
Abstract
Purpose
The aim of this study was to evaluate the effect of different clinical covariates on tacrolimus dose requirements in adult kidney transplant patients with a specific focus on drug interactions.
Patients
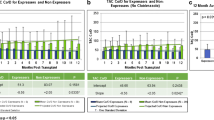
Tacrolimus dosing requirement, normalized by drug levels and expressed as the concentration/dose (C/D) ratio as a surrogate index of tacrolimus bioavailability, was employed to identify four categories of tacrolimus dosing requirement, namely, very high, high, small, and very-small, in very fast, fast, slow, and very slow metabolizers, respectively. Steroid weight-based doses were analyzed instead of fixed doses, and genetic analysis of cytochrome P450 (CYP) 3A5*1/*3 and multi-drug resistance 1 (MDR1) C3435T and C1236T polymorphisms were performed
Results
Multivariate analysis on 450 adult transplant patients identified six risk factors for being slow metabolizers and therefore requiring small tacrolimus doses: male sex (OR 1.615, p = 0.020); age >60 years (OR 2.456, p = 0.0005); body mass index ≥25 (OR 1.546, p = 0.046), hepatitis C virus positivity (OR 2.800, p = 0.0004); low steroid dose <0.06 mg/kg (OR 3.101, p < 0.0001). Patients with a small tacrolimus requirement were at increased risk for multiple infections (OR 1.533, p = 0.0008) and higher systolic blood pressure (OR 1.385, p = 0.022) and showed a significant association with the CYP3A5*3/*3 genotype adjusted by MDR1 polymorphisms C3435T and C1236T (OR 8.104, p = 0.0001).
Conclusions
Our results demonstrate the importance of the interaction among genetic and clinical factors in conditioning tacrolimus disposition, with corticosteroid weight-based dose being the only modifiable risk factor for tacrolimus requirement. As the tacrolimus dosing requirement increases with increasing tacrolimus clearance through concomitant steroid use, undesirable changes in tacrolimus levels may occur when steroid doses are tapered, predominantly in slow metabolizers. This often neglected drug interaction has to be monitored to optimize tacrolimus exposure in kidney transplant patients.

Similar content being viewed by others


References
Scott LJ, McKeage K, Keam SJ et al (2003) Tacrolimus. Drugs 63:1247–1297
Iwasaki K, Shiraga T, Masuda H, Nagase K, Tokuma Y, Hata T, Fujii Y, Sakuma S, Fujitsu T, Fujikawa A, Shimatami K, Sato A, Fujioka M (1995) Further metabolism of KK 506 (Tacrolimus). Identification and biological activities of the metasbolites oxidized at multiple sites of FK 506. Drug Metab Dispos 23:28–34
Iwasaki K (2007) Metabolism of tacrolimus (FK506) and related topics in clinical pharmacokinetics. Drug Metab Pharmacokinet 22:328–335
Tamura K, Kobayashi M, Hashimoto K, Kojima K, Nagase K, Iwasaki K, Kaizu T, Tanaka H, Niwa M (1987) A highly sensitive method to assay FK-506 levels in plasma. Transplant Proc 19:23–29
Staatz CE, Tett SE (2004) Clinical pharmacokinetics and pharmacodynamics of tacrolimus in solid organ transplantation. Clin Pharmacokinet 43:623–653
Coto E, Tavira B (2009) Pharmacogenetics of calcineurin inhibitors in renal transplantation. Transplantation 88:S62–S67
Press RR, Ploeger BA, den Hartigh J et al (2009) Explaining variability in tacrolimus pharmacokinetics to optimize early exposure in adult kidney transplant recipients. Ther Drug Monit 31:187–197
