Red cell distribution width (RDW) is correlated to time of oxygen desaturation < 90% and length of sleep apneas in patients with sleep disorder breathing (SDB) and acute heart failure with preserved ejection fraction (HFpEF)
 Cosimo A. Stamerra1†
Cosimo A. Stamerra1†  Emilia D'Elia2*†
Emilia D'Elia2*†  Mauro Gori2 Federica Roncali2
Mauro Gori2 Federica Roncali2  Alberto Cereda2
Alberto Cereda2  Antonello Gavazzi3
Antonello Gavazzi3  Claudio Ferri1 Michele Senni2,4
Claudio Ferri1 Michele Senni2,4- 1Department of Life, Health and Environmental Sciences, University of L'Aquila, L'Aquila, Italy
- 2Cardiology Unit, Hospital Papa Giovanni XXIII, Bergamo, Italy
- 3Fondazione Ricerca Ospedale Maggiore (FROM) Research Center, Hospital Papa Giovanni XXIII, Bergamo, Italy
- 4Cardiology Department, University of Milano-Bicocca, Milan, Italy
Background: Heart failure with preserved ejection fraction (HFpEF) is very frequently associated to sleep breathing disorders (SDB). Red blood cell distribution width (RDW) has been shown to be a potential inflammatory index linked to the degree of hypoxia and oxidative stress.
Aim: To identify the existence of a possible relationship between sleep apnea, oxygen saturation (SaO2) and RDW in a population of subjects affected by acute HFpEF (AHFpEF).
Methods: AHFpEF patients with known history of SDB were enrolled and performed blood chemistry, echocardiography, and 24-h polysomnography (PSG).
Results: A total of 34 acute HFpEF patients (mean age 72.8 +/−8.63) were enrolled in the study. A control group of 24 non-HF patients were considered. Compared to controls, HFpEF patients showed a higher mean apnea hypopnea index (AHI), with prevalence of central apneas. A moderate to severe desaturation pattern was observed in AHFpEF vs. controls. RDW was significantly higher in AHFpEF patients vs. controls (mean value 14.7 +/−2.6 % vs. 9.1 +/−2.2, p < 0.05). In AHFpEF, RDW showed a positive correlation with time of SaO2 < 90% (r = 0.35, p = 0.04), and with mean length of apneic events (60 +/−28 s, r = 0.29, p = 0.03).
Conclusion: In patients with AHFpEF and SDB, a dependence relationship between RDW and duration of oxygen desaturation was observed, as if oxidative stress and inflammation related to RDW increase could also be linked to severity of sleep disorders in this population.
Introduction
Anisocytosis is a condition characterized by the presence of various sizes of red blood cells (RBCs) in the peripheral blood. Red cell distribution width (RDW) provides a quantitative measure of anisocytosis, and it is associated with the presence of subclinical systemic inflammation in a variety of clinical situation such as renal impairment, nutritional deficiencies, and aging (1). Anisocytosis worsens the prognosis of cardiovascular events in patients with heart failure (HF) or in asymptomatic patients at risk of developing HF (2). Moreover, the presence of anisocytosis in heart failure with preserved ejection fraction (HFpEF), has been demonstrated to be associated with a higher frequency of non-cardiac mortality. Several HFpEF comorbidities such as renal failure, arterial hypertension, metabolic dysfunctions, neurocognitive impairment, oxidative stress, obesity, and diabetes worsen the degree of inflammation, and consequently increase RDW (3).
Sleep disordered breathing (SDB) is very common in HFpEF, with a prevalence between 50 and 70%, especially in case of obstructive sleep apneas (OSAS) (4–9). Intermittent hypoxia in OSAS triggers pro-inflammatory transcription factors, and consequent activation of inflammatory cells. To this regard, in a general population complaining snoring and witnessed apneas, it has been demonstrated a relationship between severity of OSAS and RDW that is dependent on inflammation and intermittent hypoxia, but independent from anemia (10).
Little is known regarding the role of RDW as a marker of inflammation in acute HFpEF (AHFpEF) patients with SDB, nor a potential correlation between RDW, OSAS, and oxygen saturation (SaO2) has ever been investigated in AHFpEF.
