
Abstract
Purpose
To critically review pregnancy-induced pharmacokinetic changes and their clinical application.
Methods
Structured review of Pubmed, MBASE and published books.
Results
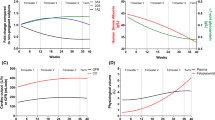
For many drugs, advanced pregnancy is associated with lower maternal serum concentrations. As most drug concentrations are not measured routinely, such changes are not evident to the clinician. Moreover, even for drug concentrations measured clinically, one cannot interpret lower total drug levels as evidence of lower fraction of free drug, which is the pharmacologically- active component, due to lower protein binding of many drugs in late pregnancy. Higher fractions of free drug will lead to higher rate of hepatic metabolism, especially for high extraction medications, leading to lower total drug concentrations.. Pregnancy- induced larger volume of distribution will lead to lower peak of drugs and hence may impact the achievement therapeutic levels. To further complicate matters, the adherence of many women decreases during pregnancy, mostly due to fears of adverse fetal effects. These dynamic and complex processes make changes in recommendations for dose schedule very challenging and in many cases not practical.
Conclusions
Indeed, there are presently no pregnancy- targeted dose schedules, similar to existing dose changes, for example, in renal failure. Similar to the recent increased attention given to pharmacokinetic changes in pregnancy, well designed studies should compare dose-effect relationships in women receiving medications in different stages of pregnancy, to women receiving the same drug before, and/or after pregnancy. Whenever possible, women with chronic conditions can serve as their own controls and decrease the uncertainty created by inter- patient variability. Measuring drug effects in parallel to drug concentrations, will allow pharmacokinetic- pharmacodynamic modelling, leading to evidence-based decisions regarding changes in dose schedules during gestation.
Similar content being viewed by others

References
Koren G, Pastuszak AP, Ito S. Drugs in pregnancy. N Engl J Med. 1998;338:1128–37.
Pariente G, Leibson T, Carls A, Adams-Webber T, Ito S, Koren G. Pregnancy-associated changes in pharmacokinetics: a systematic review. PLoS Med. 2016;13:e1002160. https://doi.org/10.1371/journal.pmed.1002160.eCollection2016Nov.
Gedeon C, Koren G. Designing pregnancy centered medications: drugs which do not cross the human placenta. Placenta. 2006;27:861–8.
Parry E, Shields R, Turnbull A. Transit Time in the small intestine in pregnancy. J Obstet Gynaecol Br Commonw 1970; 77: 900–901.
Costantine MM. Physiologic and pharmacokinetic changes in pregnancy. Front Pharmacol. 2014;5:65. https://doi.org/10.3389/fphar.2014.00065.eCollection2014.
Clark SM, Dutta E, Hankins GD: The outpatient management and special considerations of nausea and vomiting in pregnancy. Semin Perinatol 2014;38:496–502.
Chan MT, Mainland P, Gin T: Minimum alveolar concentration of halothane and enflurane are decreased in early pregnancy. Anesthesiology 1996;85(4):782–786.
Palahniuk RJ, Shnider SM, Eger EI. Pregnancy decreases the requirement for inhaled anesthetic agents. Anesthesiology. 1974;41:82–3. https://doi.org/10.1007/s40268-015-0110-z.
Wood M, Wood MB. Changes in plasma drug binding. And alpha 1-acid glycoprotein in mother and newborn infant. Clin Pharmacol Ther. 1981;29:522–6.
Davis M, Simmons CJ, Dordini B, et al. Induction of hepatic enzymes during normal pregnancy. J Obstet Gynaecol Br Commonw. 1973;80:690–4.
Dickmann LJ, Isoherranen N. Quantitative prediction of CYP2B6 induction by estradiol during pregnancy: potential explanation for increased methadone clearance during pregnancy. Drug Metab Dispos. 2013;41:270–4.
Aldridge A, Bailey J, Neims AH. The disposition of caffeine during and after pregnancy. Semin Perinatol. 1981;5:310–4.
Westin AA, Brekke M, Molden E, et al. Treatment with antipsychotics in pregnancy: changes in drug disposition. Clin Pharmacol Ther. 2017; https://doi.org/10.1002/cpt.770.
Dempsey D, Tutka P, Jacob IIIP, et al. Nicotine metabolite ratio as an index of cytochrome P450 2A6 metabolic activity. Clin Pharmacol Ther. 2004;76:64–72.