Bai JP, Lesko LJ, Burckart GJ (2010) Understanding the genetic basis for adverse drug effects: the calcineurin inhibitors. Pharmacotherapy 30:195–209
Renders L, Frisman M, Ufer M (2006) CYP 3A5 Genotype markedly influences the pharmacokinetics of tacrolimus and sirolimus in kidney transplant recipients. Clin Pharmacol Ther 81:228–234
Felipe CR, de Sandes TV, Mandia Sampaio EL et al (2009) Clinical Impact of polymorphisms of transport proteins and enzymes involved in the metabolism of immunosuppressive drugs. Transplant Proc 41:1441–1455
Capron A, Mourad M, De Meyer M et al (2010) CYP3A5 and ABCB1 polymorphisms influence tacrolimus concentrations in peripheral blood mononuclear cells after renal transplantation. Pharmacogenomics 11:703–714
Kuypers DR, de Jonge H, Naesens M et al (2007) CYP3A5 and CYP3A4 but not MDR1 single-nucleotide polymorphisms determine the long-term tacrolimus disposition and drug-related nephrotoxicity in renal recipients. Clin Pharmacol Ther 82:711–725
Li D, Gui R, Huang Z et al (2006) Tacrolimus dosing in Chinese renal transplant patients is related to MDR1 gene C3435T polymorphisms. Transplant Proc 38:2850–2852
Fredericks S, Moreton M, Reboux S et al (2006) Multidrug resistance gene 1 (MDR-1) haplotypes have a minor influence on tacrolimus dose requirements. Transplantation 82:705–708
Staatz CE, Goodman LK, Tett SE (2010) Effect of CYP3A and ABCB1 single nucleotide polymorphisms on the pharmacokinetics and pharmacodynamics of calcineurin inhibitors: Part I. Clin Pharmacokinet 49:141–175
Barry A, Levine M (2010) A Systematic review of the effect of CYP3A5 genotype on the apparent oral clearance of tacrolimus in renal transplanted patients. Ther Drug Monit 32:708–714
Kamdem LK, Streit F, Zanger UM, Brockmöller J, Oellerich M, Armstrong VW, Wojnowski L (2005) Contribution of CYP3A5 to the in vitro hepatic clearance of tacrolimus. Clin Chem 51(8):1374–1381
Anglicheau D, Flamant M, Schlageter MH et al (2003) Pharmacokinetic interaction between corticosteroids and tacrolimus after renal transplantation. Nephrol Dial Transplant 18:2409–2414
Fu SJ, Wang YB, Yu LX et al (2008) Factors responsible for inter-individual variations in dosage/concentration of tacrolimus in renal transplant recipients. Nan Fang Yi Ke Da Xue Xue Bao 28:2161–2164
Chen JS, Li LS, Cheng DR et al (2009) Effect of CYP3A5 genotype on renal allograft recipients treated with tacrolimus. Transplant Proc 41:1557–1561
Wang J (2009) CYP3A5 polymorphisms and immunosuppressive drugs in solid-organ transplantation. Expert Rev Mol Diagn 9:383–390
Zhao JY, Ikeguchi M, Eckersberg T, Kuo MT (1993) Modulation of multidrug resistance gene expression by dexamethasone in cultured hepatoma cells. Endocrinology 133:521–528
Demeule M, Jodoin J, Beaulieu E, Brossard M, Beliveau R (1999) Dexamethasone modulation of multidrug transporters in normal tissues. FEBS Lett 442:208–214
El-Sankary W, Plant NJ, Gibson GG, Moore DJ (2000) Regulation of the CYP3A4 gene by hydrocortisone and xenobiotics: role of the glucocorticoid and pregnane X receptors. Drug Metab Dispos 28:493–496
McCune JS, Hawke RL, LeCluyse EL et al (2000) In vivo and in vitro induction of human cytochrome P4503A4 by dexamethasone. Clin Pharmacol Ther 68:356–366
Shimada T (2002) Lowered blood concentration of tacrolimus and its recovery with changes in expression of CYP3A and P-glycoprotein after high-dose steroid therapy. Transplantation 74:1419–1424