Thus, the aim of our study is to investigate a potential association between RDW, OSAS, and SaO2 in AHFpEF patients with history of SDB.
Materials and methods
Study population
We designed a prospective, single-center study approved by the Ethical Committee of Papa Giovanni XXIII Hospital, Bergamo, Italy. All consecutive AHFpEF patients admitted to the cardiology ward for decompensated HF between March 2019 and December 2020 were considered. Inclusion criteria were: (i) ≥18 years old; (ii) hospitalization for AHF, according to ESC guidelines (11); (iii) NYHA (New York Heart Association) class ≥ III; (iv) diuretic infusions required within 24 h from hospital admission; (v) presence of documented sleep apnea; (vi) written informed consent. Exclusion criteria were: (i) acute coronary syndrome; (ii) severe pulmonary disease; (iii) severe valvular disfunction. A control group of non HF patients with left ventricle ejection fraction (LVEF) >50% hospitalized for causes other than HF and acute myocardial ischemia was considered.
A set of biochemical tests, an echocardiogram and a 24 h polysomnography were performed in the acute phase of hospitalization, once the patient switched from intravenous to oral diuretics.
Median follow up was 18 months.
Polysomnography, echocardiogram, and biochemical tests
Embletta diagnostic system (ResMed TM, Sidney, Australia) is a portable device providing AHI (apnea hypopnea index), AI (Apnea Index), HI (Hypopnea Index), central apnea index (CAI), obstructive apnea index (OAI) through specific sensors able to detect respiratory and abdominal movements. “Apnea” is defined as an absence of airflow for at least 10 s, “hypopnea” is defined as a 30% reduction in airflow accompanied by a decrease in SaO2 of at least 4% (12). An AHI >15 events/h was considered significant for diagnosis of SDB. For all patients, 24 h polysomnography was settled during hospitalization, at the time of switch from intravenous to oral diuretic. The variables investigated were: AHI, AI, HI, CAI (central AI), OAI (obstructive AI), oxygen desaturation index (ODI), mean and minimum SaO2, time and percentage of desaturation <90%, number of desaturation events >4 %, and minimum and maximum length of an apneic event (seconds).
All enrolled patients underwent also a transthoracic echocardiography (TTE) in the acute phase of hospitalization. All parameters of diastolic dysfunction and right ventricular (RV) function were evaluated (Table 4).
The biochemical tests necessary for the performance of normal clinical-care activities were detected in all patients during the acute phase of hospitalization and the follow up visits.
Statistical analysis
PRISM 4 Software (GRAPHPAD PRISM 4.0; GraphPad Software, La Jolla, CA, USA) was used for statistical analyses of the entire population. Quantitative variables are shown by mean and standard deviation. All the variables were compared between cases and controls using non-parametric Wilcoxon tests (for continuous variables) or Fisher's exact tests (for categorical variables).
Overall, p-values below 0.05 were defined statistically significant.
Results
Between March 2019 and December 2020, a total of 34 AHFpEF patients (23 men, 11 women, mean age 72.8 +/−8.63), with SDB diagnosed by an AHI > 15 events/hour in a PSG performed within the previous 3 years were enrolled in the study. They were compared to a group of 24 non-HF patients admitted to the hospital for other cardiovascular causes, with a similar LVEF. Clinical characteristics and blood chemistry values of the patients enrolled are shown in Tables 1, 2. Medical treatment previous to enrollment is described in Table 3.
