 Cecilia Smith Simonsen1,2,3*
Cecilia Smith Simonsen1,2,3* Heidi Øyen Flemmen4,5Line Broch1,2,3Cathrine Brunborg6Pål Berg-Hansen2Stine Marit Moen7
Heidi Øyen Flemmen4,5Line Broch1,2,3Cathrine Brunborg6Pål Berg-Hansen2Stine Marit Moen7 Elisabeth Gulowsen Celius2,3
Elisabeth Gulowsen Celius2,3- 1Department of Neurology, Vestre Viken Hospital Trust, Drammen, Norway
- 2Department of Neurology, Oslo University Hospital, Oslo, Norway
- 3Institute of Clinical Medicine, University of Oslo, Oslo, Norway
- 4Department of Neurology, Telemark Hospital Trust, Skien, Norway
- 5Institute of Health and Society, University of Oslo, Oslo, Norway
- 6Oslo Centre for Biostatistics and Epidemiology, Research Support Services, Oslo University Hospital, Oslo, Norway
- 7Multiple Sclerosis Centre Hakadal, Grønvoll, Norway
Background: Moderate and high efficacy disease modifying therapies (DMTs) have a profound effect on disease activity. The current treatment guidelines only recommend high efficacy DMTs for patients with highly active MS. The objective was to examine the impact of initial treatment choice in achieving no evidence of disease activity (NEDA) at year 1 and 2.
Methods: Using a real-world population-based registry with limited selection bias from the southeast of Norway, we determined how many patients achieved NEDA on moderate and high efficacy DMTs.
Results: 68.0% of patients who started a high efficacy DMT as the first drug achieved NEDA at year 1 and 52.4% at year 2 as compared to 36.0 and 19.4% of patients who started a moderate efficacy DMT as a first drug. The odds ratio (OR) of achieving NEDA on high efficacy drugs compared to moderate efficacy drugs as a first drug at year 1 was 3.9 (95% CI 2.4–6.1, p < 0.001). The OR for high efficacy DMT as the second drug was 2.5 (95% CI 1.7–3.9, p < 0.001), and was not significant for the third drug. Patients with a medium or high risk of disease activity were significantly more likely to achieve NEDA on a high efficacy therapy as a first drug compared to moderate efficacy therapy as a first drug.
Conclusions: Achieving NEDA at year 1 and 2 is significantly more likely in patients on high-efficacy disease modifying therapies than on moderate efficacy therapies, and the first choice of treatment is the most important. The immunomodulatory treatment guidelines should be updated to ensure early, high efficacy therapy for the majority of patients diagnosed with MS.
Introduction
Multiple sclerosis is a chronic neuroinflammatory disease with onset in mostly young people, and it is the commonest cause of serious physical disability in adults of working age (1). The condition may have a profound impact on quality of life and employment (2). Interferon as a treatment for multiple sclerosis (MS) was first approved in 1996 (3). In 2006, natalizumab was approved as the first high efficacy disease modifying therapy (DMTs) (4), and in the following years more DMTs followed suit. The therapies are divided into moderate efficacy DMTs, with a well-defined safety profile, and high efficacy DMTs, which are more effective but carries higher risk of serious side effects (5). The current European and American treatment guidelines only advise the use of high efficacy drugs for highly active disease (6, 7). Time to EDSS 6 over the past two decades has increased (8). Although DMTs are not the only reason for this development (9), they likely play an important role (10). There are few head to head randomized clinical trials (RCT), so the importance of real-world evidence has been elevated (11).
The concept of “No Evidence of Disease Activity” (NEDA) has been identified as an ambitious tool for measuring efficacy of DMTs (12). NEDA at 1 year is achieved if there is no history of a clinical relapse, no new activity on magnetic resonance imaging (MRI) and no sign of clinical disease progression measured by expanded disability status scale (EDSS) in the past year (13). Although NEDA is by no means a perfect tool (14), limited disease activity in the first few years of diagnosis is widely regarded as a good prognostic sign (15).
The aim of this study was to determine how many patients in a Norwegian population-based real-world study achieved NEDA at 1 and 2 years and examine the impact of initial treatment choice in achieving NEDA.
Materials and Methods
Data Collection and Study Population
The BOT-MS (Buskerud, Oslo and Telemark) is a database comprising the complete population of MS patients in the two counties Buskerud and Telemark, and the majority of the patients in the Norwegian capital Oslo (n = 3,951). The data were recorded prospectively until 31.12.2017, but retrieved retrospectively by three neurologists specialized in MS between January and December 2018. Detailed information on the database and data collection has previously been published (9).
For this cohort study, we included all patients who had been treated with moderate efficacy DMTs (interferons, glatiramer acetate, teriflunomidem, and dimethyl-fumarate) and/or high efficacy DMTs (natalizumab, fingolimod, or alemtuzumab) for at least 12 months. All patients had access to all disease modifying drugs as all were available and reimbursed since market access in Europe (Table 1). The definition of moderate and high efficacy DMTs was chosen because at the time of market access, fingolimod was considered high efficacy and dimethyl-fumarate was considered moderate efficacy treatment (16). Consequently, that is how they were utilized in the follow-up period. We only included patients started on the treatment in 2006 or after, as 2006 was the first year our population had access to the first high efficacy drug, natalizumab. Only patients with yearly (±2 months) EDSS and MRI were included. Patients with missing or incomplete information and patients with incomplete information precluding determination of NEDA were excluded. For NEDA-status at year 1 we did not include those that discontinued due to side effects or wish for pregnancy, but we included the patients who discontinued the drug before the full 12 months due to lack of efficacy. For NEDA-status in year 2, we included any patient who had been on the drug for at least 24 months, including treatment interruption due to lack of efficacy, but not interruption due to side-effects and wish for pregnancy. The population was divided into three subgroups dependent on previous treatments: first drug, second drug or third drug. When looking at drugs previously used, we included all drugs the patient had taken for at least 3 months. Alemtuzumab was considered effective from the first treatment.
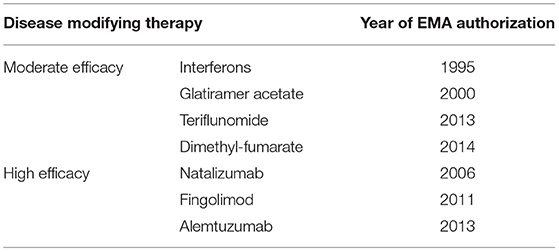
Table 1. Disease modifying therapies and year of European Medical Agency (EMA) approval (http://www.emsp.org/about-ms/ms-treatments/#).
We considered any new or enlarging lesions or new gadolinium enhancing lesions on follow-up brain MRI to represent MRI change. For EDSS, we considered any increase in EDSS on at least two consecutive occasions to represent a worsening of EDSS. Only EDSS documented 3 months or more after a relapse were included. Relapses documented in the patients' hospital records were counted as a relapse, regardless of steroid treatment. If we had a negative finding in one of the three components of NEDA, we considered the patient as NEDA fail even though we did not have one or two of the other components (EDSS, MRI and/or relapse).
We created a predictive variable for the future risk of disease activity based on our previous findings in this population (9) and known prognostic risk factors. Age (17–19), sex (17, 18, 20, 21), symptoms at onset (17, 22, 23), involvement of more than one Kurtzke functional system at onset (24), number of relapses within the first 2 years of onset (17, 21, 24–26), findings on a first MRI (20) and EDSS (27) were used, see Table 2. We graded the risk of disease activity based on seven categories of characteristics at the time of diagnosis that are believed to have an impact on future disease activity. Symptom at onset was defined by Kurtzke's functional system (28) and multiple symptoms at onset was defined as symptoms from two or more functional system. We divided the population into low risk for disease activity (0–3 points), medium risk (4–7), and high risk (8–14p). Based on seven categories, the population was divided into three risk groups: low risk for disease activity (1–3 points), medium risk (4–7), and high risk (8–14p). We did not include spinal cord lesions or gadolinium enhancing lesions as this is not done routinely in the clinical practice.
