 Michael Stadler*
Michael Stadler* Letizia VenturiniIvonne BüntingElke Dammann
Letizia VenturiniIvonne BüntingElke Dammann Eva M. WeissingerAdrian Schwarzer
Eva M. WeissingerAdrian Schwarzer Christian Schultze-FloreySteve EhrlichDominik MarkelCatherina LueckAlexandra GladyszTabea Fröhlich
Christian Schultze-FloreySteve EhrlichDominik MarkelCatherina LueckAlexandra GladyszTabea Fröhlich Nouraldin Damrah
Nouraldin Damrah Gernot BeutelMatthias Eder
Gernot BeutelMatthias Eder Arnold GanserLothar Hambach
Arnold GanserLothar Hambach- Department of Hematology, Hemostasis, Oncology, and Stem Cell Transplantation, Hannover Medical School, Hannover, Germany
Preemptive and therapeutic donor lymphocyte infusions (preDLI and tDLI) are widely used in relapsing and relapsed hematopoietic malignancies after allogeneic stem cell transplantation (alloSCT) to enhance the graft-versus-malignancy effect. However, in advanced myeloid malignancies, long-term survival after preDLI and tDLI remains low, reflecting our inability to master the double-edged sword of alloreactivity, balancing anti-neoplastic activity versus graft-versus-host disease (GvHD). We previously evaluated a quantitative PCR-based high-sensitivity chimerism (hs-chimerism) based on insertion/deletion polymorphisms instead of short tandem repeats, where increasing host chimerism in peripheral blood predicts relapse more than a month before clinical diagnosis, and declining host chimerism signals anti-host alloreactivity. Here we report 32 consecutive patients with advanced myeloid malignancies receiving preDLI or tDLI “navigated” by hs-chimerism (“navigated DLI”). We compared them to a historical cohort of 110 consecutive preDLI or tDLI recipients, prior to implementation of hs-chimerism at our institution (“controls”). Both groups were comparable regarding age, gender, conditioning, donor type, and time to DLI. With longer median follow-up of the navigated DLI group (8.5 versus 5 months), their landmark overall (64%) and disease-free survival (62%) at 2 years from first DLI compared favorably with controls (23% and 21%, respectively). Improved survival of navigated DLI was due to both reduced relapse incidence (38% versus 60%) and non-relapse mortality (17% versus 44%) at 2 years. Early relapse prediction by hs-chimerism allowed a preemptive approach in 28% of navigated DLI versus 7% in controls. Our results confirm hs-chimerism as a highly valuable tool for monitoring and steering immune interventions after alloSCT.
Introduction
Alloreactivity induced by allogeneic stem cell transplantation (alloSCT) currently represents the strongest weapon against aggressive hematologic malignancies (1–3). However, a substantial number of patents still succumb to the underlying disease, despite many efforts pre and post-transplant to reduce relapse rate (4, 5). For patients with impending or overt relapse after alloSCT, augmenting alloreactivity is required, either by donor lymphocyte infusions (DLI) (6) or through second transplantation, apart from cytoreduction as needed. Unfortunately, both cell based approaches yield only limited success, with long term survival rates in advanced myeloid malignancies below 20% (7). Currently, we seem unable to precisely “dose” anti-host immune cells in order to control the deleterious effects of either too little or too much alloreactivity, i.e., subsequent relapse or severe graft-versus-host disease (GvHD) (8).
One prerequisite to steering alloreactivity is accurate, reliable, rapid, and affordable measurement of recipient/donor chimerism. For aggressive malignancies with high relapse dynamics, conventional chimerism techniques based on short tandem repeats (9) have been found not sensitive enough to detect impending relapse in useful time (10, 11). Next-generation sequencing approaches for minimal residual disease detection, on the other hand, are time-consuming, expensive and limited to previously identified disease markers which may even be lost during disease progression. We have recently evaluated and implemented a quantitative PCR-based high-sensitivity chimerism method (hs-chimerism) based on insertion/deletion polymorphism markers, which is applicable to more than 90% of recipient/donor pairs (12). With a sensitivity of 0.01%, this method allows prediction of relapse in whole blood samples more than a month in advance compared to conventional chimerism methods with sensitivities around 1%. Relapse is predicted by consistently increasing recipient signals over time, while declining recipient chimerism, e.g. when tapering immunosuppression or during GvHD, heralds anti-host alloreactivity. With a turn-over time of only one to two days and moderate cost, we are using this method for monitoring and guiding the post-transplant follow-up of our patients with aggressive malignancies.
Here, we report outcome data from our first 32 consecutive patients receiving preemptive DLI (preDLI, for impending relapse) or therapeutic DLI (tDLI, for established relapse) “navigated” by aid of hs-chimerism (navigated DLI), in comparison to a historical cohort of 110 consecutive recipients of preDLI or tDLI for advanced myeloid neoplasms, prior to implementation of hs-chimerism at our institution (controls).
Patients and methods
Design
This is a single center study of a prospective, non-randomized cohort with a historical control group.