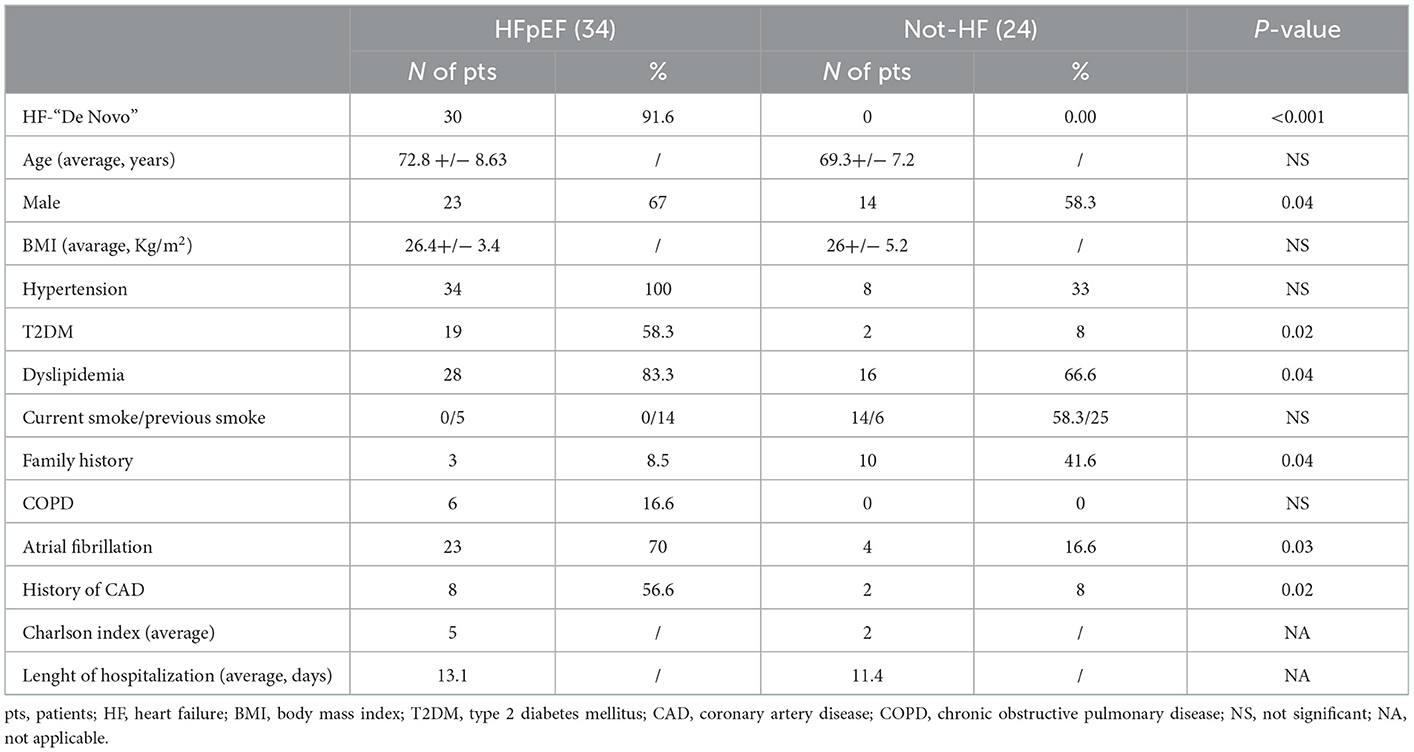
Table 1. Clinical characteristics of the patients enrolled.
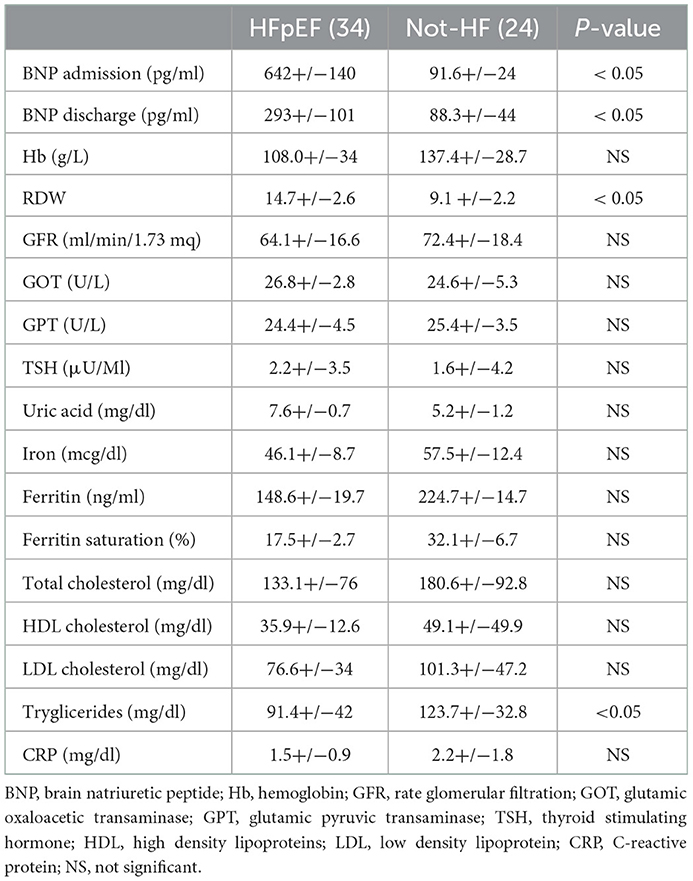
Table 2. Blood chemistry values.