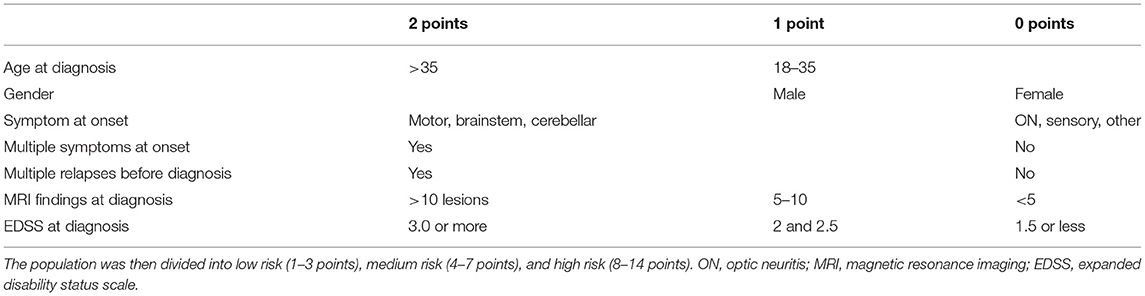
Table 2. The risk of disease activity at the time of diagnosis was calculated according to these seven factors.
The first generation drugs are referred to as injectables (interferon, glatiramer acetate) and were used as a reference category in calculations of odds ratio. Age was dichotomous in the age category with “old” (≥40 years at time of drug initiation) and “young” (<40 years). To investigate the impact of possible changes in prescription practice, and to correct for missing patients, we split the groups into those patients initiated before 2013, and those initiated after 2013. The year 2013 was chosen as this was when teriflunomide, the first oral moderate efficacy drug, became available.
Statistics
We used IBM SPSS Statistics 25.0 (IBM Corp., Armonk, NY, USA) for data analysis. Differences in continuous variables between two groups were assessed by independent sample t-test. Between groups, differences in continuous variables were tested with Student t-test for normally distributed data and Mann-Whitney U-test for skewed data. The chi-square-test for contingency tables was used to detect associations between categorical variables. Binary logistic regression analysis was used to investigate the association between the treatments and NEDA, and to adjust for possible confounding effects of sex, age at start of medication, time from onset to start of medication and risk group (low, medium and high risk). The results from the regression analysis are presented as odds ratio, adjusted and unadjusted, with 95% confidence intervals (CI). All p-values were two-sided and a 5% significance level was used.
Ethics
This study was approved by the Regional Ethics Committee in Norway (REK 2015/670). One of the conditions for approval was that strict privacy concerns were respected, and that data was not made publicly available. Specific requests regarding data sharing should be directed to the corresponding author.
Results
We included 694 patients with a total of 1,146 drug initiations; demographics are shown in Table 3 and drug swaps are illustrated in Figure 1. Of the patients who started a high efficacy DMT as the first drug, 68.0% achieved NEDA at year 1 and 52.4% achieved NEDA at year 2. Conversely, 36.0% of patients who started a moderate efficacy DMT as a first drug achieved NEDA in year 1 and 19.4% in year 2 (Table 4). The superior effect of high efficacy vs. moderate efficacy DMT on NEDA was highly significant (p < 0.001) at both year 1 and 2.
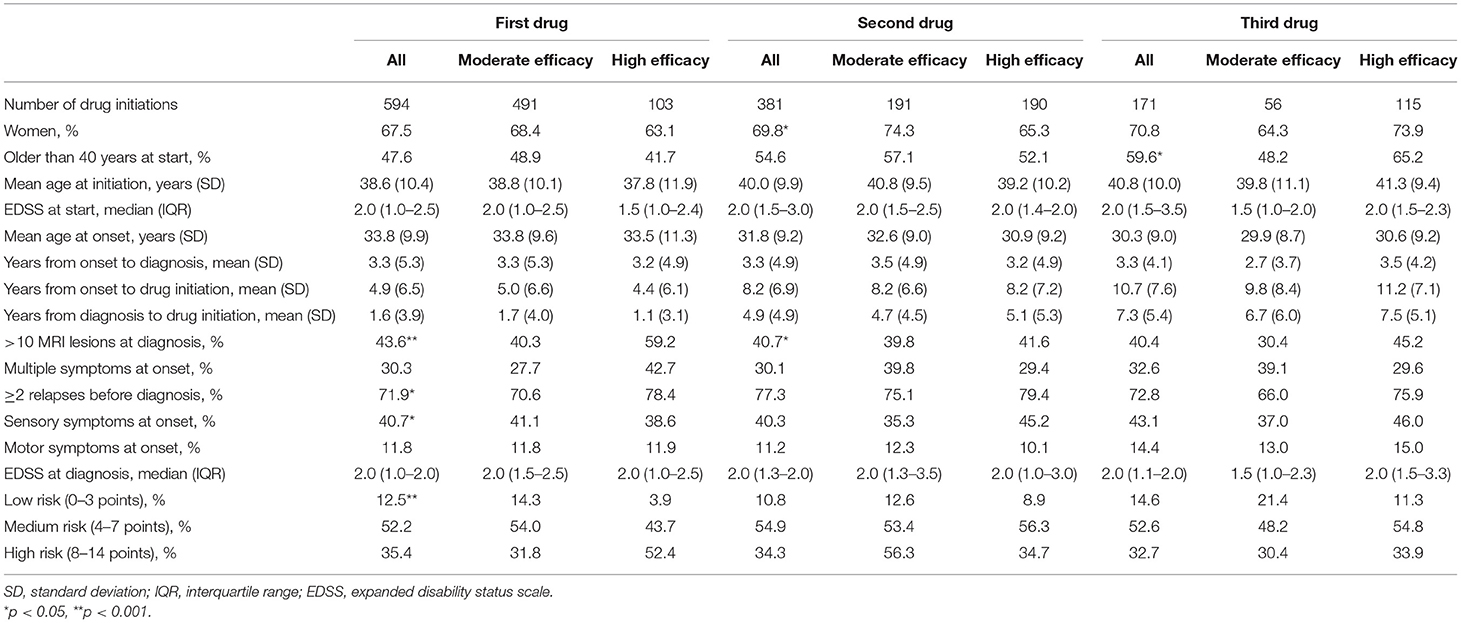
Table 3. Demographics of study population.
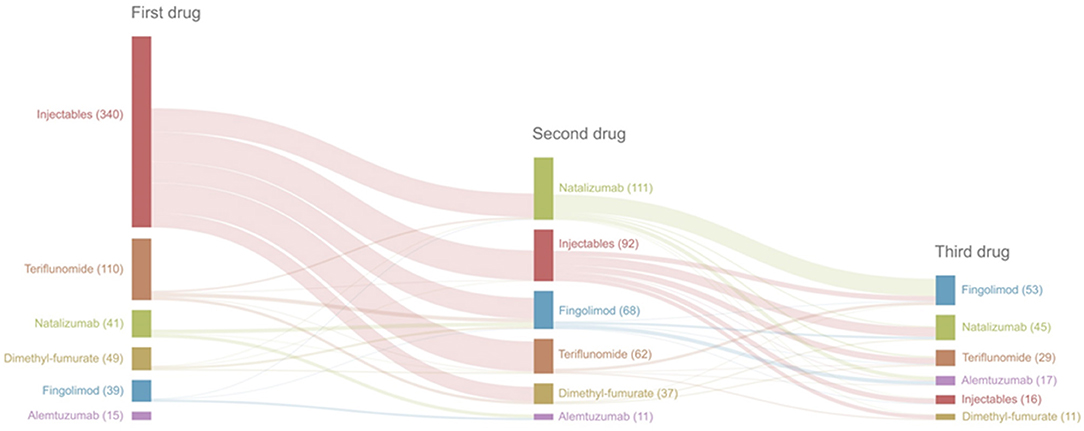
Figure 1. Flow chart of drug swaps.