Patient cohorts
From 2016 to 2018, we validated and implemented a quantitative PCR-based, high-sensitivity chimerism method (hs-chimerism) using insertion/deletion polymorphism markers (12) instead of the short tandem repeat chimerism used previously at our institution. To evaluate the feasibility and efficacy of hs-chimerism in steering preDLI and tDLI, starting from 2019 we monitored all consecutive patients allotransplanted for advanced myeloid malignancies in whom the decisions on timing (initiating or delaying) of preDLI or tDLI were guided by hs-chimerism (“navigated DLI” group). All navigated DLI were performed from 2019 through 2021; data lock was December 31, 2021. For comparison, we choose all consecutive patients allotransplanted for advanced myeloid malignancies with preDLI and tDLI from 2001 to 2015 (“control group”). Patients’ characteristics are detailed in Table 1. Patients with preDLI and tDLI between 2016 and 2018 were excluded to avoid overlap with samples used for validation of hs-chimerism. (In addition to the navigated DLI group, 133 further patients with advanced myeloid malignancies were assessed by hs-chimerism between 2019 and 2021, but lacked significant increases in host chimerism and did not receive any DLI. Their characteristics are shown in the Supplementary Table). Data evaluation was in accordance with the declaration of Helsinki and amendments. All patients had given written informed consent to treatment, data analysis and publication prior to transplantation.
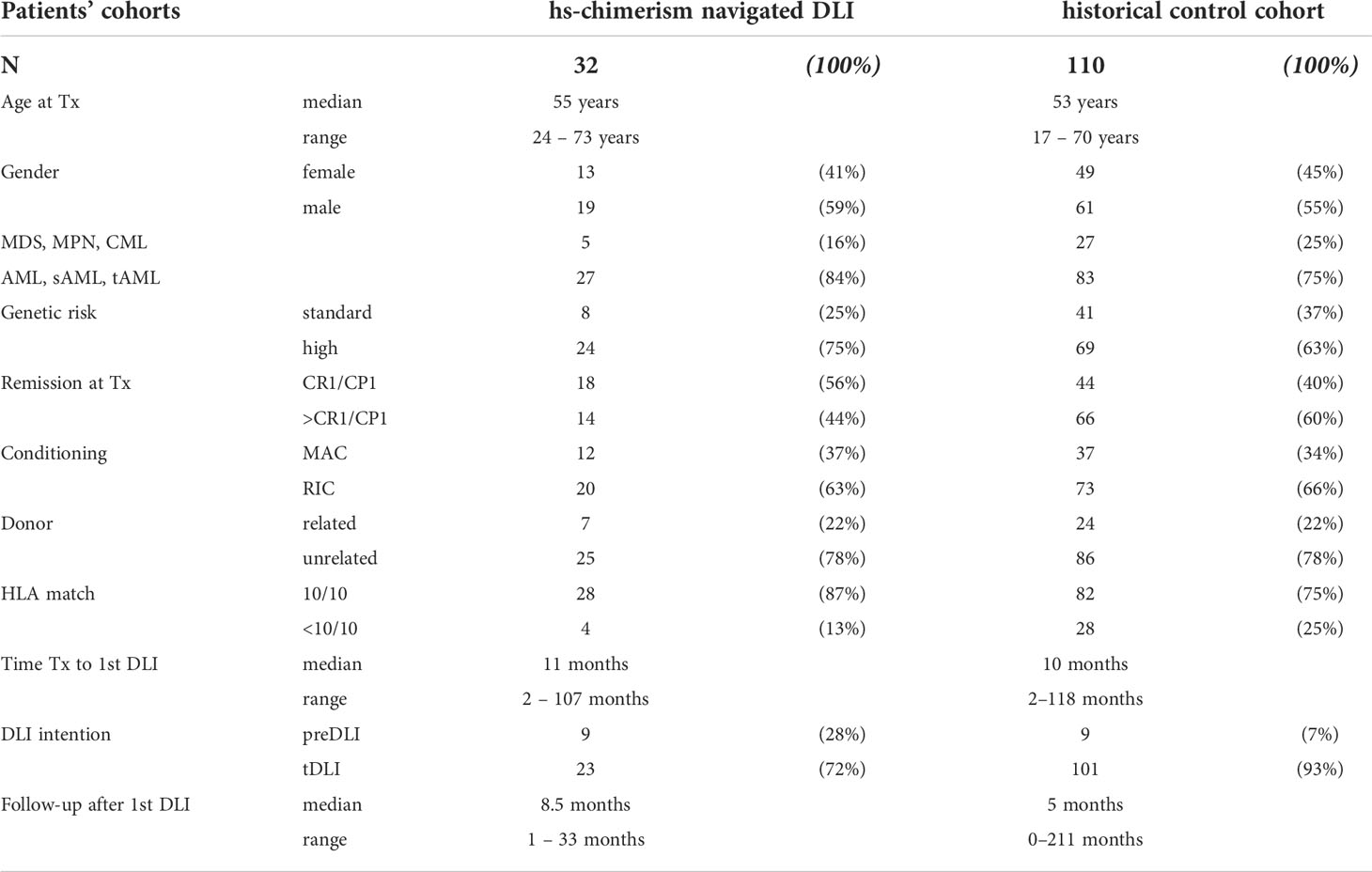
Table 1 Patients’ cohorts hs-chimerism navigated DLI historical control cohort.
hs-chimerism
Detailed procedures for hs-chimerism have previously been published (12, 13). Briefly, the method is based on human biallelic insertion/deletion polymorphism markers informative for recipient/donor genotype discrimination. Standard curves were created by subjecting serial dilutions of mixed DNA to real-time quantitative PCR. In the linear range, sensitivity was 0.01% (1 in 10.000). For individual hs-chimerism measurements, 300 ng of genomic DNA from patients’ whole blood were analyzed.
