Repair of Perineal Hernia Following Abdominoperineal Excision with Biological Mesh: A Systematic Review
 Sunil K. Narang
Sunil K. Narang Nasra N. Alam
Nasra N. Alam Ferdinand Köckerling
Ferdinand Köckerling Ian R. Daniels
Ian R. Daniels Neil J. Smart
Neil J. Smart- 1Exeter Surgical Health Services Research Unit (HeSRU), Royal Devon and Exeter Hospital, Exeter, Devon, UK
- 2Department of Surgery, Center for Minimally Invasive Surgery, Vivantes Hospital, Academic Teaching Hospital of Charité Medical School, Berlin, Germany
Introduction: Perineal hernia (PerH) following abdominoperineal excision (APE) procedure is a recognized complication. PerH was considered an infrequent complication of APE procedure; however, PerH rates of up to 45% have been reported in recent publications following a laparoscopic APE procedure. Various methods of repair of PerH with the use of synthetic meshes or myocutaneous flap have been described, although there is no general agreement on an optimal strategy. The use of biological meshes for different operations is growing in popularity, and these have been promoted as being superior and safer when compared to synthetic meshes. Although the use of biologics is becoming popular claims of better outcomes are largely unsupported by evidence. The aim of this systematic review is to evaluate the currently available evidence supporting the use of biologic or biosynthetic meshes for the repair of PerH that develop following an APE.
Methods: A systematic review of all English language literature relevant to repair of PerH following APE with biologic or biosynthetic mesh published between January 1, 2000 and July 31, 2016 was carried out using MEDLINE, EMBASE, and the Cochrane Library of Systematic Reviews for relevant literature. Searches were performed using a combination of Medical Subject Headings (MeSH) terms and text words “PerH,” “APE,” “morbidity,” “biologics,” “biosynthetic,” and “hernia.” Studies in which the use of biological meshes was not reported were excluded from the review. Various outcome measures, including operative technique, complication rates, recurrence rates, type of mesh, management of recurrences, and risk factors, were extracted. Oxford Centre for Evidence-based Medicine – Levels of Evidence (March 2009) was used to assess the quality of evidence.
Results: The systematic review of the literature identified three case reports, four case series, and one pooled analysis that were included in the final review. Overall, these studies were of poor quality providing level 4 evidence. Various different approaches and techniques of repair of PerH were described; however, it was difficult to extract information with regard to the primary and secondary outcome measures.
Conclusion: There is no general agreement to the optimal operative strategy to repair PerH following an APE. There is insufficient evidence to recommend any specific operative approach or repair technique for PerH following an APE.
Introduction
The finding of a perineal hernia (PerH) following an abdominoperineal excision (APE) is a recognized complication; however, it is unclear as to how frequently this occurs. Until a few years ago, they were considered to be an infrequent complication following an APE and prevalence rates of 0.6–7% were reported (1–6). However, the surgical management of rectal cancer has evolved over the recent years with the acceptance of the principle of total mesorectal excision (TME) and the recognition of the importance of a clear surgical resection and avoidance of tumor perforation during an APE (7). This procedure has evolved into the extra levator abdominoperineal excision (eLAPE) with the potential surgical resection margin information being identified through MRI staging (7, 8). This has resulted in a reduction in circumferential resection margin involvement and intra-operative perforation of the tumor (9). However, an eLAPE creates a wider defect in the pelvic floor leaving only the ischioanal fat and skin for closure of the defect as the entire pelvic floor muscle complex has been excised surrounding the distal rectum. Perineal herniation in this group of patients is increasingly recognized and a recent publication has reported an overall PerH rate of 26% and this can be as high as 45% in those having a laparoscopic eLAPE procedure (10).
A PerH repair may be necessary as the hernia is not only painful but can also result in urinary dysfunction or bowel obstruction causing impairment of daily activities of living. Various methods or repair have been described in the literature, including primary tissue repair, synthetic mesh, biological mesh, and myocutaneous flaps. This repair can be facilitated by either using an abdominal and/or perineal approach although none of the described repairs are well established.
