2017) Zoledronic acid in patients at imminent risk of fractures in a FLS in Rio de Janeiro. Osteoporos Int 28:S313
Javaid MK (2021) Efficacy and efficiency of FLS to reduce the risk of recurrent osteoporosis fractures. Aging Clin Exp Res 33:2061–2067
Van Geel TACM, Van Helden S, Geusens PP et al (2009) Clinical subsequent fractures cluster in time after first fractures. Ann Rheum Dis 68:99–102
Pinedo-Villanueva R, Charokopou M, Toth E et al (2019) Imminent fracture risk assessments in the UK FLS setting: implications and challenges. Arch Osteoporos 14:12
Funding
No funding was received for conducting this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no competing interests to declare that are relevant to the content of this article.
Ethical approval
The study project was approved by the Research Ethics Committee of Universidade Positivo with the number 13433819.9.0000.0093.
Informed consent
All patients agreed to participate in the study and signed an informed consent form.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Inácio, A.M., Marques, L.L.M., Borba, V.Z.C. et al. Incidence of fractures and clinical profile of patients following up at a Fracture Liaison Service in the city of Curitiba. Aging Clin Exp Res 34, 1885–1891 (2022). https://doi.org/10.1007/s40520-022-02116-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-022-02116-w