Treatments
Treatment strategy was the same in both groups. Chimerism analyses were performed monthly during the first year after alloSCT and gradually reduced to once yearly after five years, except for situations of rising host chimerism as well as after DLI, when chimerism was measured more frequently. Chimerism assessment guided both adaptation of immunosuppression and DLI application. preDLI were performed for impending relapse, as detected by chimerism, cytogenetic or molecular diagnostics, but still with less than 5% bone marrow blasts. tDLI were carried out for overt relapse, mostly after cytoreductive treatment (chemotherapy, hypomethylating agents, targeted molecular therapies, as appropriate and available). Immunosuppression was off or stopped before DLI. Unstimulated donor peripheral blood leukaphereses were performed without in vitro manipulation. DLI were started at a dose of 1 x 10E7 CD3 positive donor cells per kg recipient’s body weight, and escalated in half-logarithmic steps by at least monthly intervals, unless precluded by symptoms or signs of incipient GvHD. In the navigated DLI group, declining host chimerism in serial measurements triggered delay or suspension of subsequent DLI in order to prevent unnecessary excess GvHD. First DLI doses were usually administered freshly after leukapheresis. Aliquots of donor lymphocytes were cryopreserved and thawed immediately prior to subsequent DLI. Premedication consisted of antihistamines, but no steroids. After DLI administration, patients were monitored by outpatient clinical visits every two weeks until further DLI, GvHD, disease remission, or progression.
Statistics
Survival curves were calculated and drawn according to the method of Kaplan & Meier (14). Primary (overall survival) and secondary endpoints (disease-free survival, relapse incidence, non-relapse mortality, GvHD) were evaluated in landmark analyses from the day of first DLI. Due to the design of this study with a historical control cohort, and small numbers in the navigated DLI group, we refrained from calculations of significance and uni- or multivariate analyses, in favor of only descriptive and graphical comparisons between the cohorts.
Results
To evaluate the feasibility of hs-chimerism in guiding DLI, we collected all 32 consecutive transplant recipients for advanced myeloid malignancies with preDLI or tDLI from 2019 until 2021 based on individual hs-chimerism results (“navigated DLI”). For comparison, all respective 110 consecutive patients with preDLI or tDLI from 2001 to 2015, prior to the implementation of hs-chimerism, served as a historical control cohort. (133 additional patients with advanced myeloid malignancies were monitored by hs-chimerism between 2019 and 2021, but without significant increases in host chimerism and without DLI.)
Patients’ characteristics
Patients’ characteristics are detailed in Table 1. Both cohorts were well matched with respect to age, gender, conditioning intensity, donor type, and time from alloSCT to first DLI. Differences included more patients with aggressive diseases (AML/sAML/tAML; 84% versus 75%) and with high cytogenetic or molecular risk (75% versus 63%) for the navigated DLI group. On the other hand, fewer patients in the control cohort had reached complete remission (CR) before alloSCT (40% versus 56%) or had a fully matched donor (75% versus 87%).
(2019 – 2021 hs-chimerism patients without DLI were well matched with those of the navigated group, except for an even higher proportion of patients with adverse risk genetics: 85% versus 75%; see Supplementary Table).
hs-chimerism patterns with DLI
Examples of individual hs-chimerism results from representative patients with navigated DLI for acute myeloid leukemia (AML), myelodysplastic syndrome (MDS), myeloproliferative neoplasia (MPN), and chronic myeloid leukemia (CML) are shown in Figure 1. In diseases with low relapse dynamics, the initial increase in host chimerism appeared protracted (Figures 1B–D). Decrease of host chimerism was rather slow with relapse pharmacotherapy (e.g. hypomethylating agents), but mostly precipitous after one or more DLI. Note in Figure 1A that decreasing host chimerism obviated application of subsequent DLI, even prior to clinical symptoms and signs of GvHD, thus sparing excess toxicity. DLI-induced anti-host alloreactivity cleared relapses at the cytogenetic and molecular levels (Figures 1B–D), and was not always associated with GvHD (Figures 1B, C).