The use of synthetic meshes is associated with problems, such as mesh infection, chronic inflammation, and foreign body reaction. If bowel is in direct contact with the synthetic mesh used for a PerH repair, then there is a risk of adhesions and erosion into the bowel wall by the mesh. Biologic and biosynthetic meshes were developed to overcome such problems. The role of biologic mesh for primary reconstruction of the pelvic floor after eLAPE has been the subject of a systematic review, and this was considered a promising technique for improving wound healing and complication rates comparable to other techniques (11). Biologic meshes have been used recently as an alternative for repairing PerH following an eLAPE. The biologic mesh acts not only as a structural support for the hernia repair but also as a scaffold allowing the ingrowth of native fibroblasts, which in turn lay down the fibrous tissue and promote tissue remodeling (12). The aim of this systematic review is to evaluate the currently available evidence supporting the use of biologic or biosynthetic meshes for the repair of PerH.
Methods
Search Strategy
A systematic review of all English language literature relevant to the repair of a PerH following an APE with biologic or biosynthetic mesh published between January 1, 2000 and July 31, 2016 was carried out using MEDLINE (PubMed and Ovid), EMBASE (Ovid), and the Cochrane Library of Systematic Reviews/Controlled Trials for relevant literature. Searches were performed using a combination of Medical Subject Headings (MeSH) terms and text words “perineal hernia,” “abdominoperineal excision,” “morbidity,” “biologics,” “biosynthetic,” and “hernia.” All randomized/non-randomized, controlled/non-controlled clinical trials, prospective observational studies, clinical registry data, retrospective case series, and case reports that reported on repair of PerH following APE were included for analysis. Conference abstracts, letters, technical notes, and commentaries were excluded. In addition, bibliographies from the papers requested were manually checked to identify additional relevant papers.
Study Selection
Titles and abstracts of the identified studies were screened by the main reviewer Sunil K. Narang and independently checked by Nasra N. Alam. Studies that were irrelevant were rejected. The full texts of identified papers were independently assessed by two reviewers (Sunil K. Narang and Nasra N. Alam) to determine whether they met the predetermined inclusion/exclusion criteria. Disagreements were resolved by discussion or adjudication by the senior author (Neil J. Smart).
Inclusion Criteria
All studies should have been published in print or electronic format between 1 January, 2000 and July 31, 2016. Only adult patients undergoing PerH repair following APE were included in the review. An APE may have been performed as an open procedure, laparoscopic, hand-assisted or robot-assisted. PerH repair may have been done using open, laparoscopic, or combined approach. The diagnosis of PerH may have been established based on clinical examination or cross-sectional imaging.
Exclusion Criteria
Studies on the pediatric population or using synthetic mesh or myocutaneous flaps were excluded from this review. Diagnosis of PerH established on the basis of patient-reported symptoms of PerH or telephone or postal follow-up were excluded from the review.
Outcomes
The primary outcome measure of the systematic review was to assess the recurrence of PerH following repair with biologic or biosynthetic meshes. Other factors, such as time interval to development of PerH and diagnostic definition of PerH (clinical, cross-sectional imaging, patient-reported or telephone interview), were also noted.
The secondary outcome measures recorded were:
1. Complications following repair.
2. Management of recurrences.
3. Patient-reported outcome measures or quality of life scores.
Definitions
Clinically, a PerH is defined as a palpable bulge in the perineum associated with protrusion of intra-abdominal or pelvic viscera through the defect in the pelvic floor fascia and musculature. Radiographic definition of PerH unclear as the landmarks for defining the pelvic floor are not universally agreed.
Quality Assessment
Oxford Centre for Evidence-based Medicine – Levels of Evidence (March 2009) was used to assess the quality of evidence (13).
Data Extraction (Selection and Coding)
Data on the study type, number of patients treated, length of follow-up, cross-sectional imaging, and symptoms from PerH were extracted from the included studies by the reviewers. These data were extracted separately by reviewers (Sunil K. Narang and Nasra N. Alam) to guard against reviewer bias. Any discrepancies were resolved by adjudication by the senior author Neil J. Smart. All data and results of statistical tests were extracted from the papers and entered into an electronic data sheet (Microsoft Excel). For particular outcomes that were to be evaluated, if the data were not specifically reported, they were regarded as not reported or missing and no assumptions were made regarding the missing data.