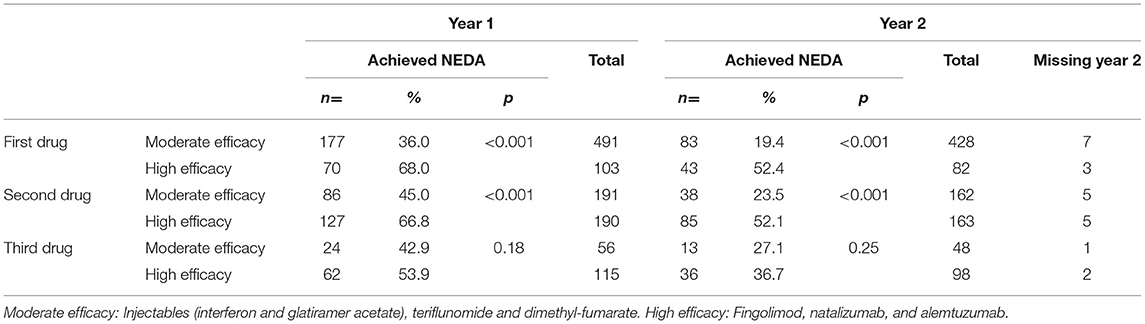
Table 4. NEDA year 1 and NEDA year 2.
The odds ratio of achieving NEDA on a high efficacy DMT as first drug at year 1 was 3.9 (95% CI 2.4–6.1, p < 0.001) and at year 2 was 4.6 (96% CI 2.8–7.6, p < 0.001) compared to moderate efficacy DMTs (Table 5). The odds ratio did not change meaningfully after adjusting for sex, age at start of medication and time from onset to start of medication. The difference in the proportion of patients achieving NEDA on high efficacy drugs and the odds ratio of achieving NEDA were lower for the second drug, but still highly significant (p < 0.001). There was no significant difference for the third drug (Tables 4, 5).
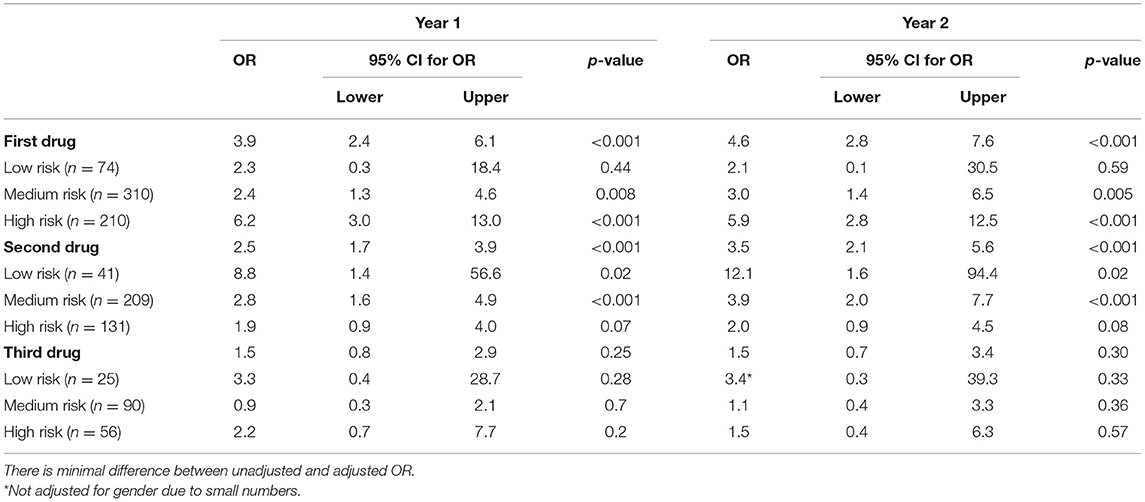
Table 5. Odds ratio (OR) analyzed by binary logistics for NEDA year 1 and 2 in high efficacy DMT vs. moderate efficacy DMT, stratified by risk and adjusted for age at initiation of medication, time from onset to initiation of drug and sex.
We also looked at moderate and high efficacy drug initiations before and after 2013 (data not shown), and the findings remained largely unchanged. One exception is that the odds ratio adjusted for initiation before and after 2013 for the second drug increased from 2.5 (95% CI 1.66–3.9, p < 0.001) to 3.1 (95% CI 2.0–4.9, p < 0.001).
Age did not have a notable impact on the proportion achieving NEDA on the first drug. The proportion of older patients achieving NEDA on a moderate efficacy drug as the second drug was lower than younger patients (37.8 vs. 50.5%), but this was not significant (p = 0.08). As a third drug, however, there was a significant difference between moderate and high efficacy drugs in the younger population (72.6 vs. 62.5%, p = 0.004), but there was no significant difference in the older age group (Supplementary Tables 1, 2).
Table 6 shows the demographic observations of those who achieved NEDA vs. those who did not achieve NEDA on moderate and high efficacy drugs in the three subgroups. Patients who achieved NEDA on moderate efficacy DMTs were in general slightly older, had longer time from onset to diagnosis and from onset to initiation of treatment. In contrast, this finding tended to be reversed in patients on high efficacy therapies who achieved NEDA. Patients with a medium or high risk of disease activity (87.6% of patients on a first drug, 89.2% of patients on a second drug and 85.3% of patients on a third drug) were significantly more likely to achieve NEDA on a high efficacy therapy as a first drug. There was no significant difference in patients on moderate efficacy therapy, or any second or third drug, regardless of potency.
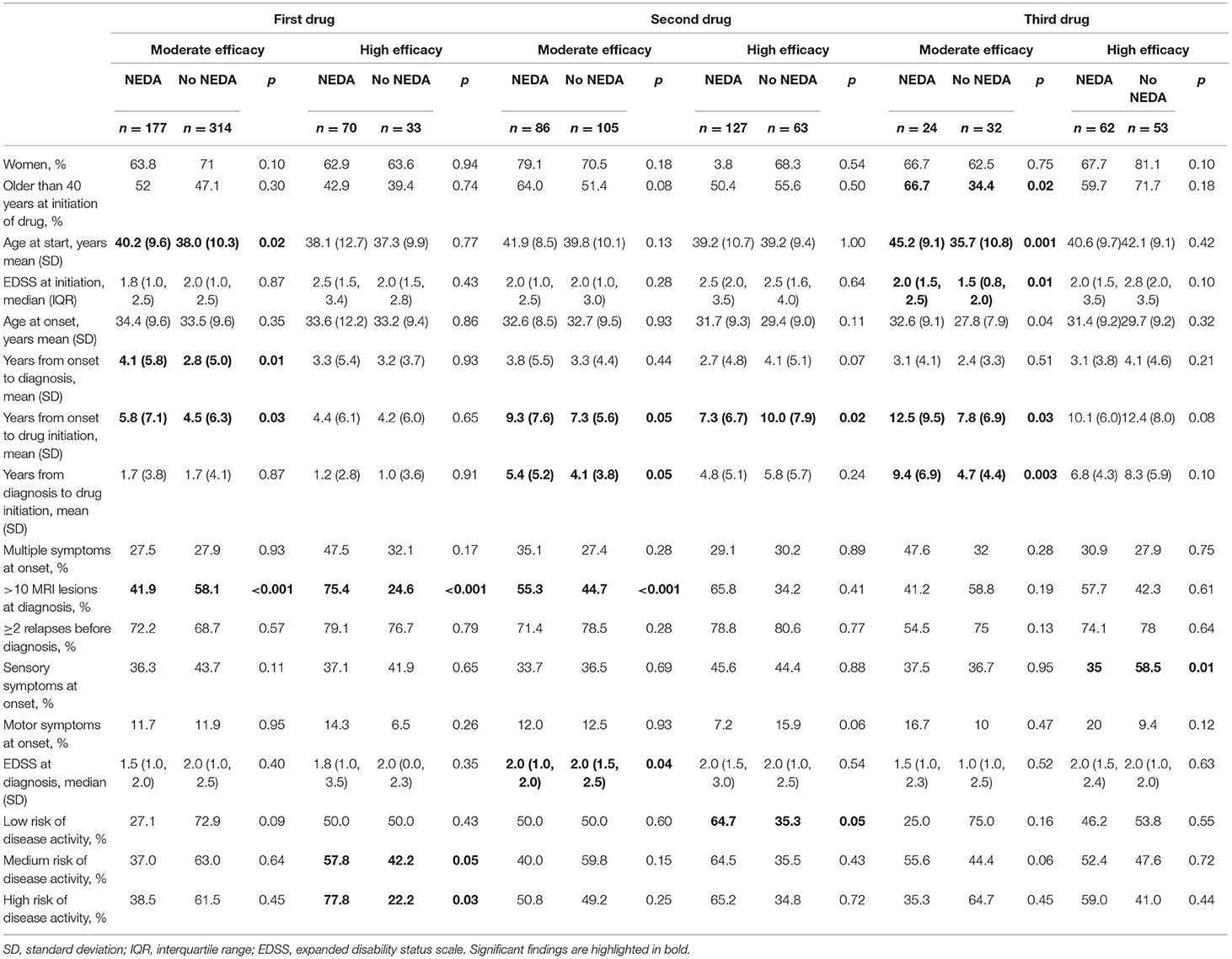
Table 6. Demographics by NEDA and no NEDA.