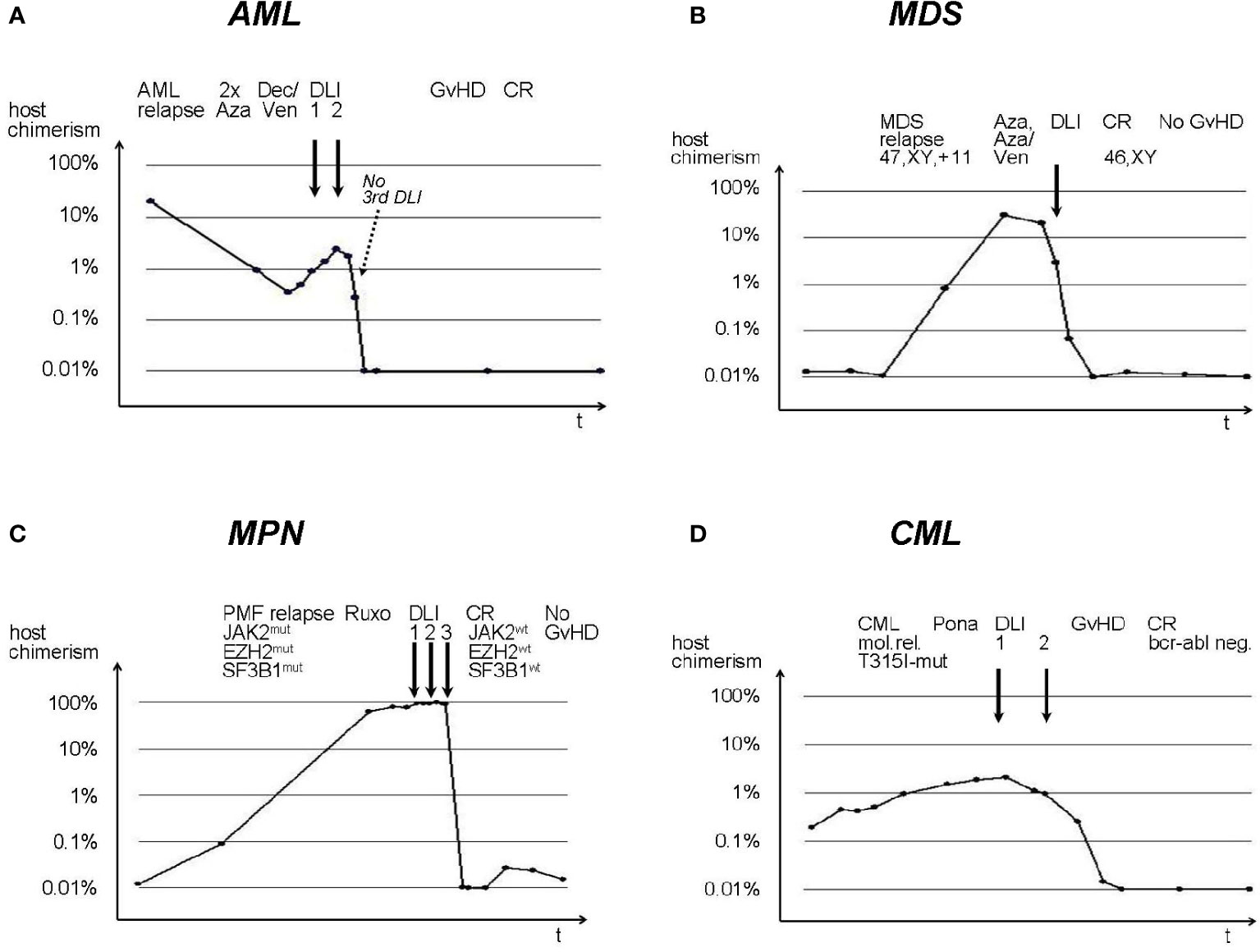
Figure 1 Individual hs-chimerism sequences in AML, MDS, MPN, and CML patients with navigated DLI. (A) AML, (B) MDS, (C) MPN, (D) CML. DLI are indicated by solid arrows. Aza, Azacytidine; Ven, Venetoclax; PMF, Primary Myelofibrosis; Ruxo, Ruxolitinib; Pona, Ponatinib; mut, mutation; wt, wild type. y-axes: host chimerism; x-axes: time after alloSCT.
Follow-up
According to the study design, the range of follow-up after first DLI was much longer in the control cohort, starting as early as 2001 (211 months versus 33 months). However, the median follow-up after first DLI was longer in the navigated DLI group (8.5 months versus 5 months), already suggesting superior outcome.
Outcome
Landmark overall (OS) and disease-free survival (DFS) from first DLI are shown in Figures 2A–D. Whereas 2-year-OS and -DFS in the control cohort (23% and 21%, respectively) were well comparable with results from earlier studies (7), 2-year-OS and -DFS of the navigated DLI group reached 64% and 62%, respectively. This was due to improvements in both relapse incidence after first DLI (RI) with 2-year-RI for navigated DLI at 38% versus 60% for controls (Figures 2E, F) and non-relapse-mortality after DLI (NRM) with 2-year-NRM in the navigated DLI group at 17% versus 44% for the control cohort (Figures 2G, H). Accordingly, both overall GvHD (Figures 2I, J; navigated DLI 67% versus controls 83%) and significant GvHD (acute GvHD °III–°IV or chronic extensive GvHD; Figures 2K, L) at 2 years from first DLI favored the navigated DLI group (44% versus 52% in the control cohort).