Statistical Analysis
There was a significant heterogeneity in the included studies in the study design, intervention design, study cohorts, and outcome measures. A weighted analysis of variables for risk factors for PerH development was not possible because of the lack of both uniformity and the quantity of the data reported. For this reason, a meta-analysis of the data could not be performed; therefore, primary and secondary outcome measure parameters are expressed as a range.
Results
A total of 190 potential articles were identified from the initial literature search. After removal of duplicate articles 176 articles remained (Figure 1). Using the inclusion criteria described above, 146 articles were eliminated on title and abstract review. Full text articles were obtained for 30 articles out of which 22 articles were rejected, as they did not meet the inclusion criteria. Eight articles were included for final analysis. Out of the eight articles that were included, three were case reports, four were case series, and one article was a pooled analysis. The quality assessment of the included studies is presented in Tables 1–3. The level of evidence based on the Oxford Centre for Evidence-based Medicine (March 2009) was 4 at best. The pooled analysis included all publications from 1944 to 2010 and has probably included data from Skipworth et al. (14) and de Campos et al. (15). There was a significant variation among studies in their description of diagnostic method, selection criteria, operative technique, type of mesh used, and duration of follow-up, recurrence rates, complications, and management of recurrences. None of the studies in the review used the Clavien Dindo grading of post-operative complications (16).
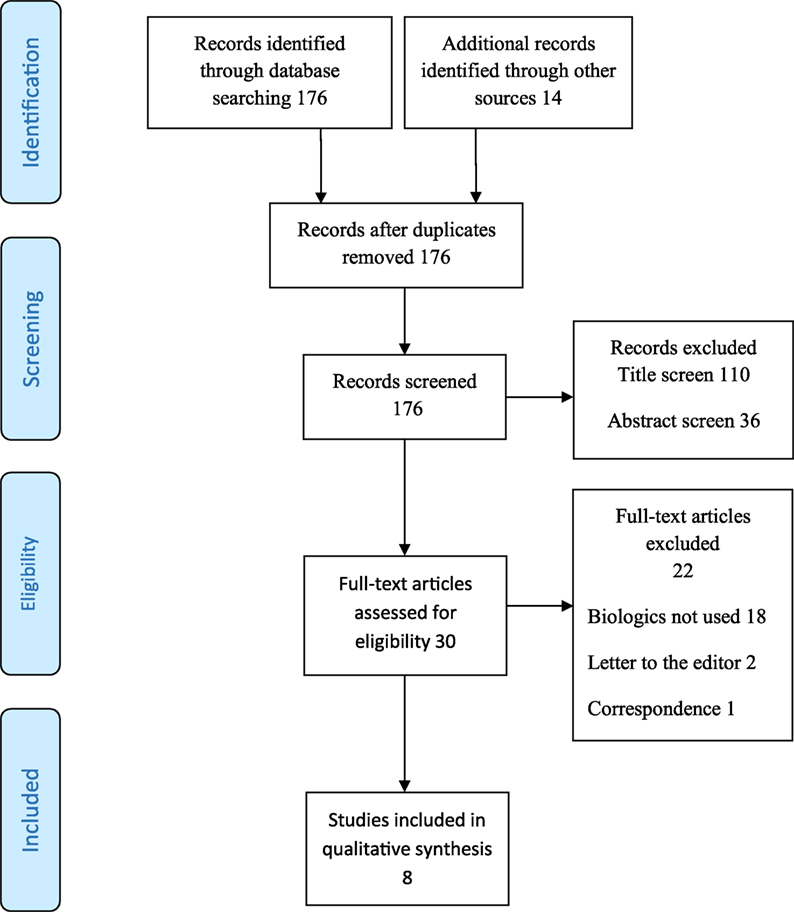
Figure 1. PRISMA flow diagram outlining study selection.