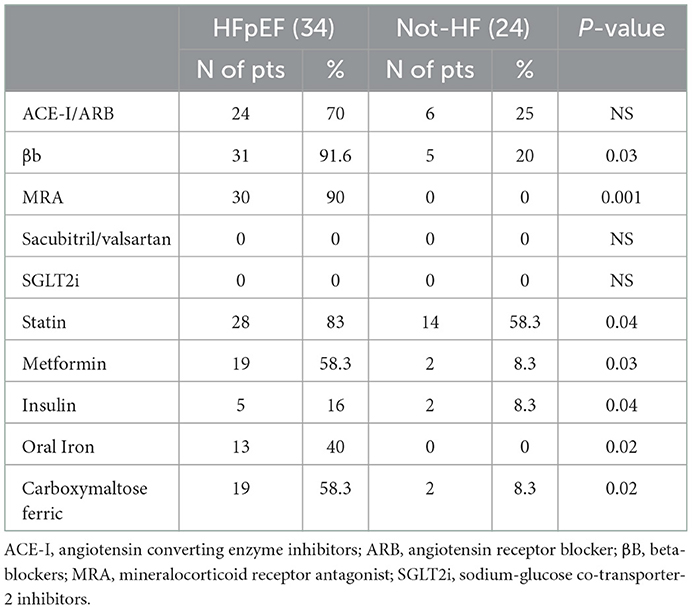
Table 3. Medical therapy.
In the AHFpEF group mean brain natriuretic peptide (BNP) at admission was 642 +/−140 ng/L. Every patient was treated with diuretic infusions and was than subjected to a 24 h PSG. In the case group vs. control group, a higher mean AHI was documented (27+/−36.7 events/hour vs. 9.8 +/−22 events/hours, p = 0.002), and a prevalence of central apneas was reported in AHFpEF patients (CAI = 10 +/−13.2; OAI = 3.5 +/−7.7). A moderate to severe desaturation pattern was observed in AHFpEF vs. controls (mean SaO2 = 92 +/−2.8 % vs. 93 +/−3%, p = 0.11; minimum SaO2 = 80.1 +/−14.2 % vs. 87.2 +/−10 %, p = 0.002; time SaO2 <90% = 80 +/−113 min vs. 12.2 +/−68, p = 0.02; Oxygen desaturation index (ODI) 22.1 +/−17.4 vs. 9.9 +/−12, p < 0.05). RDW was significantly higher in AHFpEF vs. non HF patients (mean value 14.7 +/- 2.6 % vs. 9.1 +/- 2.2, p < 0.05). In AHFpEF, RDW showed a positive correlation not only with time of SaO2 <90% (r = 0.35, p =0.04), but also with medium length of apneic events (60 +/−28 s, r = 0.29, p = 0.03). A strong positive correlation between RDW and mean pulmonary arterial pressure (PAPs 29.2 +/−12.4 mmHg, r = 0.54, p = 0.004) was observed.
In the two groups, nor C reactive protein or white blood cell count showed any significant correlation with PSG parameters related to hypoxia. Moreover, no significant correlations were documented between RDW and AHI, nor between RDW and BNP. Echocardiographic and polysomnographic values of the enrolled population are shown in Table 4. During the mean follow up of 18 months, 13 patients (38%) were admitted to hospital for worsening HF. These patients did not have a particular accentuation of basal sleep disturbances compared to those patients who were not re-admitted to the hospital.