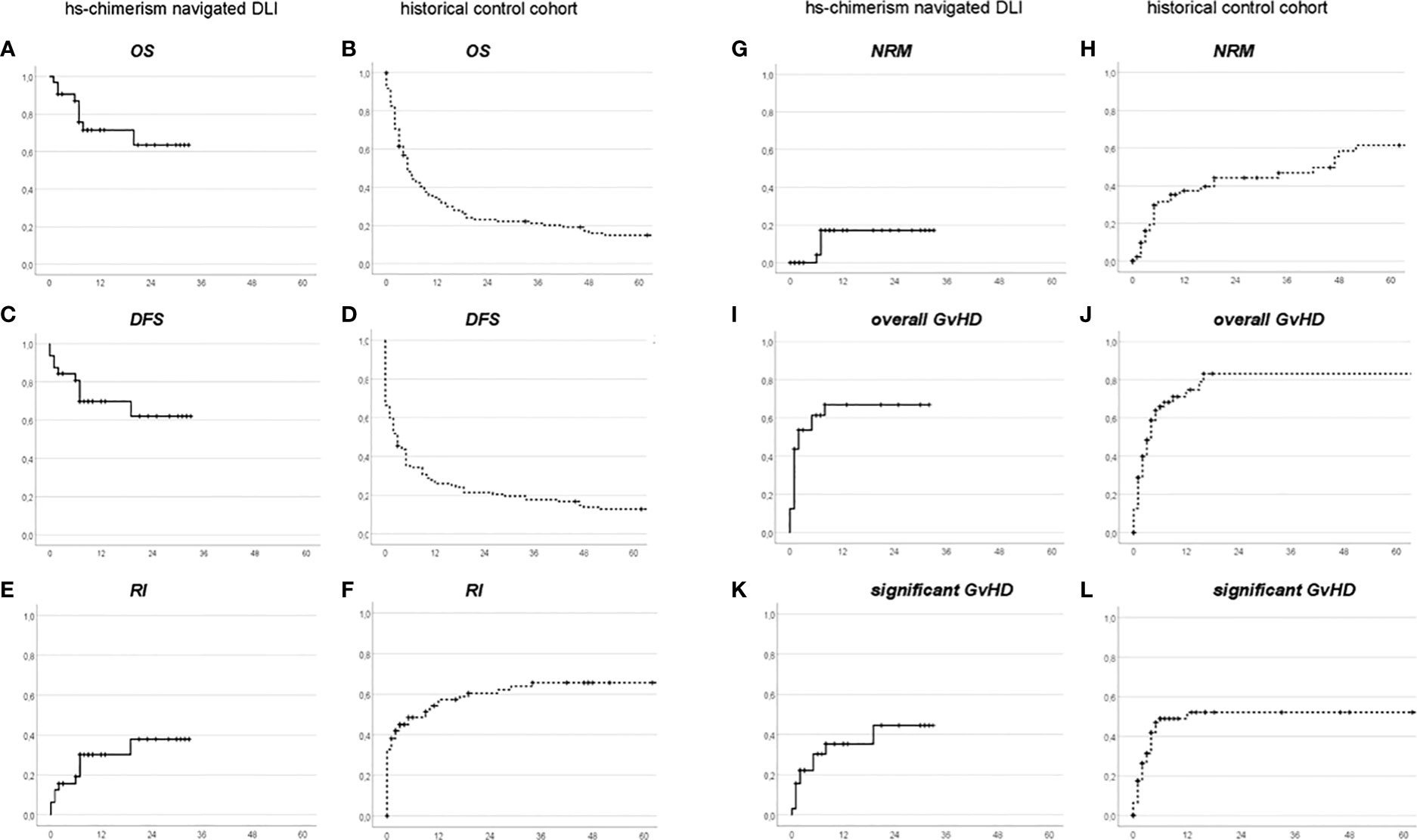
Figure 2 Landmark Overall Survival (A, B), Disease-Free Survival (C, D), Relapse Incidence (E, F), Non-Relapse Mortality (G, H), overall GvHD (I, J), and significant GvHD (K, L), from first DLI, in the hs-chimerism navigated group (A, C, E, G, I, K) or the historical control group (B, D, F, H, J, L), respectively. x-axes: months after first DLI.
(Outcomes at 2 years for the 2019 – 2021 hs-chimerism patients without DLI were: OS 91%, DFS 82%, RI 14%, NRM 5%, overall GvHD 75%, and significant GvHD 22%. Median follow-up was 14 (range, 2 to 33) months; see Supplementary Figure 1).
preDLI and tDLI
Outcome after preDLI appeared only moderately better in the navigated DLI group (2-year-OS 76% versus 67% in controls; Figures 3A, B), whereas in tDLI the difference was more pronounced (2-year-OS 60% in navigated DLI versus 19% in the control group; Figures 3C, D). This suggests that the main contribution to improvement by hs-chimerism occurred after established relapse. On the other hand, thanks to early relapse prediction, hs-chimerism enabled more often a preemptive approach (in 28% of navigated DLI versus 7% in controls) which by itself was associated with a better outcome. Thus, application of hs-chimerism resulted in a dual benefit “before and after” DLI.