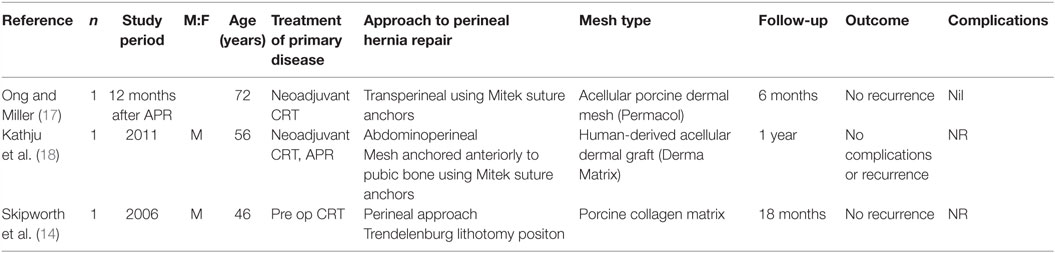
Table 1. Case reports.
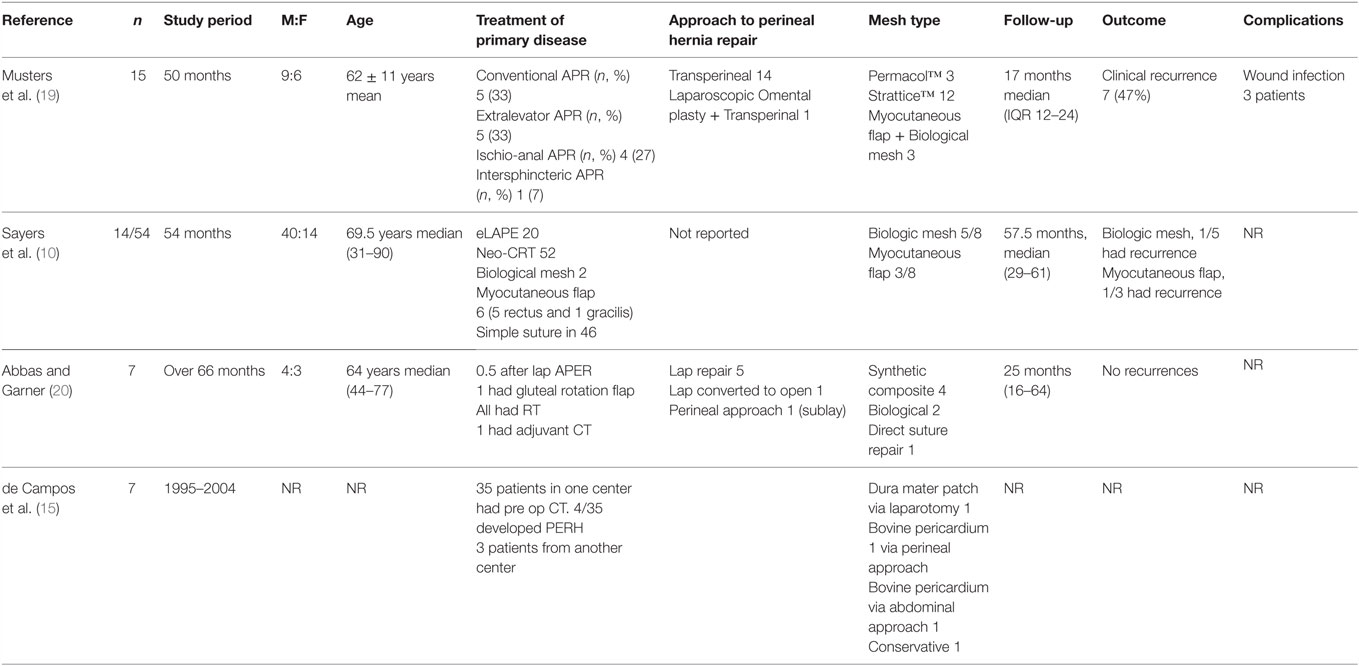
Table 2. Case series.

Table 3. Pooled analysis evidence.
In the three case reports, there were no recurrences following repair of PerH on follow-up ranging from 12 to 18 months (11, 13, 14). Of the four case series, the duration of follow-up and final outcome was not reported in one publication (4, 8, 12). In the remaining three case series, different types of cross and non-cross-linked biologic meshes were used and some patients underwent myocutaneous flap repair and/or omentoplasy in addition to the mesh repair.