Kuypers DR (2008) Influence of interactions between immunosuppressive drugs on therapeutic drug monitoring. Ann Transplant 13:11–18
Lam S, Partovi N, Ting LS, Ensom MH (2008) Corticosteroid interactions with cyclosporine, tacrolimus, mycophenolate, and sirolimus: fact or fiction? Ann Pharmacother 42:1037–1047
Park SI, Felipe CR, Pinheiro-Machado PG (2009) Tacrolimus pharmacokinetic drug interactions: effect of prednisone, mycophenolic acid or sirolimus. Fundam Clin Pharmacol 23:137–145
Lemahieu WP, Maes BD, Vanrenterghem Y (2005) Different evolution of trough and dose levels during the first year after transplantation for tacrolimus versus cyclosporine. Transplant Proc 37:2051–2053
Hesselink DA, Ngyuen H, Wabbijn M, Gregoor PJ, Steyerberg EW, van Riemsdijk IC, Weimar W, van Gelder T (2003) Tacrolimus dose requirement in renal transplant recipients is significantly higher when used in combination with corticosteroids. Br J Clin Pharmacol 56(3):327–330
van Duijnhoven EM, Boots JM, Christiaans MH, Stolk LM, Undre NA, van Hooff JP (2003) Increase in tacrolimus trough levels after steroid withdrawal. Transplant Int 16(10):721–725
Masuda S, Inui K (2006) An up-date review on individualised dosage adjustments of calcineurin inhibitors in organ transplant patients. Pharmacol Ther 112:184–198
Golshayan D, Pascual M (2008) Minimization of calcineurin inhibitors to improve long-term outcomes in kidney transplantation. Transpl Immunol 2:21–28
Tsunoda SM, Aweeka FT (1996) The use of therapeutic drug monitoring to optimize immunosuppressive therapy. Clin Pharmacokinet 30:107–140
Wilkinson A, Davidson A, Dotta J et al (2005) Guidelines for the treatment and management of new-onset diabetes after transplantation. Clin Transplant 19:291–298
Hu YF, He J, Chen GL (2005) CYP3A5*3 and CYP3A4*18 single nucleotide polymorphisms in a Chinese population. Clin Chim Acta 353(1–2):187–192
Wu L, Xu X, Shen J et al (2007) MDR1 gene polymorphisms and risk of recurrence in patients with hepatocellular carcinoma after liver transplantation. J Surg Oncol 96(1):62–68
de Wildt SN, van Schaik RH, Soldin OP, Soldin SJ, Brojeni PY, van der Heiden IP, Parshuram C, Nulman I, Koren G (2011) The interactions of age, genetics, and disease severity on tacrolimus dosing requirements after pediatric kidney and liver transplantation. Eur J Clin Pharmacol. 23 Jun 23 [Epub ahead of print]
Kuypers DR, Claes K, Evenepoel P, Maes B, Coosemans W, Pirenne J, Vanrenterghem Y (2004) Time-related clinical determinants of long-term tacrolimus pharmacokinetics in combination therapy with mycophenolic acid and corticosteroids: a prospective study in one hundred de novo renal transplant recipients. Clin Pharmacokinet 43(11):741–762
Ferraris JR, Argibay PF, Costa L, Jimenez G, Coccia PA, Ghezzi LF, Ferraris V, Belloso WH, Redal MA, Larriba JM (2011) Influence of CYP3A5 polymorphism on tacrolimus maintenance doses and serum levels after renal transplantation: age dependency and pharmacological interaction with steroids. Pediatr Transplant 15(5):525–532
Gijsen V, Mital S, van Schaik RH, Soldin OP, Soldin SJ, van der Heiden IP, Nulman I, Koren G, de Wildt SN (2011) Age and CYP3A5 genotype affect tacrolimus dosing requirements after transplant in pediatric heart recipients. J Heart Lung Transplant. 17 Sept [Epub ahead of print]