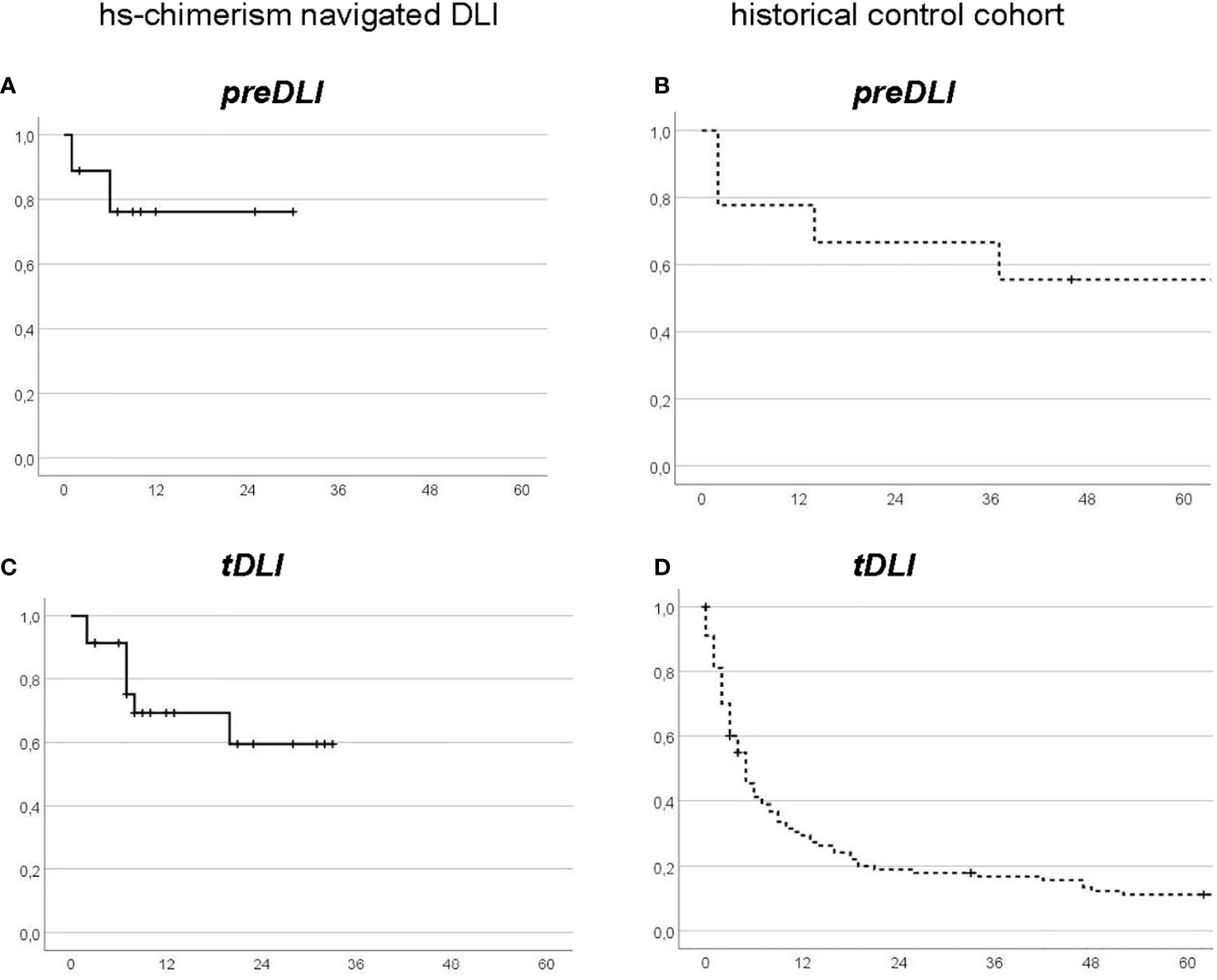
Figure 3 Landmark Overall Survival from first DLI, by DLI intention: preDLI (A, B) versus tDLI (C, D) in the hs-chimerism navigated group (A, C) or the historical control group (B, D), respectively. x-axes: months after first DLI.
Discussion
Our data suggest that navigating preDLI and tDLI using hs-chimerism substantially improved outcomes, for both the individual patient and the whole cohort. Due to its high sensitivity, accuracy, reliability, rapid turnover, and moderate cost, this method enabled close monitoring of subsequent steps for relapse prevention and therapy timelier. This allowed us to modify therapeutic strategies prior to clinically relevant problems, e.g. to forgo additional DLI when host chimerism started to decline in order to reduce GvHD toxicity, or to schedule refractory patients for second alloSCT at an earlier time-point. For the navigated DLI group, steering of DLI by hs-chimerism paid off with consistently reduced relapse incidence, NRM, and GvHD, resulting in superior OS and DFS at 2 years from first DLI (almost tripled compared to our experience until 2015). The improvement through navigating by hs-chimerism was greatest in the tDLI setting, whereas preDLI patients had the benefit of early relapse prediction enabling a preemptive approach leading to already better outcome.