The operative technique to repair a PerH varied significantly ranging from perineal repair, open abdominal repair, or combined approach with or without the use of laparoscope. The type of biological mesh used was not reported in three studies. Others described the use of additionally cross-linked acellular porcine collagen (Permacol™), non-cross-linked porcine collagen (Strattice™), Human-derived Acellular Dermal graft (DermaMatrix), Dura mater patch, and Bovine pericardium. Complications following repair were not reported in any of the case reports although the pooled analysis reported a perineal wound breakdown rate of 12% with the use of all different types of synthetic and biologic meshes. Management of recurrence of PerH was reported by Musters et al. and four recurrent PerH were repaired using prolene mesh (19). None of the studies used patient-reported outcome measures to assess the impact of surgery on the quality of life of the patients.
Discussion
A PerH is an incisional hernia through the pelvic floor, which results in protrusion of abdominal or pelvic viscera. There is no universally accepted clinical or radiological definition of a PerH. They are typically diagnosed based on symptoms, such as an expansile cough impulse in the perineum, which is not only uncomfortable but can also cause bowel or bladder symptoms. In the majority of cases, this hernia remains asymptomatic and may be incidentally detected on cross-sectional imaging performed for oncologic follow-up. It is vital that there should be a universally agreed clinical and radiological definition of PerH in order to make meaningful comparison between studies.
Most publications reporting PerH repair following APE are either individual case reports or small retrospective case series with relatively short follow-up. This review includes mostly small case series over a long period of time reporting different techniques performed by different surgeons. These papers are focused on the description of successful technique and are, therefore, prone to publication bias. It appears that myocutaneous flap techniques have a role in repair of PerH when the operative field has been severely damaged by irradiation and can provide a well-vascularized tissue for repair (19, 22). None of the studies compared the use of biologics with either prosthetic mesh or myocutaneous flaps and, therefore, findings of individual studies are difficult to interpret.
Some of the risk factors that may predispose an individual to the development of PerH include female gender, previous hysterectomy, coccygectomy, pre-operative pelvic irradiation, post-operative wound infection, a long small bowel mesentery, high BMI, smoking, and non-closure of the pelvic peritoneum (1, 6, 21, 23, 24). Patients with rectal cancer may have been treated with neoadjuvant chemoradiotherapy. The role of these risk factors has not been evaluated in these studies.
The decision to repair PerH is based on the symptoms, fitness of the patient and oncological stage. Repair may be performed via abdominal, perineal, or combined approach. Laparoscopy has been used in patients with reasonable access. There is no evidence to support the use of any particular approach. The pooled analysis by Mjoli et al. reported 22 perineal repairs, 11 open abdominal operations, 3 combined abdominoperineal approach, 5 laparoscopic repairs, and 2 laparoscopic-perineal procedures (21).
Within the last decade, the eLAPE procedure has become increasing popular and has led to reduction in the circumferential margin positivity rate. However, due to the wider resection of the pelvic floor, the risk of herniation may be higher. The pelvic floor may or may not have been reconstructed using flaps/meshes, etc. There is evidence that laparoscopy results in fewer adhesion in the abdomen and this may contribute to increasing PerH rates as the small and large bowel are free to descend into the pelvis (25, 26). It is likely that the incidence and prevalence of PerH will increase unless there is a much better technique of primary reconstruction of the pelvic floor at the time of APE.
The advent of synthetic absorbable meshes has generated considerable interest within the surgical community. These materials promote fibroblast activity and generate a foreign body reaction. Following complete absorption within 30–90 days, the synthetic material is replaced by collagen rich connective tissue. In this review, only one patient was identified to have undergone repair with an absorbable mesh and this hernia recurred within 16 months (21). The use of biologic mesh for repairing PerH appears attractive as the acellular collagen matrix is believed to allow migration of fibroblasts, neovascularization, and incorporation within the native tissues. This is thought to reduce the risk of wound infection. A recently published case series of 15 patients undergoing PerH repair with porcine acellular dermal mesh reported recurrence rates of 47% after a median follow-up of 17 months (IQR 12–24) (19). However, the low volume, quality of available data, and lack of any comparative studies make it difficult to evaluate the use of biologic meshes as a technique.
Conclusion
There is no general agreement to the optimal operative strategy to repair PerH following an APE. There is insufficient evidence to recommend any specific operative approach or repair technique for PerH following APE.