The numbers of patients on the individual drugs achieving NEDA are presented in Table 7. Natalizumab and fingolimod are the only DMTs that are significantly more likely than the injectables to achieve NEDA at year 1 and 2 as a first drug, though the numbers of alemtuzumab were small and 100% of patients on alemtuzumab as a second drug achieved NEDA. All the DMTs were superior to the injectables as a second drug. The adjusted odds ratio of each individual drug vs. the injectables are presented in Table 7 and Figure 2. Natalizumab as a first drug has an odds ratio of 7.4 (95% CI 3.5–15.4, p < 0.001) for reaching NEDA, which is superior to all the other drugs (see Figure 2), though the confidence interval is large. Teriflunomide and dimethyl-fumarate as a first drug did not have significantly better odds ratios at year 1 or 2 than the injectables. As a second drug, all the DMTs were superior to injectables at year 1 and 2. The odds ratio of achieving NEDA on a third drug was less convincing. Adjusting for sex, age at start of medication, time from onset to start of medication and risk groups did not meaningfully alter the results.
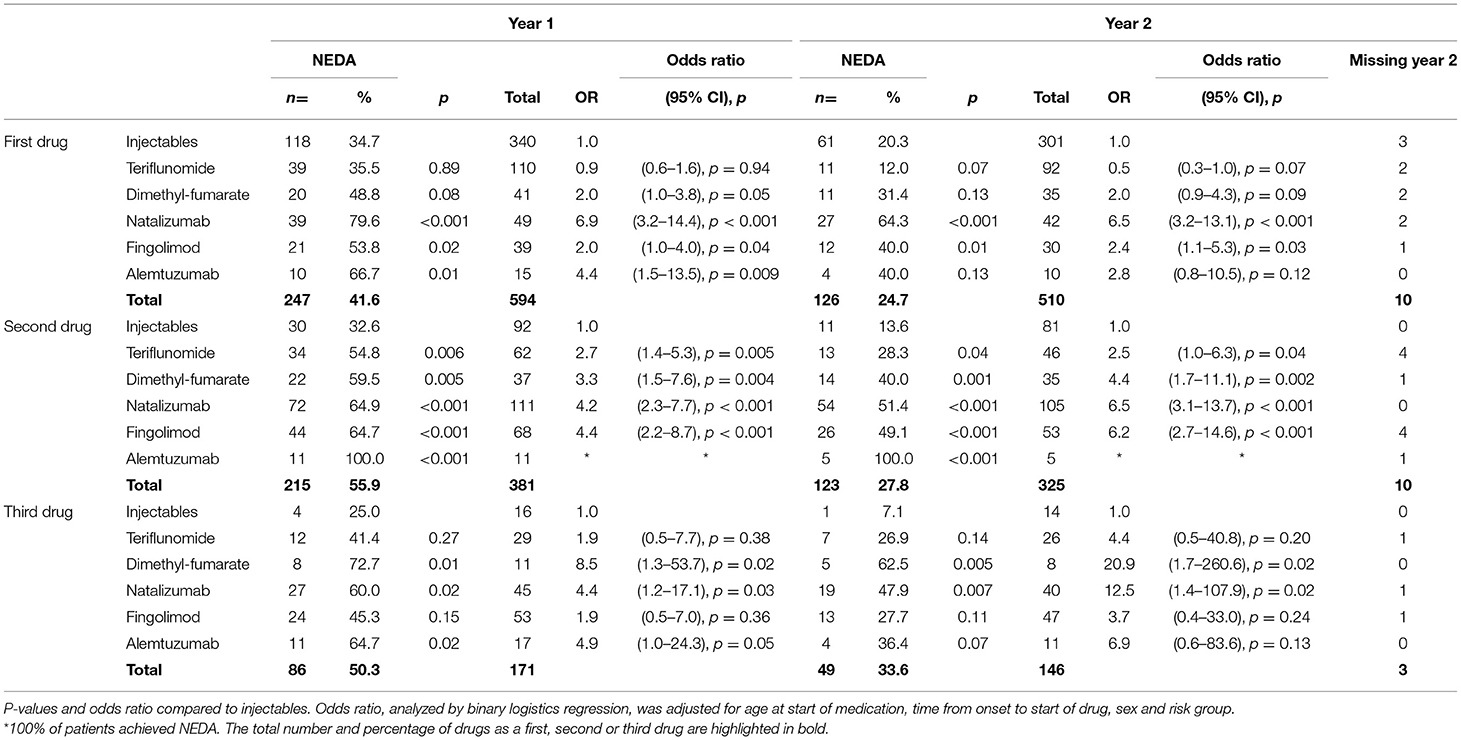
Table 7. NEDA and odds ratio of reaching NEDA on individual drugs at year 1 and 2.
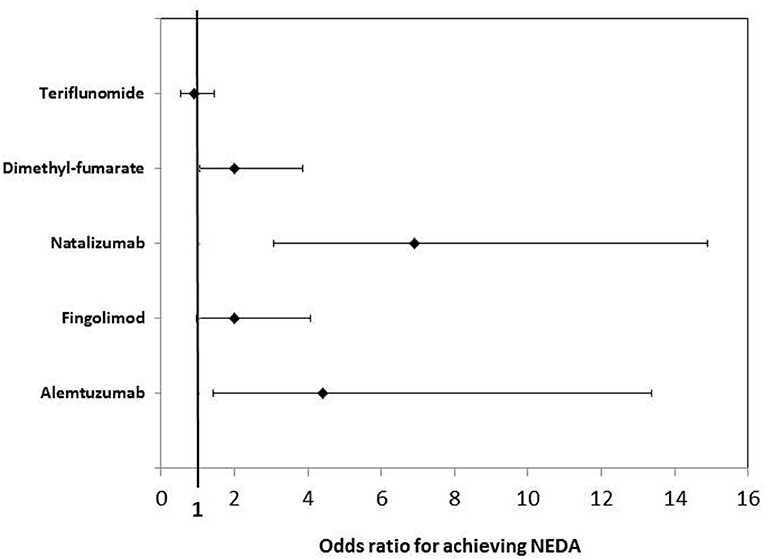
Figure 2. Forest plot of odds ratio for reaching NEDA at year 1 compared to the injectables (interferon and glatiramer acetate).