Koren G. Nicotine-replacement therapy in pregnancy-the end of the road? Ther Drug Monit. 2012;34:487–8.
Tomson T, Lindbom U, Ekqvist B, et al. Disposition of carbamazepine and phenytoin in pregnancy. Epilepsia. 1994;35:131–5.
McGready R, Stepniewska K, Seaton E, et al. Pregnancy and use of oral contraceptives reduces the biotransformation of proguanil to cycloguanil. Eur J Clin Pharmacol. 2003;59:553–7.
Wadelius M, Darj E, Frenne G, et al. Induction of CYP2D6 in pregnancy. Clin Pharmacol Ther. 1997;62:400–7.
Hogstedt S, Lindberg B, Rane A. Increased oral clearance of metoprolol in pregnancy. Eur J Clin Pharmacol. 1983;24:217–20.
Heikkinen T, Ekblad U, Palo P, et al. Pharmacokinetics of fluoxetine and norfluoxetine in pregnancy and lactation. Clin Pharmacol Ther. 2003;73:330–7.
Liu YT, Hao HP, Liu CX, Wang GJ, Xie HG. Drugs as CYP3A probes, inducers, and inhibitors. Drug Metab Rev. 2007;39:699–721.
Prevost RR, Akl SA, Whybrew WD, et al. Oral nifedipine pharmacokinetics in pregnancy-induced hypertension. Pharmacotherapy. 1992;12:174–7.
de Haan GJ, Edelbroek P, Segers J, et al. Gestation-induced changes in lamotrigine pharmacokinetics: a monotherapy study. Neurology. 2004;63:571–3.
Gerdin E, Salmonson T, Lindberg B, et al. Maternal kinetics of morphine during labour. J Perinat Med. 1990;18:479–87.
De Sousa Mendes M, Hirt D, et al. Physiologically-based pharmacokinetic modeling of renally excreted antiretroviral drugs in pregnant women. Br J Clin Pharmacol. 2015;80:1031–41.
Hebert MF, Easterling TR, Kirby B, et al. Effects of pregnancy on CYP3A and P-glycoprotein activities as measured by disposition of midazolam and digoxin. Clin Pharmacol Ther. 2008;84:248–53.
Bergagnini-Kolev MC, Hebert MF, Easterling TR, Lin YS. Pregnancy increases the renal secretion of N1-methylnicotinamide, an endogenous probe for renal cation transporters, in patients prescribed metformin. Drug Metab Dispos. 2017;45(3):325–9.
Eyal S, Easterling TR, Carr D, Umans JG, Miodovnik M, Hankins GD, et al. Pharmacokinetics of metformin during pregnancy. Drug Metab Dispos. 2010;38(5):833–40.
Andrew MA, Easterling TR, Carr DB, Shen D, Buchanan ML, Rutherford T, et al. Amoxicillin pharmacokinetics in pregnant women: modeling and simulations of dosage strategies. Clin Pharmacol Ther. 2007;81(4):547–56.
Koren G. Depression and perception of teratogenic risk. Isr J Psychiatry Relat Sci. 2014;51:106–8.
Kanji S, et al. Reporting guidelines for clinical pharmacokinetic studies: the ClinPK statement. Clin Pharmacokinet. 2015;54:783–95.
Koren G, Bologa M, Long D, et al. Perception of teratogenic risk by pregnant women exposed to drugs and chemicals during the first trimester. Am J Obstet Gynecol. 1989;160:1190–4.
Tomson T, Landmark CJ, Battino D. Antiepileptic drug treatment in pregnancy: changes in drug disposition and their clinical implications. Epilepsia. 2013;54:405–14.
Vinayakumar D, Vinod GV, Madhavan S, Krishnan MN. Maternal and fetal outcomes in pregnant women undergoing balloon mitral valvotomy for rheumatic mitral stenosis. Indian Heart J. 2016;68:780–2.
Author information
Authors and Affiliations
Corresponding author
Additional information
Guest Editor: Sara Eyal
Rights and permissions
About this article

Cite this article
Koren, G., Pariente, G. Pregnancy- Associated Changes in Pharmacokinetics and their Clinical Implications. Pharm Res 35, 61 (2018). https://doi.org/10.1007/s11095-018-2352-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11095-018-2352-2