Author Notes
Previous presentations: The data in this paper have been presented at the Consensus Conference on the clinical use of biologic and biosynthetic meshes in abdominal surgery on Wednesday, January 27, 2016 at Hotel Ellington, Nürnberger Straße 50-55, D-10789 Berlin.
Author Contributions
SN, FK, ID, and NS designed the search; SN and NA performed the search; FK, ID, and NS contributed analytic tools; SN and NA analyzed the data. SN wrote the first draft paper. All authors contributed to revision of the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Aboian E, Winter DC, Metcalf DR, Wolff BG. Perineal hernia after proctectomy: prevalence, risks, and management. Dis Colon Rectum (2006) 49(10):1564–8. doi:10.1007/s10350-006-0669-0
2. Beck M. Perineal hernia: the ventral decubitus perineal approach. J Visc Surg (2011) 148(1):39–41. doi:10.1016/j.jviscsurg.2010.12.006
3. Dulucq J-L, Wintringer P, Mahajna A. Laparoscopic repair of postoperative perineal hernia. Surg Endosc (2006) 20(3):414–8. doi:10.1007/s00464-005-0193-7
4. Rayhanabad J, Sassani P, Abbas MA. Laparoscopic repair of perineal hernia. JSLS (2009) 13(2):237–41.
5. Śmietański M, Szczepkowski M, Alexandre JA, Berger D, Bury K, Conze J, et al. European Hernia Society classification of parastomal hernias. Hernia (2014) 18(1):1–6. doi:10.1007/s10029-013-1162-z
6. So JB, Palmer MT, Shellito PC. Postoperative perineal hernia. Dis Colon Rectum (1997) 40(8):954–7. doi:10.1007/BF02051204
7. Shihab OC, Brown G, Daniels IR, Heald RJ, Quirke P, Moran BJ. Patients with low rectal cancer treated by abdominoperineal excision have worse tumors and higher involved margin rates compared with patients treated by anterior resection. Dis Colon Rectum (2010) 53(1):53–6. doi:10.1007/DCR.0b013e3181c70465
8. Shihab OC, Taylor F, Salerno G, Heald RJ, Quirke P, Moran BJ, et al. MRI predictive factors for long-term outcomes of low rectal tumours. Ann Surg Oncol (2011) 18(12):3278–84. doi:10.1245/s10434-011-1776-2
9. West NP, Anderin C, Smith KJE, Holm T, Quirke P; European Extralevator Abdominoperineal Excision Study Group. Multicentre experience with extralevator abdominoperineal excision for low rectal cancer. Br J Surg (2010) 97(4):588–99. doi:10.1002/bjs.6916
10. Sayers AE, Patel RK, Hunter IA. Perineal hernia formation following extralevator abdominoperineal excision. Color Dis (2015) 17(4):351–5. doi:10.1111/codi.12843
11. Alam NN, Narang SK, Köckerling F, Daniels IR, Smart NJ. Biologic mesh reconstruction of the pelvic floor after extralevator abdominoperineal excision: a systematic review. Front Surg (2016) 3:9. doi:10.3389/fsurg.2016.00009
12. Peacock O, Pandya H, Sharp T, Hurst NG, Speake WJ, Tierney GM, et al. Biological mesh reconstruction of perineal wounds following enhanced abdominoperineal excision of rectum (APER). Int J Colorectal Dis (2012) 27(4):475–82. doi:10.1007/s00384-011-1325-2
13. OCEBM Levels of Evidence – CEBM [Internet]. (2015). Available from: http://www.cebm.net/ocebm-levels-of-evidence/
14. Skipworth RJE, Smith GHM, Anderson DN. Secondary perineal hernia following open abdominoperineal excision of the rectum: report of a case and review of the literature. Hernia (2007) 11(6):541–5. doi:10.1007/s10029-007-0234-3
15. de Campos FGCM, Habr-Gama A, Araújo SE, Sousa AH, Nahas CR, Lupinacci RM, et al. Incidence and management of perineal hernia after laparoscopic proctectomy. Surg Laparosc Endosc Percutan Tech (2005) 15(6):366–70. doi:10.1097/01.sle.0000191592.93326.63
16. Dindo D, Demartines N, Clavien P-A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg (2004) 240(2):205–13. doi:10.1097/01.sla.0000133083.54934.ae