A clinical benefit of hs-chimerism monitoring was also obvious in the 133 patients with advanced myeloid malignancies not receiving DLI for lack of significant increases in host chimerism: with a median follow-up of 14 (range, 2 to 33) months, their outcome at 2 years was excellent with OS 91%, DFS 82%, RI 14%, and NRM 5% (Supplementary Figure 1), confirming our earlier observation of a very high negative predictive value (98-99% relapse exclusion) of the hs-chimerism (12), even in a cohort with substantial genetic risk (Supplementary Table). Interestingly, only 22% experienced significant GvHD despite an overall GvHD rate of 75%, suggesting that most of these patients had received just the right amount of mild GvL to prevent relapse.
Earlier studies on guiding preDLI by chimerism were hampered by limited sensitivity of conventional techniques and had focused on relapse prediction. Still, in pediatric leukemia patients, survival rates around 50% to 80% were reported for selected patients offered preDLI for increasing mixed chimerism (15, 16). In adults, preDLI for mixed chimerism detected by conventional or lineage specific chimerism analyses with sensitivities in the range of 1% or 0.1%, respectively, did not result in improved survival (17). However, a recent, large registry-based study on 192 patients receiving preDLI for minimal residual disease or mixed chimerism reported 51% and 63% OS, respectively, with no relapses beyond 3 years from first DLI (18).
Jacque et al. (11), using a high-sensitivity insertion/deletion chimerism quantitative real-time PCR technique, found lower relapse rates in patients offered immunomodulation for mixed chimerism (mostly tapering of immunosuppression), but lost both of their preDLI patients to acute GvHD °IV.
With regard to steering tDLI by chimerism analysis, we are unaware of any published studies.
Our analysis has several limitations:
First, a bias inherent to the design with a historical control cohort cannot be ruled out, although we undertook all efforts to minimize such bias by including all consecutive patients of the respective time periods into the cohorts.
Second, the size of the navigated DLI group is rather small, so individual outcomes might gain relatively more weight than in the larger control group (which, however, would apply for both favorable and unfavorable outcomes).
Third, the follow-up of the navigated group is still short. As can be seen from Figure 2H, there was a late increase beyond 3 years in NRM in the control cohort, probably as a consequence of chronic GvHD; a similar late increase cannot be excluded to occur in the future in the navigated DLI group as well (albeit less likely, due to the lower incidence of GvHD among navigated DLI patients). However, the median follow-up of the navigated DLI group already exceeded that of the control cohort at this time point, in line with superior outcome in the navigated DLI group.
Finally, with the control cohort originating in the remote past, there might be a bias through medical progress in favor of the more recent navigated group, e.g. based on more potent cytoreductive treatments before DLI. However, when splitting up the control cohort in half-decades (2001 to 2005: n = 42, 2006 to 2010: n = 31, 2011 to 2015: n = 37), 2-year-OS from first DLI remained at 28%, 17%, and 22%, respectively, with no progress over time to appreciate (Supplementary Figure 2). Furthermore, observing individual hs-chimerism data (Figures 1A–D), the effect of various therapies before DLI (azacytidine, decitabine, venetoclax, ruxolitinib, ponatinib) appeared rather small in comparison to the steep decline of host chimerism with alloreactivity. Venetoclax, the only drug not yet in use for myeloid relapse up to 2015, which therefore might have caused a bias between the navigated and control cohorts, did not change this pattern and was employed in less than half of the navigated group for cytoreduction prior to DLI. Thus, while a contribution of adjunctive medical therapies cannot be entirely ruled out, it would not be sufficient to explain the substantial outcome improvement observed with navigated DLI.
Taken together, hs-chimerism has proven a highly valuable tool for monitoring and steering immune interventions after alloSCT and deserves further evaluation and development.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
Concept, design, and manuscript draft: MS. hs-chimerism: LV, IB, and LH. Patient care: MS, LH, AS, CS-F, SE, DM, CL, AGl, TF, ND, EMW, GB, ME, and AGa. Manuscript editing: LH, EMW, CS-F, CL, and ME. All authors contributed to the article and approved the submitted version.