Manzanares C (2002) Therapeutic drug monitoring of tacrolimus: a moving matter. Therapie 57(2):133–136
Rodrigo E, de Cos MA, Sánchez B, Ruiz JC, Piñera C, Fernández-Fresnedo G, Palomar R, Pérez-Ceballos MA, Cotorruelo JG, Zubimendi JA, de Francisco AL, Arias M (2005) High initial blood levels of tacrolimus in overweight renal transplant recipients. Transplant Proc 37(3):1453–1454
Joy MS, Hogan SL, Thompson BD et al (2007) Cytochrome P450 3A5 expression in the kidneys of patients with calcineurin inhibitor nephrotoxicity. Nephrol Dial Tranplant 22:1963–1968
Metalidis C, Lerut E, Naesens M, Kuypers DR (2011) Expression of CYP3A5 and P-glycoprotein in renal allografts with histological signs of calcineurin inhibitor nephrotoxicity. Transplantation 91(10):1098–1102
Naesens M, Kuypers DRJ, Sarwal M (2009) Calcineurin Inhibitor nephrotoxicity. Clin J Am Soc Nephrol 4:481–508
Lamba JK, Lin YS, Schuetz EG, Thummel KE (2002) Genetic contribution to variable human CYP3A-mediated metabolism. Adv Drug Deliv Rev 18:1271–1294
O’Seaghdha CM, McQuillan R, Moran AM et al (2009) Higher tacrolimus trough levels on days 2–5 post-renal transplant are associated with reduced rates of acute rejection. Clin Transplant 23:462–468
De Jonge H, Kuypers DRJ (2008) Pharmacogenetics in solid organ transplantation: current status and future directions. Tranplant Rev 22:6–20
Kuypers DR (2005) Immunosuppressive drug monitoring—what to use in clinical practice today to improve renal graft outcome. Transplant Int 18:140–150
Thervet E, Loriot MA, Barbier S et al (2010) Optimization of initial tacrolimus dose using pharmacogenetic testing. Clin Pharmacol Ther 87:721–726
Van Gelder T, Hesselink DA (2010) Dosing tacrolimus based on CYP3A5 genotype: will it improve clinical outcome? Clin Pharmacol Ther 87:640–641
Kuypers DR (2010) Pharmacogenetic vs. concentration-controlled optimization of tacrolimus dosing in renal allograft recipients. Clin Pharmacol Ther 88:595–596
McLeod HL, Evans WE (2001) Pharmacogenomics: unlocking the human genome for better drug therapy. Annu Rev Pharmacol Toxicol 41:101–121
Burckart GJ, Amur S (2010) Update on the clinical pharmacogenomics of organ transplantation. Pharmacogenomics 11(2):227–236
Zhao W, Elie V, Roussey G et al (2009) Population pharmacokinetics and pharmacogenetics of tacrolimus in de novo pediatric kidney transplant recipients. Clin Pharmacol Ther 86:609–618
Benkali K, Prémaud A, Picard N et al (2009) Tacrolimus population pharmacokinetic-pharmacogenetic analysis and Bayesian estimation in renal transplant recipients. Clin Pharmacokinet 48(12):805–816
Press RR, de Fijter JW, Guchelaar HJ (2010) Individualizing calcineurin inhibitor therapy in renal transplantation-current limitations and perspectives. Curr Pharm Des 16(2):176–186
Phapale PB, Kim S-D, Lee HW (2010) An integrative approach for identifying a metabolic phenotype predictive of individualized pharmacokinetics of tacrolimus. Clin Pharmacol Ther 87:426–436
Conflict of interest disclosure
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Stratta, P., Quaglia, M., Cena, T. et al. The interactions of age, sex, body mass index, genetics, and steroid weight-based doses on tacrolimus dosing requirement after adult kidney transplantation. Eur J Clin Pharmacol 68, 671–680 (2012). https://doi.org/10.1007/s00228-011-1150-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-011-1150-0