17. Ong SL, Miller AS. A transperineal approach to perineal hernia repair using suture anchors and acellular porcine dermal mesh. Tech Coloproctol (2013) 17(5):605–7. doi:10.1007/s10151-011-0774-5
18. Kathju S, Lasko LA, Medich DS. Perineal hernia repair with acellular dermal graft and suture anchor fixation. Hernia (2011) 15(3):357–60. doi:10.1007/s10029-010-0664-1
19. Musters GD, Lapid O, Stoker J, Musters BF, Bemelman WA, Tanis PJ. Is there a place for a biological mesh in perineal hernia repair? Hernia (2016). Available from: http://link.springer.com/10.1007/s10029-016-1504-8
20. Abbas Y, Garner J. Laparoscopic and perineal approaches to perineal hernia repair. Tech Coloproctol (2014) 18(4):361–364. doi:10.1007/s10151-013-1060-5
21. Mjoli M, Sloothaak DAM, Buskens CJ, Bemelman WA, Tanis PJ. Perineal hernia repair after abdominoperineal resection: a pooled analysis. Colorectal Dis (2012) 14(7):e400–6. doi:10.1111/j.1463-1318.2012.02970.x
22. Hansen MT, Bell JL, Chun JT. Perineal hernia repair using gracilis myocutaneous flap. South Med J (1997) 90(1):75–7. doi:10.1097/00007611-199701000-00018
23. Kelly AR. Surgical repair of post-operative perineal hernia. Aust N Z J Surg (1960) 29:243–5. doi:10.1111/j.1445-2197.1960.tb03845.x
24. Perl JI. Repair of postoperative perineal hernia. Report of a case. J Int Coll Surg (1960) 34:86–92.
25. Svane M, Bulut O. Perineal hernia after laparoscopic abdominoperineal resection – reconstruction of the pelvic floor with a biological mesh (PermacolTM). Int J Colorectal Dis (2012) 27(4):543–4. doi:10.1007/s00384-011-1253-1
26. Beck DE, Fazio VW, Jagelman DG, Lavery IC, McGonagle BA. Postoperative perineal hernia. Dis Colon Rectum (1987) 30(1):21–4. doi:10.1007/BF02556914
Appendix
BioMesh Study Group
Ferdinand Köckerling (Chairman), Stavros Antoniou, René Fortelny, Frank A. Granderath, Markus Heiss, Franz Mayer, Marc Miserez, Agneta Montgomery, Salvador Morales-Conde, Filip Muysoms, Alexander Petter-Puchner, Rudolph Pointner, Neil Smart, Marciej Smietanski, Bernd Stechemesser.
Aim
The BioMesh Study Group has set itself the task of identifying how best to use biological meshes for the various indications. The first step toward achieving that goal is to compile systematic reviews of the different indications on the basis of the existing literature. The available literature sources will be evaluated in accordance with the Oxford Centre for Evidence-based Medicine-Levels of Evidence (March 2009). Next, based on the review findings, corresponding Statements and Recommendations are to be formulated in a Consensus Conference for the use of biological meshes for the different indications. The findings of this study were presented at the Consensus Conference in Berlin in January 2016 as a part of the project undertaken by the BioMesh Study Group. The findings of the Consensus Conference are currently being summarized for a joint publication.
Keywords: perineal hernia, abdominoperineal excision, biologic mesh, biosynthetic mesh
Citation: Narang SK, Alam NN, Köckerling F, Daniels IR and Smart NJ (2016) Repair of Perineal Hernia Following Abdominoperineal Excision with Biological Mesh: A Systematic Review. Front. Surg. 3:49. doi: 10.3389/fsurg.2016.00049
Received: 04 July 2016; Accepted: 22 August 2016;
Published: 05 September 2016
Edited by:
Hakan Kulacoglu, Recep Tayyip Erdoğan University, TurkeyReviewed by:
Gabriel Sandblom, Karolinska Institutet, SwedenUlf Gunnarsson, Umeå University, Sweden
Juan Manuel Suárez-Grau, Riotinto Hospital and Clinic QUIRON Sagrado Corazon, Spain
Copyright: © 2016 Narang, Alam, Köckerling, Daniels and Smart. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Neil J. Smart, drneilsmart@hotmail.com