Acknowledgments
We thank Susanne Luther-Wolf for technical assistance with DNA preparation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2022.867356/full#supplementary-material
References
1. Kolb HJ. Graft-versus-leukemia effects of transplantation and donor lymphocytes. Blood (2008) 112:4371–83. doi: 10.1182/blood-2008-03-077974
2. Sweeney C, Vyas P. The graft-versus-leukemia effect in AML. Front Oncol (2019) 9:1217. doi: 10.3389/fonc.2019.01217
3. Kunadt D, Stölzel F. Effective immunosurveillance after allogeneic hematopoieticstem cell transplantation in acute myeloid leukemia. Cancer Manag Res (2021) 13:7411–27. doi: 10.2147/CMAR.S261721
4. Lee CJ, Savani BN, Mohty M, Gorin NC, Labopin M, Ruggeri A, et al. Post-remission strategies for the prevention of relapse following allogeneic hematopoietic cell transplantation for high-risk acute myeloid leukemia: expert review from the acute leukemia working party of the EBMT. Bone Marrow Transplant (2019) 54:519–30. doi: 10.1038/s41409-018-0286-2
5. Webster JA, Luznik L, Gojo I. Treatment of AML relapse after allo-HCT. Front Oncol (2021) 11:812207. doi: 10.3389/fonc.2021.812207
6. Schmid C, Kuball J, Bug G. Defining the role of donor lymphocyte infusion in high-risk hematologic malignancies. J Clin Oncol (2021) 39:397–418. doi: 10.1200/JCO.20.01719
7. Kharfan-Dabaja MA, Labopin M, Polge E, Nishihori T, Bazarbachi A, Finke J, et al. Association of second allogeneic hematopoietic cell transplant vs donor lymphocyte infusion with overall survival in patients with acute myeloid leukemia relapse. JAMA Oncol (2018) 4:1245–53. doi: 10.1001/jamaoncol.2018.2091
8. Deeg HJ. Chimerism, the microenvironment and control of leukemia. Front Oncol (2021) 12:652105. doi: 10.3389/fonc.2021.652105
9. Navarro-Bailón A, Carbonell D, Escudero A, Chicano M, Muniz P, Suárez-González J, et al. Short tandem repeats (STRs) as biomarkers for the quantitative follow-up of chimerism after stem cell transplantation: methodological considerations and clinical application. Genes (2020) 11:993. doi: 10.3390/genes11090993
10. Koldehoff M, Steckel NK, Hlinka M, Belen DW, Elmaagacli AH. Quantitative analysis of chimerism after allogeneic stem cell transplantation by real-time PCR with single nucleotide polymorphisms, standard tandem repeats, and y-chromosome-specific sequences. Am J Hematol (2006) 81:735–46. doi: 10.1002/ajh.20693
11. Jacque N, Nguyen S, Golmard J-L, Uzunov M, Garnier A, Leblond V, et al. Chimerism analysis in peripheral blood using indel quantitative real-time PCR is a useful tool to predict post-transplant relapse in acute leukemia. Bone Marrow Transplant (2015) 50:259–65. doi: 10.1038/bmt.2014.254
12. Sellmann L, Rabe K, Bünting I, Dammann E, Göhring G, Ganser A, et al. Diagnostic value of highly-sensitive chimerism analysis after allogeneic stem cell transplantation. Bone Marrow Transplant (2018) 53:1457–65. doi: 10.1038/s41409-018-0176-7
13. Alizadeh M, Bernard M, Danic B, Dauriac C, Birebent B, Lapart C, et al. Quantitative assessment of hematopoietic chimerism after bone marrow transplantation by real-time quantitative polymerase chain reaction. Blood (2002) 99:4618–25. doi: 10.1182/blood.V99.12.4618
14. Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc (1958) 53:457–81. doi: 10.1080/01621459.1958.10501452
15. Rettinger E, Willasch AM, Kreyenberg H, Borkhardt A, Holter W, Kremens B, et al. Preemptive immunotherapy in childhood acute myeloid leukemia for patients showing evidence of mixed chimerism after allogeneic stem cell transplantation. Blood (2011) 118:5681–8. doi: 10.1182/blood-2011-04-348805
16. Ruijkijyanont P, Morris C, Kang G, Gan K, Hartford C, Triplett B, et al. Risk-adapted donor lymphocyte infusion based on chimerism and donor source in pediatric leukemia. Blood Cancer J (2013) 3:e137. doi: 10.1038/bcj.2013.39
17. Zeiser R, Spyridonidis A, Wäsch R, Ihorst G, Grüllich C, Bertz H, et al. Evaluation of immunomodulatory treatment based on conventional and lineage-specific chimerism analysis in patients with myeloid malignancies after myeloablative allogeneic hematopoietic cell transplantation. Leukemia (2005) 19:814–21. doi: 10.1038/sj.leu.2403719
Keywords: Donor lymphocyte infusion, chimerism, allogeneic stem cell transplantation, alloreactivity, graft-versus-leukemia, graft-versus-host
Citation: Stadler M, Venturini L, Bünting I, Dammann E, Weissinger EM, Schwarzer A, Schultze-Florey C, Ehrlich S, Markel D, Lueck C, Gladysz A, Fröhlich T, Damrah N, Beutel G, Eder M, Ganser A and Hambach L (2022) Navigating preemptive and therapeutic donor lymphocyte infusions in advanced myeloid malignancies by high-sensitivity chimerism analysis. Front. Oncol. 12:867356. doi: 10.3389/fonc.2022.867356
Received: 01 February 2022; Accepted: 05 July 2022;
Published: 17 August 2022.
Edited by:
Alison Loren, University of Pennsylvania, United StatesReviewed by:
Michael Richard Grunwald, Levine Cancer Institute, United StatesIsmael Buño, Instituto de Investigación Sanitaria Gregorio Marañón, Spain
Copyright © 2022 Stadler, Venturini, Bünting, Dammann, Weissinger, Schwarzer, Schultze-Florey, Ehrlich, Markel, Lueck, Gladysz, Fröhlich, Damrah, Beutel, Eder, Ganser and Hambach. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michael Stadler, stadler.michael@mh-hannover.de