Unsurprisingly, patients on moderate efficacy therapy as a first drug were more likely to discontinue treatment than patients on a high efficacy therapy as a first drug (65.2 vs. 29.2%, p < 0.001). This was also the case in patients on a second drug (55.4 vs. 42.7%, p = 0.02) but not in patients on a third drug (42.9 vs. 29.5%, p = 0.10). Table 8 shows the number of patients who discontinued therapy on moderate and high efficacy therapies and causes of discontinuation. Patients on moderate efficacy therapy as a first drug were more likely to discontinue due to side effects than patients on high efficacy therapy as a first drug (45 vs. 14%, p = 0.002). This was also the case for the second drug (40 vs. 14%, p < 0.001). The number of patients who discontinued a third drug were too small to draw a conclusion (n = 4 and n = 5).
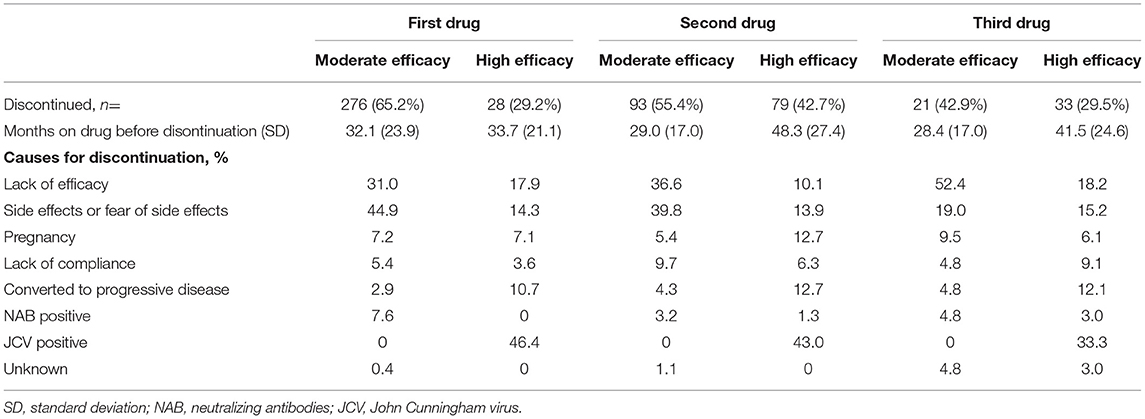
Table 8. Information on drug discontinuation.
Discussion
In this Norwegian population-based, real-world study we found that patients who start high efficacy therapies are significantly more likely to achieve NEDA at year 1 and 2 than patients starting moderate efficacy therapy. However, the odds ratio of achieving NEDA is reduced for each attempted drug.
Patients started on a high efficacy drug as a first DMT had an odds ratio of achieving NEDA of 3.9 compared to the moderate efficacy drugs, adjusting for sex, age and time from onset to diagnosis. The odds ratio was reduced to 2.5 as a second drug, and the odds ratio of 1.5 was not significant for the third drug. Age did not have a notable impact on the proportion of patients achieving NEDA on the first and second drug, but older patients were less likely to achieve NEDA on the third drug. Our findings illustrate the importance of choosing the most effective drug at the time of diagnosis. These findings were especially strong in the 90% of patients who were classified as having a medium to high risk of disease activity.
NEDA is by no means a perfect tool as it is overly reliant on MRI (29), it does not take into account subtle deterioration in fine motor skills and cognitive changes, and there is no consensus regarding the definitions of the different components (13). Failure to achieve NEDA is not necessarily a good predictor of long-term disability (14). However, neuronal injury occurs early in the disease, and limited disease activity within the first few years of diagnosis is widely regarded as a good prognostic sign (15).
Our findings are in accordance with studies supporting high efficacy therapy at the time of diagnosis compared to an escalation approach (30, 31). The escalation approach may be inadequate to prevent unfavorable outcomes in a real-world population (32), and this is important as the disease activity in the first couple of years influence the disease course (33, 34). The risk of progression at 10 years is highly dependent on EDSS score at 5 years, and it progresses more rapidly from EDSS 4 onwards compared to EDSS 2 and onwards (35). In the absence of a cure, an increasing body of evidence supports early initiation of high efficacy disease modifying treatment in MS to halt disease activity and reduce disability progression (36, 37).
However, many neurologists still utilize a stepwise approach in initiating disease modifying therapy, starting with the safer, but less effective therapies, and only escalate once there is sign of disease activity (38). This is reflected in national guidelines, regulatory bodies and insurance policies (1, 30, 39). In addition, some argue that there is no need for high efficacy treatment in patients with positive prognostic factors and a suspected “mild” disease (5). In our cohort, patients who achieved NEDA on moderate efficacy drugs tended to be older and have longer time from onset and diagnosis to start of drug initiation. This most likely reflects the disease rather than the drug efficacy. Patients with delayed drug initiation after onset and diagnosis have more likely been followed with a watchful wait approach (40). These patients have fewer relapses and less MRI activity, and thus less disease activity and less incentive to initiate immunomodulatory treatment early. However, the concept of mild or benign MS is controversial (37, 41). One study found only nine of 1,049 patients with disease duration of >15 years and EDSS <4 were truly benign (42). Ellenberger et al. found one in four patients with benign MS at 15 years were unemployed, and only one in three remained benign after 30 years (43). Smestad et al. found that although only one third of MS patients in an Oslo cohort had mild disability based on EDSS, half of them were cognitively impaired (44).
One argument for not initiating high efficacy treatment early is the safety profile (15). However, natalizumab has few side effects beyond the risk of progressive multifocal leukoencephalopathy (PML), and this risk has been mitigated with intensified follow-up regimes, monitoring of the JC-virus index and possibly extended interval dosing (45). The three hospitals included in this study utilize natalizumab frequently. We check JC-virus index biannually and discontinue the drug in cases of elevated titres. Due to risk stratification, none of the hospitals has experienced PML, despite a combined population of more than 2,500 patients, or a quarter of the national MS population. In addition, patients treated with alemtuzumab are monitored closely for 5 years after treatment initiation, and there have been no deadly outcomes from alemtuzumab treatment. Also moderate efficacy drugs are certainly not without side effects that can significantly affect quality of life (46). Our population was significantly more likely to discontinue moderate efficacy therapies due to side effects than high efficacy therapies. The injectables have poorer acceptability profiles than other DMTs, and the high efficacy drugs have lower dropout rates than moderate efficacy drugs (47). Although side effects from moderate efficacy therapies are rarely life threatening, there are several reported cases of PML in Tecfidera treated patients (48). In the end, higher disability at a younger age seems a more significant risk than most of the adverse effects associated with established high efficacy DMTs.
The European (ECTRIMS/EAN) guidelines of 2018 suggest the choice of treatment depends on patient characteristics, disease severity, safety profile and drug accessibility (6). They advise escalating treatment if there is disease activity despite injection therapy. The American Academy of Neurology guidelines notes that patients with a highly active disease should be treated with high efficacy DMT (7). Neither the European guidelines, nor the American guidelines recommend a specific treatment strategy. Two large randomized clinical trials (TREAT-MS, NCT035300328 and DELIVER-MS, NCT03535298) examining escalation vs. early high efficacy therapy are currently underway and will provide valuable information on the short-term differences between these two treatment strategies. However, the differences in long-term disability will require decades of follow-up time, and the available evidence favors early high efficacy therapy. In our opinion, international guidelines should consider updating their recommendations according to current knowledge.
