
Abstract
Introduction. In the guidelines of the German specialist medical societies, postoperative chemoradiotherapy is recommended for rectal carcinomas in stages II and III. In the meantime, there are important study findings favoring preoperative radiotherapy as against postoperative irradiation. In the present unicentric study, the clinical results after preoperative irradiation and postoperative chemotherapy are to be determined. In period I, sandwich radiation without total mesorectal excision was applied. In period II, the treatment was developed further with exclusive preoperative radiation and total mesorectal excision. Since from 1994 the therapy regimen has changed with the introduction of total mesorectal excision and improved radiotherapy, the present study was carried out to check whether this has led to better results of therapy.
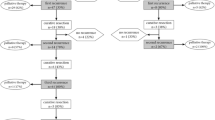
Patients and Methods. Over a period of 7 years, data from 607 patients with rectal carcinoma were recorded and stored in an Excel file. The carcinomas were grouped into lower, middle and upper segment levels and classified endosonographically. Multimodal treatment was administered in stage uT3. In period I, sandwich radiation was carried out with 24 Gy preoperatively and 24 Gy postoperatively, followed by adjuvant chemotherapy. Total mesorectal excision was not performed. In period II, 50.4 Gy were applied preoperatively, followed by adjuvant chemotherapy. The operation comprised total mesorectal excision of the lower two thirds of the rectum. Calcium folinate and 5-fluoroucil were administered in six chemotherapy cycles. Primarily inoperable patients received preoperative irradiation with up to 50.4 Gy in both periods to attain down-staging. The following surgical procedures were applied: abdominal perineal extirpations, deep anterior resections, coloanal anastomoses, colon pouch anal anastomoses and transanal microsurgical resections.
Results. In 469 curatively operated patients, including primarily inoperable patients after down-staging radiotherapy, the rates of local recurrence were 5.8% with a mean follow-up observation of 4.29 years, and the carcinoma-specific 4-year actuarial survival was 84%. The rate of recurrence was highest in the lowest segment level of the rectum (7.6 as compared to 2.4%, P=0.042). The rates of local recurrence were 7.4% in period I and 4.3% in period II (P=0.44). The carcinoma-specific 4-year actuarial survivals were 81% in period I and 87% in period II (P=0.202). Investigation of the subgroups of irradiated patients showed complete freedom from recurrence after a mean follow-up observation time of 3.58 years for patients in stage uT3 with total mesorectal excision, preoperative radiotherapy and postoperative chemotherapy (n=51). The difference from patients without postoperative chemotherapy was significant (P=0.018). After radiotherapy, the complication observed was a raised rate of sacral cavity infections after total resection of the rectum (p=0.039).
Conclusion. Total mesorectal excision, preoperative radiotherapy and postoperative chemotherapy can effectively influence the rate of local recurrences after rectal carcinoma operations (0–4.3% after a mean period of follow-up observation of 3.58 years). No appraisal can be made with regard to the benefit resulting from the individual measures.
Zusammenfassung
Einleitung. In den Leitlinien der deutschen medizinischen Fachgesellschaften wird für Rektumkarzinome in den Stadien II und III eine postoperative Radio-Chemo-Therapie empfohlen. Inzwischen liegen wichtige Untersuchungsergebnisse vor, die für eine präoperative und gegen eine postoperative Radiatio sprechen. In der vorliegenden unizentrischen Studie sollen die klinischen Ergebnisse nach präoperativer Radiatio und postoperativer Chemotherapie ermittelt werden. In einem Zeitraum I wurde eine Sandwichbestrahlung und keine totale mesorektale Exzision angewandt. In einem Zeitraum II wurde die Therapie fortentwickelt mit ausschließlich präoperativer Bestrahlung und totaler mesorektaler Exzision. Da das Therapieregime ab 1994 mit Einführung der totalen mesorektalen Exzision und einer verbesserten Bestrahlungsbehandlung geändert wurde, soll geprüft werden, ob dies zu einer Verbesserung der Therapieergebnisse geführt hat.
Patienten und Methodik. Während 7 Jahren wurden die Daten von 607 Patienten mit Rektumkarzinomen erfasst und in einer Excel-Datei gespeichert. Die Karzinome wurden einer unteren, mittleren und oberen Etage zugeordnet und endosonographisch klassifiziert. Multimodal behandelt wurde im Stadium uT3. Im Zeitraum I erfolgte eine Sandwichbestrahlung mit 24 Gy präoperativ und 24 Gy postoperativ, gefolgt von einer adjuvanten Chemotherapie. Eine totale mesorektale Exzision wurde nicht vorgenommen. Im Zeitraum II wurden 50,4 Gy präoperativ eingestrahlt, gefolgt von einer adjuvanten Chemotherapie. Die Operation umfasste eine totale mesorektale Exzision in den beiden unteren Rektumdritteln. Zur Chemotherapie wurde 5-Fluoro-uracil und Calciumfolinat in 6 Zyklen verabreicht. Primär inoperable Patienten erhielten in beiden Zeiträumen eine präoperative Bestrahlung bis 50,4 Gy zur Erzielung eines Downstaging. An operativen Methoden wurden angewandt: abdominoperineale Exstirpationen, tiefe anteriore Resektionen, koloanale Anastomosen, Kolon-Pouch-anale Anastomosen sowie transanale mikrochirurgische Resektionen.
Ergebnisse. Bei 469 kurativ operierten Patienten unter Einschluss von Patienten nach Downstaging-Radiatio bei primärer Inoperabilität betrugen die Lokalrezidivraten bei einer mittleren Nachbeobachtungszeit von 4,29 Jahren 5,8% und die karzinomspezifische 4-Jahres-Überlebensrate 84%. Die Rezidivrate war in der untersten Rektumetage am höchsten (7,6 vs. 2,4%, p=0,042). Die Lokalrezidivraten betrugen im Zeitraum I 7,4% und im Zeitraum II 4,3% (p=0,44). Die karzinomspezifischen 4-Jahres-Überlebensraten betrugen im Zeitraum I 81% und im Zeitraum II 87% (p=0,202). Die Untersuchung der Untergruppen von Bestrahlungspatienten ergab für Patienten im Stadium uT3 mit totaler mesorektaler Exzision, präoperativer Radiatio und postoperativer Chemotherapie (n=51) eine vollständige Rezidivfreiheit nach einer mittleren Nachbeobachtungszeit von 3,58 Jahren. Der Unterschied zu Patienten ohne postoperative Chemotherapie war signifikant (p=0,018). An Komplikationen nach Bestrahlung war eine erhöhte Rate von Sakralhöhleninfekten nach Rektumexstirpationen festzustellen (p=0,04).
Schlussfolgerung. Unter Anwendung der totalen mesorektalen Exzision, einer präoperativen Radiatio und postoperativen Chemotherapie kann das Auftreten von Lokalrezidiven nach Rektumkarzinomoperationen wirksam beeinflusst werden (0–4,3% nach einer mittleren Nachbeobachtungszeit von 3,58 Jahren). Zur Wertigkeit der einzelnen Maßnahmen kann keine Aussage gemacht werden.
Similar content being viewed by others


Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Thomschke, D., Kyau-Ummen, B. & Halbfaß, H. Lokalrezidiv- und Überlebensraten nach Rektumkarzinomoperationen und multimodaler Therapie. Chirurg 73, 245–254 (2002). https://doi.org/10.1007/s00104-002-0428-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00104-002-0428-2