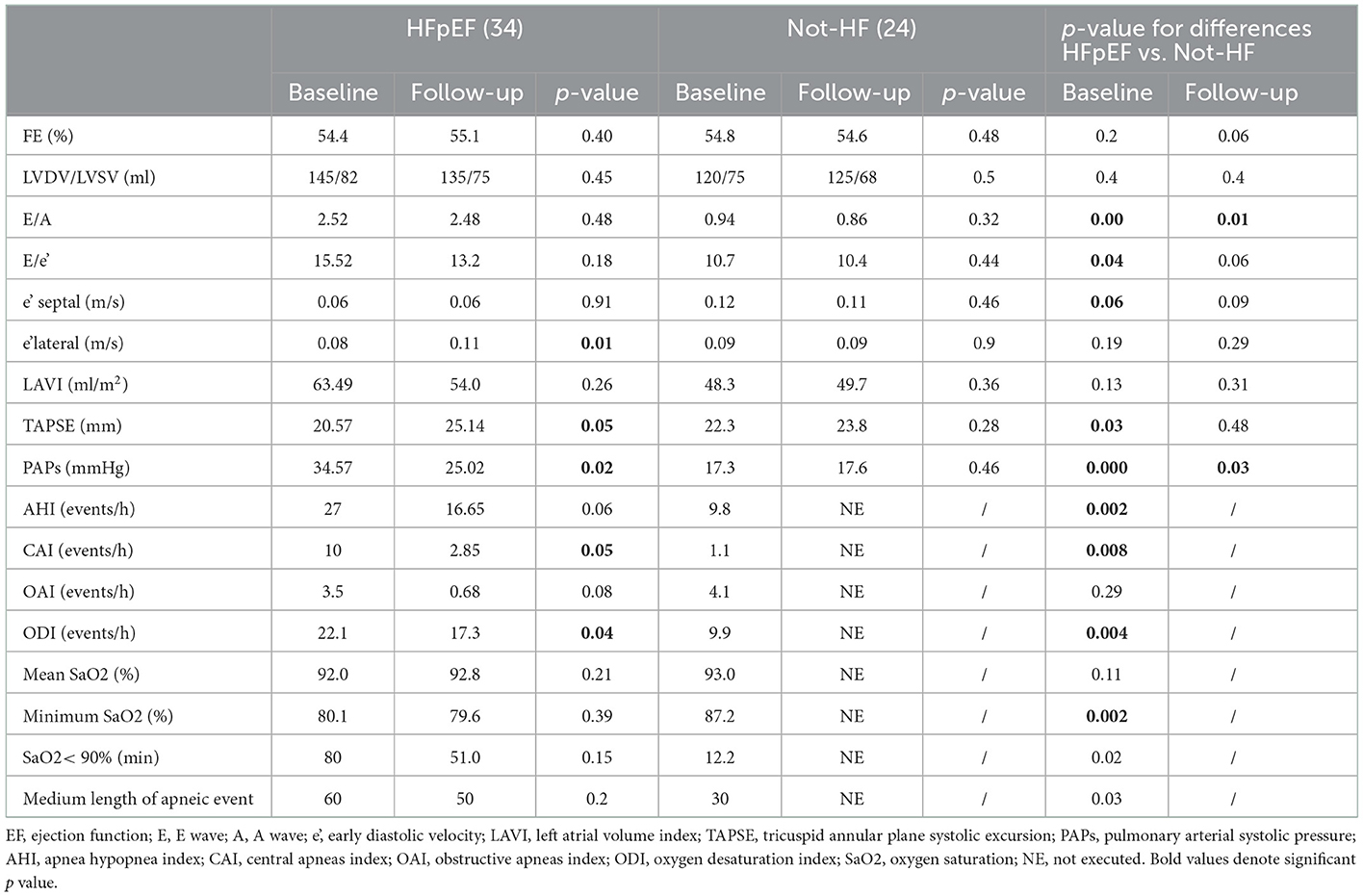
Table 4. Echocardiographic and polysomnographic values.
Discussion
In this study, we observed that AHFpEF patients seem to report a higher RDW value compared to non-HF patients with similar LVEF, and we hypothesize that RDW could be a subtle marker of inflammation in this population.
Anisocytosis, HFpEF, and SDB are three different entities, sharing many pathogenetic mechanisms.