The strength of this study is the well-defined study population. The ratio of neurologists per capita in 2017 was 9.5/100,000 (data from The Norwegian Doctors' Union), and almost all Norwegian MS patients are followed by neurologists at public hospitals. There are few neurologists in private practice. All Norwegian MS neurologists had complete access to all therapies available in Europe at the time of approval, and all these drugs are reimbursed. Real-world studies, such as this, are not restricted by stringent inclusion criteria but instead assess the entire heterogeneous population and can therefore be generalized beyond their study frames (49). BOT-MS is a population-based registry, and a major strength as a real-world study is that we have limited selection bias and know who is missing and why.
Real-world data is also subject to missing data, which is a source of potential information bias. Many of the patients started on the injectables might not have been followed as strictly as those started on the newer drugs. Thus, patients with enough information on the composites of NEDA to be included were likely to have more disease activity. This means there may be an underrepresentation of NEDA patients in this group. This possible information bias was partly counteracted by only including patients started on treatment as of 2006, the year the first highly potent disease modifying drug, natalizumab, was made available to our patients. From this point onwards, there was a more stringent follow-up process of all MS patients. In addition, the odds ratio for teriflunomide was the same as injectables. Our findings also remained largely unchanged before and after 2013, which marks the introduction of teriflunomide and dimethyl-fumarate.
We have created a risk score to categorize patients as having low, medium and high risk of disease activity. Our choices in creating this score were based on available literature (17–26), though we acknowledge that others may categorize the risk differently. In fact, the MS community's ability of predicting individual disease development is limited (37). Our score is based on easily accessible data, though ideally it should have included information on smoking (50), vitamin D (51), and spinal cord lesions, gadolinium enhancing lesions (52) and atrophy (53) on MRI, to name a few. This score has not yet been validated, and we would like to validate it in a new population. We could have used propensity score analyses to control for confounding, but propensity score matching does not yield different estimates compared to conventional multivariate methods (54) and is often used inappropriately in MS research (55).
We acknowledge that treatment allocation bias may play a role in this study. The cohort exposed to high efficacy drugs as a first drug were younger, with lower disease duration and more MRI lesions and relapses at presentation. It is likely that this would lead to a greater response to immunotherapy (15). We do not believe this weakens our study, but rather strengthens our findings and our conclusion that more people should be offered high efficacy therapies. Of the 199 people with medium or high risk of disease activity diagnosed in 2013 or after, 64% were started on moderate efficacy therapy as a first drug. These patients should have received high efficacy therapy from the start (37).
We have chosen to categorize fingolimod as a high efficacy therapy since that is how it was portrayed when it first arrived on the market (56). International, national and local guidelines (6) consequently recommended it as a choice for treatment escalation in highly active MS during the span of this study, and treatment choices were subsequently decided based on this premise. However, many studies conclude that fingolimod has a similar efficacy profile to the moderate efficacy therapy dimethyl-fumarate (57, 58), though not all (16, 47). We have shown NEDA-data on each individual drug in this study in addition to the two efficacy groups. Regardless, the allocation of fingolimod as a moderate efficacy therapy would only strengthen our conclusion that achieving NEDA is significantly more likely in patients on high-efficacy disease modifying therapies.
Another potential bias is observation bias. All patients treated with natalizumab are seen monthly, and the patients treated with teriflunomide are seen frequently in the first year after initiation. These patients were thus more inclined to mention relapses to their treating MS team, as opposed to the remaining MS patients who are seen less often (59). Despite this, natalizumab patients did better than other patients. Another weakness is the retrospective data retrieval, subjecting the study to investigator bias. This was ameliorated by only having three neurologists specialized in MS to include in the database based on a mutually accepted manual. Finally, we did not have enough observations to make a confident statement on the odds ratio of reaching NEDA on alemtuzumab, and we have not included cladribine, another high efficacy DMT, which was approved after the inclusion period.
Conclusion
Achieving NEDA is significantly more likely in patients on high-efficacy disease modifying therapies than on moderate efficacy therapies, and the first choice of treatment is the most important. Moderate efficacy therapies should be used with caution in most MS patients, unless the clinician is confident the patient has a less active form of MS. There is a need for updating immunomodulatory treatment guidelines ensuring early, high efficacy therapy for the majority of patients diagnosed with MS.
Data Availability Statement
The datasets presented in this article are not readily available because one of the conditions for ethics approval was that strict privacy concerns were respected, and that data was not made publicly available. Requests to access the datasets should be directed to cecsim@vestreviken.no.
Ethics Statement
The studies involving human participants were reviewed and approved by Regional Ethics Committee in Norway (REK 2015/670). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
CS, HF, LB, PB-H, SM, and EC: design and conceptualization. CS, HF, and LB: data acquisition. CS, HF, LB, CB, PB-H, SM, and EC: data analysis, data interpretation, and writing original draft. All authors contributed to the article and approved the submitted version.
Funding
The authors declare that this study received unrestricted funding from Sanofi (grant number GZ-2014-11451). The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Conflict of Interest
CS has received unrestricted research grant from Sanofi and Novartis, advisory board and/or speaker honoraria from Sanofi, Merck, Novartis, and Biogen Idec. HF has received unrestricted research grant Biogen Idec and Novartis, advisory board and/or speaker honoraria Sanofi, Merck, and Biogen Idec. LB has received an unrestricted grant from Sanofi Genzyme and advisory board honoraria from Merck. PB-H has received advisory board and/or speaker honoraria from Novartis, UCB, Sanofi, Merck, and Biogen Idec. EC has received unrestricted research grants from Novartis and Sanofi, advisory boards and/or speaker honoraria (Almirall, Biogen Idec, Merck, Roche, Novartis, Sanofi, and Teva).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The BOT research group would like to thank all the patients in our database, as well as dedicated colleagues who have kept detailed notes on each patient and their disease throughout the past few decades.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2021.693017/full#supplementary-material