Anisocytosis is an important predictor of morbidity and mortality in patients affected by various chronic diseases, such cardiovascular, pulmonary, and rheumatic diseases (13–16). Thus, mechanisms underlying the increase in RDW may affect outcomes in patients already affected by chronic diseases of different origins, as it happens in HFpEF. HFpEF is a complex clinical syndrome characterized by a normal LVEF in presence of a diastolic dysfunction, leading to myocardial stiffness and elevated filling pressures. Comorbidities, both cardiovascular and non-cardiovascular, are main features of HFpEF, whose phenotype directly depend on the interactions of these multiple co-existent diseases. Oxydative stress, endothelial dysfunction, and systemic inflammation are peculiar characteristics of HFpEF, in fact a chronic state of inflammation has largely been described as a substrate for the incipit, or at least the progression, of the disease (17–19).
SDB is a syndrome characterized by abnormal respiration during sleep, and it is strongly related to chronic inflammation, as intermittent hypoxia due to central or obstructive sleep apneas leads to the development of oxidative stress, endothelial dysfunction, and consequently a vicious circle enhancing both acute and chronic cardiovascular diseases (20, 21).
A connection among HFpEF, SDB, and anisocytosis could be surmised in the proinflammatory state which is typical of these pathologies. HFpEF and SDB are, in fact, characterized by hypoxia, oxidative stress, activation of inflammatory cytokines, activation of reactive oxygen species, and endothelial dysfunction (22–25), all of which lead to dyserythropoiesis with increased production of erythroblasts, with a larger size heterogeneity of RBC volumes (23).
Furthermore, subjects with HF and SDB are usually elderly and may be suffering from malnutrition, metabolic dysfunctions and chronic renal failure; these pathological conditions cause a reduced bone marrow production of RBCs, with an aggravation of anisocytosis (25–27).
In a recent study, Imai et al. evaluated the correlation between high RDW values at admission and poor outcomes due to non-cardiac events in 278 AHFpEF patients, thus acting as a long-term prognostic index (3).
In this framework, anisocytosis worsens tissue hypoxia already present both in HFpEF and in SDB, enhancing oxidative stress, apoptosis and myocardial fibrosis. Moreover, in HFpEF inflammatory molecular markers and soluble interleukin family members have been shown to be independent predictors of mortality (28–30).
Limitations
The major limitation of this study is the small sample of the population considered, that does not allow to make substantial observations.
The absence of an HF control group is also a main limitation, but the control group we evaluated had at least a normal LVEF.
Of note, we performed a 24 h PSG, which is an added value for the registration and evaluation of the data.
Conclusions
Our study seems to suggest that AHFpEF patients tend to have higher RDW values compared to a population of non-HF patients with similar LVEF, and that RDW could be a marker of inflammation and increase of pulmonary pressure in this population.
Additionally, our research might suggest that mechanisms underlying the increase in RDW, such as inflammation and oxidative stress, also cause desaturation in subjects affected by AHFpEF and SDB, showing the connection between RDW and both time and length of oxygen desaturation.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Ethical Committee Hospital Papa Giovanni XXIII. The patients/participants provided their written informed consent to participate in this study.
Author contributions
CS and ED'E: writing, editing, and conduction of the study. MG: revision. AC: statistical analysis. AG, CF, and MS: supervision. All authors contributed to the article and approved the submitted version.