References
1. Giovannoni G, Butzkueven H, Dhib-Jalbut S, Hobart J, Kobelt G, Pepper G, et al. Brain health: time matters in multiple sclerosis. Mult Scler Relat Disord. (2016) 9(Suppl. 1):S5–48. doi: 10.1016/j.msard.2016.07.003
2. Kobelt G, Thompson A, Berg J, Gannedahl M, Eriksson J. New insights into the burden and costs of multiple sclerosis in Europe. Mult Scler (Houndmills, Basingstoke, England). (2017) 23:1123–36. doi: 10.1177/1352458517694432
3. Interferon beta-1b in the treatment of multiple sclerosis: final outcome of the randomized controlled trial. The IFNB Multiple Sclerosis Study Group and The University of British Columbia MS/MRI Analysis Group. Neurology. (1995) 45:1277–85. doi: 10.1212/WNL.45.7.1277
4. Polman CH, O'Connor PW, Havrdova E, Hutchinson M, Kappos L, Miller DH, et al. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N Engl J Med. (2006) 354:899–910. doi: 10.1056/NEJMoa044397
5. Ontaneda D, Tallantyre E, Kalincik T, Planchon SM, Evangelou N. Early highly effective versus escalation treatment approaches in relapsing multiple sclerosis. Lancet Neurol. (2019) 18:973–80. doi: 10.1016/S1474-4422(19)30151-6
6. Montalban X, Gold R, Thompson AJ, Otero-Romero S, Amato MP, Chandraratna D, et al. ECTRIMS/EAN guideline on the pharmacological treatment of people with multiple sclerosis. Eur J Neurol. (2018) 25:215–37. doi: 10.1111/ene.13536
7. Rae-Grant A, Day GS, Marrie RA, Rabinstein A, Cree BAC, Gronseth GS, et al. Practice guideline recommendations summary: disease-modifying therapies for adults with multiple sclerosis: report of the guideline development, dissemination, and implementation subcommittee of the American Academy of Neurology. Neurology. (2018) 90:777–88. doi: 10.1212/WNL.0000000000005347
8. Beiki O, Frumento P, Bottai M, Manouchehrinia A, Hillert J. Changes in the risk of reaching multiple sclerosis disability milestones in recent decades: a nationwide population-based cohort study in Sweden. JAMA Neurol. (2019) 76:665–71. doi: 10.1001/jamaneurol.2019.0330
9. Simonsen CS, Flemmen H, Broch L, Brunborg C, Berg-Hansen P, Moen SM, et al. The course of multiple sclerosis rewritten: a Norwegian population-based study on disease demographics and progression. J Neurol. (2021) 268:1330–41. doi: 10.1007/s00415-020-10279-7
10. Kingwell E, Leray E, Zhu F, Petkau J, Edan G, Oger J, et al. Multiple sclerosis: effect of beta interferon treatment on survival. Brain J Neurol. (2019) 142:1324–33. doi: 10.1093/brain/awz055
11. Cohen JA, Trojano M, Mowry EM, Uitdehaag BMJ, Reingold SC, Marrie RA. Leveraging real-world data to investigate multiple sclerosis disease behavior, prognosis, and treatment. Mult Scler J. (2019) 26:23–37. doi: 10.1177/1352458519892555
12. Giovannoni G, Turner B, Gnanapavan S, Offiah C, Schmierer K, Marta M. Is it time to target no evident disease activity (NEDA) in multiple sclerosis? Mult Scler Relat Disord. (2015) 4:329–33. doi: 10.1016/j.msard.2015.04.006
13. Giovannoni G, Tomic D, Bright JR, Havrdová E. “No evident disease activity”: the use of combined assessments in the management of patients with multiple sclerosis. Mult Scler (Houndmills, Basingstoke, England). (2017) 23:1179–87. doi: 10.1177/1352458517703193
14. Hegen H, Bsteh G, Berger T. ‘No evidence of disease activity'—is it an appropriate surrogate in multiple sclerosis? Eur J Neurol. (2018) 25:1107–e101. doi: 10.1111/ene.13669
15. Comi G, Radaelli M, Soelberg Sorensen P. Evolving concepts in the treatment of relapsing multiple sclerosis. Lancet (London, England). (2017) 389:1347–56. doi: 10.1016/S0140-6736(16)32388-1
16. Kalincik T, Kubala Havrdova E, Horakova D, Izquierdo G, Prat A, Girard M, et al. Comparison of fingolimod, dimethyl fumarate and teriflunomide for multiple sclerosis. J Neurol Neurosurg Psychiatry. (2019) 90:458–68. doi: 10.1136/jnnp-2018-319831
17. Confavreux C, Vukusic S, Adeleine P. Early clinical predictors and progression of irreversible disability in multiple sclerosis: an amnesic process. Brain J Neurol. (2003) 126:770–82. doi: 10.1093/brain/awg081
18. Weinshenker BG. Natural history of multiple sclerosis. Ann Neurol. (1994) 36:S6–11. doi: 10.1002/ana.410360704
19. Tomassini V, Fanelli F, Prosperini L, Cerqua R, Cavalla P, Pozzilli C. Predicting the profile of increasing disability in multiple sclerosis. Mult Scler (Houndmills, Basingstoke, England). (2019) 25:1306–15. doi: 10.1177/1352458518790397
20. Tintore M, Rovira À, Río J, Otero-Romero S, Arrambide G, Tur C, et al. Defining high, medium and low impact prognostic factors for developing multiple sclerosis. Brain J Neurol. (2015) 138:1863–74. doi: 10.1093/brain/awv105
21. Bsteh G, Ehling R, Lutterotti A, Hegen H, Di Pauli F, Auer M, et al. Long term clinical prognostic factors in relapsing-remitting multiple sclerosis: insights from a 10-year observational study. PLoS ONE. (2016) 11:e0158978. doi: 10.1371/journal.pone.0158978
22. Miller DH, Hornabrook RW, Purdie G. The natural history of multiple sclerosis: a regional study with some longitudinal data. J Neurol Neurosurg Psychiatry. (1992) 55:341–6. doi: 10.1136/jnnp.55.5.341
23. Weinshenker BG, Ebers GC. The natural history of multiple sclerosis. Can J Neurol Sci. (1987) 14:255–61. doi: 10.1017/S0317167100026573
24. Eriksson M, Andersen O, Runmarker B. Long-term follow up of patients with clinically isolated syndromes, relapsing-remitting and secondary progressive multiple sclerosis. Mult Scler (Houndmills, Basingstoke, England). (2003) 9:260–74. doi: 10.1191/1352458503ms914oa
25. Scalfari A, Neuhaus A, Degenhardt A, Rice GP, Muraro PA, Daumer M, et al. The natural history of multiple sclerosis: a geographically based study 10: relapses and long-term disability. Brain J Neurol. (2010) 133:1914–29. doi: 10.1093/brain/awq118
26. Degenhardt A, Ramagopalan SV, Scalfari A, Ebers GC. Clinical prognostic factors in multiple sclerosis: a natural history review. Nat Rev Neurol. (2009) 5:672–82. doi: 10.1038/nrneurol.2009.178
27. Sorensen PS, Sellebjerg F, Hartung HP, Montalban X, Comi G, Tintoré M. The apparently milder course of multiple sclerosis: changes in the diagnostic criteria, therapy and natural history. Brain J Neurol. (2020) 143:2637–52. doi: 10.1093/brain/awaa145
28. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. (1983) 33:1444–52. doi: 10.1212/WNL.33.11.1444
29. Stangel M, Penner IK, Kallmann BA, Lukas C, Kieseier BC. Towards the implementation of 'no evidence of disease activity' in multiple sclerosis treatment: the multiple sclerosis decision model. Ther Adv Neurol Disord. (2015) 8:3–13. doi: 10.1177/1756285614560733
30. Brown JWL, Coles A, Horakova D, Havrdova E, Izquierdo G, Prat A, et al. Association of initial disease-modifying therapy with later conversion to secondary progressive multiple sclerosis. JAMA. (2019) 321:175–87. doi: 10.1001/jama.2018.20588
31. He A, Merkel B, Brown JWL, Zhovits Ryerson L, Kister I, Malpas CB, et al. Timing of high-efficacy therapy for multiple sclerosis: a retrospective observational cohort study. Lancet Neurol. (2020) 19:307–16. doi: 10.1016/S1474-4422(20)30067-3
32. Harding K, Williams O, Willis M, Hrastelj J, Rimmer A, Joseph F, et al. Clinical outcomes of escalation vs. early intensive disease-modifying therapy in patients with multiple sclerosis. JAMA Neurol. (2019) 76:536–41. doi: 10.1001/jamaneurol.2018.4905
33. Chalmer TA, Baggesen LM, Nørgaard M, Koch-Henriksen N, Magyari M, Sorensen PS. Early versus later treatment start in multiple sclerosis: a register-based cohort study. Eur J Neurol. (2018) 25:1262-e110. doi: 10.1111/ene.13692
34. Scalfari A, Neuhaus A, Daumer M, Muraro PA, Ebers GC. Onset of secondary progressive phase and long-term evolution of multiple sclerosis. J Neurol Neurosurg Psychiatry. (2014) 85:67–75. doi: 10.1136/jnnp-2012-304333
35. Hughes S, Spelman T, Trojano M, Lugaresi A, Izquierdo G, Grand'maison F, et al. The Kurtzke EDSS rank stability increases 4 years after the onset of multiple sclerosis: results from the MSBase Registry. J Neurol Neurosurg Psychiatry. (2012) 83:305–10. doi: 10.1136/jnnp-2011-301051
36. Signori A, Schiavetti I, Gallo F, Sormani MP. Subgroups of multiple sclerosis patients with larger treatment benefits: a meta-analysis of randomized trials. Eur J Neurol. (2015) 22:960–6. doi: 10.1111/ene.12690
37. Stankiewicz JM, Weiner HL. An argument for broad use of high efficacy treatments in early multiple sclerosis. Neurol Neuroimmunol Neuroinflamm. (2019) 7:e636. doi: 10.1212/NXI.0000000000000636
38. Scolding N, Barnes D, Cader S, Chataway J, Chaudhuri A, Coles A, et al. Association of British Neurologists: revised (2015) guidelines for prescribing disease-modifying treatments in multiple sclerosis. Pract Neurol. (2015) 15:273–9. doi: 10.1136/practneurol-2015-001139
39. Browne P, Chandraratna D, Angood C, Tremlett H, Baker C, Taylor BV, et al. Atlas of multiple sclerosis 2013: a growing global problem with widespread inequity. Neurology. (2014) 83:1022–4. doi: 10.1212/WNL.0000000000000768
40. Bsteh G, Hegen H, Dosser C, Auer M, Berek K, Wurth S, et al. To treat or not to treat: sequential individualized treatment evaluation in relapsing multiple sclerosis. Mult Scler Relat Disord. (2019) 39:101908. doi: 10.1016/j.msard.2019.101908
41. Amato MP, Portaccio E. Truly benign multiple sclerosis is rare: let's stop fooling ourselves–yes. Mult Scler (Houndmills, Basingstoke, England). (2012) 18:13–4. doi: 10.1177/1352458511431732
42. Tallantyre EC, Major PC, Atherton MJ, Davies WA, Joseph F, Tomassini V, et al. How common is truly benign MS in a UK population? J Neurol Neurosurg Psychiatry. (2019) 90:522–8. doi: 10.1136/jnnp-2018-318802
43. Ellenberger D, Flachenecker P, Haas J, Hellwig K, Paul F, Stahmann A, et al. Is benign MS really benign? What a meaningful classification beyond the EDSS must take into consideration. Mult Scler Relat Disord. (2020) 46:102485. doi: 10.1016/j.msard.2020.102485
44. Smestad C, Sandvik L, Landrø NI, Celius EG. Cognitive impairment after three decades of multiple sclerosis. Eur J Neurol. (2010) 17:499–505. doi: 10.1111/j.1468-1331.2009.02889.x
45. Ryerson LZ, Foley J, Chang I, Kister I, Cutter G, Metzger RR, et al. Risk of natalizumab-associated PML in patients with MS is reduced with extended interval dosing. Neurology. (2019) 93:e1452–62. doi: 10.1212/WNL.0000000000008243
46. Torkildsen Ø, Myhr KM, Bø L. Disease-modifying treatments for multiple sclerosis - a review of approved medications. Eur J Neurol. (2016) 23(Suppl. 1):18–27. doi: 10.1111/ene.12883
47. Li H, Hu F, Zhang Y, Li K. Comparative efficacy and acceptability of disease-modifying therapies in patients with relapsing-remitting multiple sclerosis: a systematic review and network meta-analysis. J Neurol. (2020) 267:3489–98. doi: 10.1007/s00415-019-09395-w
48. Jordan AL, Yang J, Fisher CJ, Racke MK, Mao-Draayer Y. Progressive multifocal leukoencephalopathy in dimethyl fumarate-treated multiple sclerosis patients. Mult Scler (Houndmills, Basingstoke, England). (2020). doi: 10.1177/1352458520949158. [Epub ahead of print].
49. Sormani MP, Bruzzi P. Can we measure long-term treatment effects in multiple sclerosis? Nat Rev Neurol. (2015) 11:176–82. doi: 10.1038/nrneurol.2014.237
50. Rosso M, Chitnis T. Association between cigarette smoking and multiple sclerosis: a review. JAMA Neurol. (2020) 77:245–53. doi: 10.1001/jamaneurol.2019.4271
51. Ascherio A, Munger KL, White R, Köchert K, Simon KC, Polman CH, et al. Vitamin D as an early predictor of multiple sclerosis activity and progression. JAMA Neurol. (2014) 71:306–14. doi: 10.1001/jamaneurol.2013.5993
52. Brownlee WJ, Altmann DR, Prados F, Miszkiel KA, Eshaghi A, Gandini Wheeler-Kingshott CAM, et al. Early imaging predictors of long-term outcomes in relapse-onset multiple sclerosis. Brain J Neurol. (2019) 142:2276–87. doi: 10.1093/brain/awz156
53. Odenthal C, Coulthard A. The prognostic utility of MRI in clinically isolated syndrome: a literature review. Am J Neuroradiol. (2015) 36:425–31. doi: 10.3174/ajnr.A3954
54. Stürmer T, Joshi M, Glynn RJ, Avorn J, Rothman KJ, Schneeweiss S. A review of the application of propensity score methods yielded increasing use, advantages in specific settings, but not substantially different estimates compared with conventional multivariable methods. J Clin Epidemiol. (2006) 59:437–47. doi: 10.1016/j.jclinepi.2005.07.004
55. Karim ME, Pellegrini F, Platt RW, Simoneau G, Rouette J, de Moor C. The use and quality of reporting of propensity score methods in multiple sclerosis literature: a review. Mult Scler (Houndmills, Basingstoke, England). (2020). doi: 10.1177/1352458520972557. [Epub ahead of print].
56. Fazekas F, Bajenaru O, Berger T, Fabjan TH, Ledinek AH, Jakab G, et al. How does fingolimod (gilenya®) fit in the treatment algorithm for highly active relapsing-remitting multiple sclerosis? Front Neurol. (2013) 4:10. doi: 10.3389/fneur.2013.00010
57. Vollmer B, Ontaneda D, Harris H, Nair K, Bermel RA, Corboy JR, et al. Comparative discontinuation, effectiveness, and switching practices of dimethyl fumarate and fingolimod at 36-month follow-up. J Neurol Sci. (2019) 407:116498. doi: 10.1016/j.jns.2019.116498
58. Lorscheider J, Benkert P, Lienert C, Hänni P, Derfuss T, Kuhle J, et al. Comparative analysis of dimethyl fumarate and fingolimod in relapsing-remitting multiple sclerosis. J Neurol. (2021) 268:941–9. doi: 10.1007/s00415-020-10226-6
59. Steinvorth SM, Röver C, Schneider S, Nicholas R, Straube S, Friede T. Explaining temporal trends in annualised relapse rates in placebo groups of randomised controlled trials in relapsing multiple sclerosis: systematic review and meta-regression. Mult Scler (Houndmills, Basingstoke, England). (2013) 19:1580–6. doi: 10.1177/1352458513481009
Keywords: multiple sclerosis, disease modifying therapies, no evidence of disease activity, disease activity, treatment decision
Citation: Simonsen CS, Flemmen HØ, Broch L, Brunborg C, Berg-Hansen P, Moen SM and Celius EG (2021) Early High Efficacy Treatment in Multiple Sclerosis Is the Best Predictor of Future Disease Activity Over 1 and 2 Years in a Norwegian Population-Based Registry. Front. Neurol. 12:693017. doi: 10.3389/fneur.2021.693017
Received: 09 April 2021; Accepted: 25 May 2021;
Published: 17 June 2021.
Edited by:
Mahsa Ghajarzadeh, Universal Scientific Education and Research Network, IranReviewed by:
Fritz Leutmezer, Medical University of Vienna, AustriaPaolo A. Muraro, Imperial College, United Kingdom
Copyright © 2021 Simonsen, Flemmen, Broch, Brunborg, Berg-Hansen, Moen and Celius. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cecilia Smith Simonsen, cecsim@vestreviken.no