Funding
A support for open access fee will be granted by Novartis Farma SpA in case of acceptance of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Lippi G, Cervellin G, Sanchis–Gomar F. Red blood cell distribution width and cardiovascular disorders Does it really matter which comes first, the chicken or the egg? Int J Cardiol. (2016) 206:129–30. doi: 10.1016/j.ijcard.2016.01.122
2. Lippi G, Cervellin G. Risk assessment of post–infarction heart failure. Systematic review on the role of emerging biomarkers. Crit Rev Clin Lab Sci. (2014) 51:13–29. doi: 10.3109/10408363.2013.863267
3. Imai R, Uemura Y, Okumura T, Takemoto K, Uchikawa T, Koyasu M, et al. Impact of red blood cell distribution width on non–cardiac mortality in patients with acute decompensated heart failure with preserved ejection fraction. J Cardiol. (2017) 70:591–7. doi: 10.1016/j.jjcc.2017.03.010
4. Javaheri S, Parker TJ, Liming JD, Corbett WS, Nishiyama H, Wexler L, et al. Sleep apnea in 81 ambulatory male patients with stable heart failure. Circulation. (1998) 97:2154–159. doi: 10.1161/01.CIR.97.21.2154
5. Jilek C, Krenn M, Sebah D, Obermeier R, Braune A, Kehl V, et al. Prognostic impact of sleep disordered breathing and its treatment in heart failure: an observational study. Eur J Heart Fail. (2011) 13:68–75. doi: 10.1093/eurjhf/hfq183
6. Somers VK, White DP, Amin R. Sleep apnea and cardiovascular disease: an American heart association/American college of cardiology foundation scientific statement from the American heart association council for high blood pressure research professional education committee, council on. Circulation. (2008) 118:1080–111. doi: 10.1161/CIRCULATIONAHA.107.189420
7. Tremel F, Pépin JL, Veale D, Wuyam B, Siché JP, Mallion JM, et al. High prevalence and persistence of sleep apnea in patients referred for acute left ventricular failure and medically treated over 2 months. Eur Hear J. (1999) 20:1201–209. doi: 10.1053/euhj.1999.1546
8. Herrscher TE, Akre H, Overland B, Sandvik L, Westheim AS. High prevalence of sleep apnea in heart failure outpatients: even in patients with preserved systolic function. J Card Fail. (2011) 17:420–5. doi: 10.1016/j.cardfail.2011.01.013
9. Bitter T, Faber L, Hering D, Langer C, Horstkotte D, Oldenburg O. Sleep–disordered breathing in heart failure with normal left ventricular ejection fraction. Eur J Heart Fail. (2009) 11:602–8. doi: 10.1093/eurjhf/hfp057
10. Sökücü SN, Karasulu L, Dalar L, Seyhan EC, Altin S. Can red blood cell distribution width predict severity of obstructive sleep apnea syndrome? J Clin Sleep Med. (2012) 8:521–5. doi: 10.5664/jcsm.2146
11. Bauersachs J, Soltani S. Guidelines of the ESC 2021 on heart failure. Herz. (2022) 47:12–8. doi: 10.1007/s00059-021-05084-5
12. Ruehland WR, Rochford PD, O'Donoghue FJ, Pierce RJ, Singh P, Thornton AT. The new AASM criteria for scoring hypopnea: impact on the apnea hypopnea index. Sleep. (2009) 32:150–7. doi: 10.1093/sleep/32.2.150
13. Tonelli M, Sacks F, Arnold M, Moye L, Davis B, Pfeffer M. Relation between red blood cell distribution width and cardiovascular event rate in people with coronary disease. Circulation. (2008) 117:163–8. doi: 10.1161/CIRCULATIONAHA.107.727545
14. Perlstein TS, Weuve J, Pfeffer MA, Beckman JA. Red blood cell distribution width and mortality risk in a community–based prospective cohort. Arch Intern Med. (2009) 169:588–94. doi: 10.1001/archinternmed.2009.55
15. Braun E, Domany E, Kenig Y, Mazor Y, Makhoul BF, Azzam ZS. Elevated red cell distribution width predicts poor outcome in young patients with community acquired pneumonia. Crit Care. (2011) 15:R194. doi: 10.1186/cc10355
16. Zorlu A, Bektasoglu G, Guven FM, Dogan OT, Gucuk E, Ege MR, et al. Usefulness of admission red cell distribution width as a predictor of early mortality in patients with acute pulmonary embolism. Am J Cardiol. (2012) 109:128–34. doi: 10.1016/j.amjcard.2011.08.015
17. Gori M, D'Elia E, Iorio A, Iacovoni A, Senni M. Clinical application of personalized medicine: heart failure with preserved left ventricular ejection fraction. Eur Heart J Suppl. (2020) 22(Suppl L):L124–8. doi: 10.1093/eurheartj/suaa151
18. Gori M, D'Elia E, Zambelli G, Senni M. Heart Failure with preserved ejection fraction: an update on diagnosis and treatment. G Ital Cardiol. (2020) 21:119–27.
19. Senni M, Paulus WJ, Gavazzi A, Fraser AG, Díez J, Solomon SD, et al. New strategies for heart failure with preserved ejection fraction: the importance of targeted therapies for heart failure phenotypes. Eur Heart J. (2014) 35:2797–815. doi: 10.1093/eurheartj/ehu204
20. Ryan S, Taylor CT, McNicholas WT. Systemic inflammation: a key factor in the pathogenesis of cardiovascular complications in obstructive sleep apnoea syndrome? Thorax. (2009) 64:631–6. doi: 10.1136/thx.2008.105577
21. Sánchez–de–la–Torre M, Barbé F. What treatment wins in the battle against sleepiness? Lancet Respir Med. (2015) 3:828–9. doi: 10.1016/S2213-2600(15)00455-5
22. Shirazi LF, Bissett J, Romeo F, Mehta JL. Role of inflammation in heart failure. Curr Atheroscler Rep. (2017) 19:27. doi: 10.1007/s11883-017-0660-3
23. Lippi G, Targher G, Montagnana M, Salvagno GL, Zoppini G, Guidi GC. Relation between red blood cell distribution width and inflammatory biomarkers in a large cohort of unselected outpatients. Arch Pathol Lab Med. (2009) 133:628–32. doi: 10.5858/133.4.628
24. Tsutsui H, Kinugawa S, Matsushima S. Oxidative stress and heart failure. Am J Physiol Heart Circ Physiol. (2011) 301:H2181–90. doi: 10.1152/ajpheart.00554.2011
25. Friedman JS, Lopez MF, Fleming MD, Rivera A, Martin FM, Welsh ML, et al. SOD2–deficiency anemia: protein oxidation and altered protein expression reveal targets of damage, stress response, and antioxidant responsiveness. Blood. (2004) 104:2565–573. doi: 10.1182/blood-2003-11-3858
26. Aslinia F, Mazza JJ, Yale SH. Megaloblastic anemia and other causes of macrocytosis. Clin Med Res. (2006) 4:236–41. doi: 10.3121/cmr.4.3.236
27. Sciatti E, Lombardi C, Ravera A, Vizzardi E, Bonadei I, Carubelli V, et al. Nutritional deficiency in patients with heart failure. Nutrients. (2016) 8:pii E442. doi: 10.3390/nu8070442
28. Koller L, Kleber M, Goliasch G, Sulzgruber P, Scharnagl H, Silbernagel G, et al. C–reactive protein predicts mortality in patients with referred for coronary angiography and symptoms of heart failure with preserved ejection fraction. Eur J Heart Fail. (2014) 16:758–66. doi: 10.1002/ejhf.104
29. Manzano-Fernandez S, Mueller T, Pascual-Figal D, Truong QA, Januzzi JL. Usefulness of soluble concentrations of interleukin family member ST2 as predictor of mortality in patients with acutely decompensated heart failure relative to left ventricular ejection fraction. Am J Cardiol. (2011) 107:259–67. doi: 10.1016/j.amjcard.2010.09.011
Keywords: sleep apnea, red distribution width, oxygen saturation, acute heart failure, heart failure with preserved ejection fraction (HFpEF)
Citation: Stamerra CA, D'Elia E, Gori M, Roncali F, Cereda A, Gavazzi A, Ferri C and Senni M (2023) Red cell distribution width (RDW) is correlated to time of oxygen desaturation < 90% and length of sleep apneas in patients with sleep disorder breathing (SDB) and acute heart failure with preserved ejection fraction (HFpEF). Front. Cardiovasc. Med. 10:1045702. doi: 10.3389/fcvm.2023.1045702
Received: 15 September 2022; Accepted: 09 January 2023;
Published: 03 February 2023.
Edited by:
Matteo Cameli, University of Siena, ItalyReviewed by:
Guido Pastorini, Regina Montis Regalis Hospital, ItalyMauro Feola, Regina Montis Regalis Hospital, Italy
Copyright © 2023 Stamerra, D'Elia, Gori, Roncali, Cereda, Gavazzi, Ferri and Senni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emilia D'Elia,  edelia@asst-pg23.it
edelia@asst-pg23.it
†These authors share first authorship